
Abstract
Objective:
To examine racial/ethnic disparities in severe maternal morbidity (SMM) and adverse pregnancy outcomes (APOs) among pregnant patients with substance use disorder (SUD) compared to individuals without SUD.
Materials and Methods:
We conducted a cross-sectional analysis of inpatient hospitalizations of pregnant people from the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS) from 2016 to 2019. ICD-10 codes were used to identify the frequency of SMM and/or APO between those with and without SUD by race/ethnicity. Multilevel logistic regression analyses were performed to identify the effect of race/ethnicity as an independent predictor and as an effect modifier of SMM and APO in patients with SUD.
Results:
From 2,508,259 hospitalizations, SUD was identified in 6.7% admissions with the highest rate in White patients (8.2%) followed by Black (7.7%) and Hispanic (2.2%) patients. Rate of SMM and APO were increased in patients with SUD in all racial/ethnic groups compared to those without SUD, increasing by 1% and 10%, respectively. Among all patients, Black race was an independent predictor of SMM (adjusted odds ratio [aOR] 2.09; 95% confidence interval [CI]: 2.05–2.13) and APO (aOR 1.58; 95% CI: 1.56–1.59). Hispanic ethnicity was also an independent risk factor for predicting SMM (aOR 1.40; 95% CI: 1.37–1.43). Among Hispanic patients, SUD was associated with an ∼90% increased likelihood of SMM and APO.
Conclusion:
Although higher rates of SMM and APO are seen among hospitalizations of pregnant people with SUD, racial/ethnic disparities also exist among this population. This warrants further attention and presents an opportunity for intervention and for addressing the root causes of racial and ethnic disparities.
Introduction
Substance Use Disorder (SUD) is a chronic condition that is a combination of cognitive, behavioral, and physiological symptoms with substance use, in which an individual continues using the substance despite its negative effects. 1 SUD has been an expanding challenge in health care, including pregnancy-related care. It is estimated that over 17 million individuals older than the age of 18 years struggled with SUD in 2020, including addictive use of alcohol, marijuana, tobacco, or illicit drugs, and between 8% and 11% of pregnant women have used illicit drugs, marijuana, tobacco, or alcohol in the past month. 2 Substance use has been shown to have detrimental effects on nearly all areas of pregnancy, maternal, and fetal outcomes, including increased preterm birth (PTB), low birth rate, fetal anomalies, neonatal abstinence syndrome, inadequate prenatal care, and malnourishment. 3 –5
There has been limited emphasis on the impact of racial/ethnic disparities in pregnancy outcomes, specifically in the context of SUD in pregnancy. The prevalence of SUD across the population may vary across racial/ethnic groups according to the 2020 National Survey of Drug Use and Health (NSDUH) with Asian and Hispanic individuals having the lowest rates of SUD, in contrast to higher rates of use in Black and highest use in White individuals; however, these data notes overlap confidence intervals (CIs), therefore, large apparent differences may not necessarily yield statistical significance. 6 Disparities in the diagnosis and treatment offered, received, and completed for substance use in pregnancy between racial/ethnic groups have also been noted in prior studies.
Examples of disparities studied include differences in the types of medications prescribed, differences in when drug tests were performed and Child Protective Service reporting, and the differences that socioeconomic factors and race play in completion of substance treatment. 7 –12 As these problems have been identified, the drive to address these perinatal health disparities has been palpable over the last decade. 13 –17
Severe maternal morbidity (SMM) is overall increasing in the United States, and we know that increase in substance use is one factor leading to this continued increase. 18 Our study aims to better understand how race/ethnicity and SUD relate to SMM and adverse pregnancy outcome (APO). Pregnancy, maternal, and obstetrical outcomes have previously been shown to vary by race/ethnicity, despite adjusting for socioeconomic factors and patient characteristics. 13,14 In addition, some of the most significant racial/ethnic disparities in SMM are noted among women with complex medical or behavioral comorbidities, including pregnancies complicated by substance use and the negative impact of this use. 19 –21 The objective of this study was to examine racial/ethnic disparities in SMM and APOs among pregnant patients with SUD in comparison to individuals without SUD.
Materials and Methods
We performed a cross-sectional analysis of the Healthcare Cost and Utilization Project (HCUP) National Inpatient Sample (NIS), the largest publicly available all-payer database in the United States. This study used the 2016 through 2019 NIS datasets. The years of study were specifically chosen after the implementation of ICD-10 and the resultant transition from ICD-9 to ICD-10 as an attempt to avoid inaccuracies in the conversion from ICD-9 to ICD-10 that would have occurred upon expanding the dataset to NIS data before 2016. Hospital admissions were identified using ICD-10 diagnosis and procedure codes pertaining to an ongoing pregnancy. ICD-10 codes were also used to determine SMM or APO diagnoses (Supplementary Appendix Table SA1).
The sample was limited to Black, Hispanic, and White racial/ethnic groups given small sample size of additional race/ethnicity groups. Moreover, patients were categorized into a group who had a diagnosis code indicating SUD versus others without this diagnosis. Substance use exposure was defined as a composite between alcohol, tobacco, cannabis, cocaine, sedatives, opioids, hallucinogens, and stimulant use disorder.
In the HCUP NIS database, race/ethnicity variables are provided by HCUP Partner organizations. Race and/or ethnicity are transcribed as a single uniform variable of “race” in the overall database. In some organizations, Hispanic ethnicity is provided as a variable of race, whereas in others, Hispanic ethnicity is provided as a separate variable. Given these variations in the data provided by partnering organizations, the HCUP NIS database is constructed to allow ethnicity to take precedence over race in the setting of uniform variables. For example, a patient who is Hispanic and Black is assigned to the category of Hispanic. Not all HCUP partner organizations provide information regarding race/ethnicity that goes into the national database. 22
Within the NIS data, “race” is composed of race/ethnicity descriptors with options for White, Black, Hispanic, Asian or Pacific Islander, Native American, Other, Missing, or Invalid. This also prohibits an individual from identifying as multiple races/ethnicities. We are therefore also unable to segregate individuals who may have identified themselves for instance, as Hispanic Black versus non-Hispanic Black.
Our primary outcomes of interest were SMM—structured as a composite using the CDC defined list of conditions (and applicable diagnosis codes) 23 and APO—defined as a composite, including hypertensive disorders of pregnancy (HDP), antepartum hemorrhage (AH), postpartum hemorrhage (PPH), PTB, and fetal growth restriction (FGR). Rates of substance use, SMM, and APO were calculated across the entire cohort of inpatient hospitalizations of pregnant people from 2016 to 2019, and further stratified based on racial/ethnic categories under consideration.
Analysis was performed on the entire population of hospitalizations of pregnant patients to provide a foundation of continued comparison of a subset analysis of individual cohorts. All hospitalizations of pregnant patients were analyzed first to assess the differences in SMM and APO by cohorts of race/ethnicity. We then controlled for sociodemographic factors to assess whether race/ethnicity impacted the likeliness of a cohort to experience an SMM or APO. Hospitalizations of pregnant patients were then examined to assess differences in rates of SMM and APO in patients with SUD versus to those without SUD. Finally, we identified whether race/ethnicity was a predicting factor for a pregnant patient experiencing an SMM or APO, and whether the presence of an SUD within these cohorts effects these odds.
We adopted the World Health Organization (WHO) Commission on Social Determinants of Health (CSDH) Conceptual Framework as the principal guiding framework in our approach to analyzing the overlay of race/ethnicity, substance use, and pregnancy outcomes. 24 In brief, the WHO CSDH demonstrates how social, economic, and political mechanisms give rise to a set of “socioeconomic positions,” whereby populations are stratified according to income, education, occupation, gender, race/ethnicity, and other factors; these “socioeconomic positions” in turn shape specific determinants of health status based on their respective social status. 24 Thereby, individual experiences differ in exposure and vulnerability to health-compromising conditions. Some of the most important structural stratifiers and their proxy indicators as outlined in the WHO CSDH framework include income, education, occupation, social class, gender, race, and ethnicity. 24
While we were unable to incorporate all the “structural determinants” and “social determinants” from the WHO CSDH framework due to limitations posed by available relevant sociodemographic variables in the HCUP NIS database, several of the covariates included in our multilevel comparisons and regression analyses are rooted in their relevance and mechanistic contribution as social determinants of health, with the goal of examining how these interact to influence inequities in pregnancy outcomes. 24 More specifically, the HCUP NIS database allowed us to evaluate insurance payer, patient's zip code, race/ethnicity, hospital location, type, and size. These determinants were used as proxies to the structural and social determinants identified in the WHO CSDH framework.
Pregnancy-related hospitalization rates were reported overall and by race/ethnicity. Hospital admission rates for the whole sample and each outcome level were computed by race/ethnicity across age, insurance payer (governmental, private, other, and missing), median household income for patient's ZIP code, and year of the cohort. Hospital characteristics, including hospital region, urban-rural location, bed size, and teaching status, were also included in this analysis.
Survey-weighted proportions were computed for variables of interest in the whole sample and stratified by race/ethnicity and substance use status (i.e., ± substance use exposure). Rao Scott chi-Square tests were used to compare the distribution of patients across the levels of the exposure. Multilevel logistic regression analyses were used to identify the crude and adjusted odds ratios (aORs) and associated 95% CIs of the patient characteristics influencing the study outcomes within each racial/ethnic group. Regression analyses were undertaken identifying the effect of race/ethnicity as an independent predictor and an effect modifier of the study outcomes. Discharge weights, developed using the American Hospital Association (AHA) universe, were used to provide the national estimates. 25 Statistics were computed using SAS 9.4 (SAS Institute, Inc., Cary, NC). The NIS database is entirely de-identified and hence, this research project was deemed exempt by our IRB.
Results
From 2016 to 2019, 2,508,259 inpatient hospitalizations of pregnant people were identified in the NIS database. Distribution of hospitalizations of pregnant people were balanced overall between the 4 years being evaluated. Within the inpatient admissions overall, 17.2% (N = 431,753) patients identified as Black, 23.3% (N = 585,605) as Hispanic, and 59.4% (N = 1,490,901) as White. SUD was identified in 6.7% (N = 168,779) admissions. Identified SUD included 61.2% (N = 103,246) of patients with a SUD of a single substance, whereas 38.8% (N = 65,533) had co-occurring substance use. Substance types identified were tobacco (72.9%, N = 123,119), cannabis (22.7%, N = 38,328), opioids (12.3%, N = 20,741), stimulants (5.4%, N = 9145), cocaine (3.1%, N = 5153), alcohol (2.2%, N = 3636), sedatives (0.5%, N = 923), hallucinogens (0.1%, N = 177), and other illicit substances (40.5%, N = 68,319).
SUD was identified with the highest rate in White patients at 8.2% (N = 122,522) followed by Black patients at 7.7% (N = 33,320) and Hispanic patients at 2.2% (N = 12,927). Other race/ethnicities included in the NIS database were not included in our study cohort, due to their small sample sizes—especially for individuals with substance use, thus leading to the exclusion of Asian or Pacific Islander (N = 1854, 1.0%), Native American (N = 3221, 1.8%), and other races (N = 3830, 2.2%) from the analyses. Hospitalizations among all groups were predominantly between the ages of 20–40. Hospitalizations among White patients had significantly higher rates of private insurance at 63.8% (N = 949,236), whereas hospitalizations among Black and Hispanic individuals were notable for higher rates of governmental insurance, 64.6% (N = 278,513) and 63.0% (N = 368,805), respectively.
Among Black pregnant patients, 49.4% (N = 211,470) had household incomes in the lowest income quartile, compared with 35.6% (N = 206,519) of Hispanic patients and 21.5% (N = 318,380) of White patients. Our cohort predominantly included pregnant people hospitalized from the Southern states, 26 in large, urban, and teaching hospitals 27,28 with admissions consistent across all race/ethnicity groups (Supplementary Appendix Table SA2). Demographic characteristics for the subset of hospitalizations among pregnant patients with an SUD diagnosis are presented in Table 1. In brief, hospitalizations with SUD were predominantly aged 20–30 years, with governmental insurance, in the lowest income level, and most often in the Southern region at large, urban teaching hospitals.
Patient Demographics of Pregnancy-Related Hospitalizations with Substance Use Disorder
Differences by race and ethnicity were statistically significant at p < 0.001 for all characteristics.
Among hospitalizations of pregnant people overall, SMM was identified in 2% (N = 51,784) of encounters (Supplementary Appendix Table SA3). SMM occurrences were driven by blood transfusion, followed by sepsis, disseminated intravascular coagulation (DIC), eclampsia, and acute renal failure. In the comparison across hospitalizations of pregnant people with and without SUD—rate of SMM was increased in individuals with SUD at 3.1% (N = 5218/168,779) compared to those without SUD at 2.0% (N = 46,566/2,339,480, p < 0.001). All types of SMM were also significantly increased in individuals with SUD except for rates of amniotic fluid embolism (p = 0.079), DIC (p = 0.117), heart failure or arrest during surgery (p = 0.332), and temporary tracheostomy (p = 0.070).
APO—as defined by our prespecified composite were identified in 27.4% (N = 686,943) of encounters overall. APOs most commonly identified were—HDP in 14.5% (N = 364,201) and PTB in 10.8% (N = 29,173) of encounters. Rates of APOs were increased among individuals with SUD at 36.9% (N = 62,211/168,779) compared to those without SUD at 26.7% (N = 624,732/2,339,480, p < 0.001). Significantly increased rates of HDP, AH, PTB, and FGR were seen in pregnancy-related hospitalization with SUD (all p < 0.001) (Supplementary Appendix Table SA3).
In the analyses of SMM and APO rates across race/ethnicity encounters with individuals of Black race had the highest rate of SMM at 3.4% (N = 14,513) compared to those with individuals of Hispanic ethnicity at 2.2% (N = 12,970) and White race at 1.6% (N = 24,301). Rates were significantly different (p < 0.05) in all individual SMM categories except for aneurysm occurrence (p = 0.983). Similarly, APO rates were significantly higher in hospitalizations of Black individuals at 35.7% (N = 154,085) compared to Hispanic individuals at 25.1% (N = 154,085) or White individuals at 25.9% (N = 386,008). Rates of all individual APO categories were also significantly higher in clinical encounters that comprised Black patients (Table 2).
Rates of Severe Maternal Morbidity and Adverse Pregnancy Outcomes in Hospitalizations of Pregnant Patients comparing Race and Ethnicity
In a subset of hospitalizations among pregnant patients with an SUD diagnosis—composite rate of SMM was increased in the Black (4.7%, N = 1551/33,320) and Hispanic (4.2%, N = 546/12,937) cohorts compared to the White cohort (2.5%, N = 3121/122,522) (Table 3). Likewise, among inpatient hospitalizations of pregnant patients with SUD—rate of our APO composite was highest among Black (45.7%, N = 15,232/33,320) patients compared to their Hispanic (38.7%, N = 5002/12,937) and White (34.3%, N = 41,977/122,522) counterparts (Table 3).
Rates of Severe Maternal Morbidity and Adverse Pregnancy Outcomes in Hospitalizations of Pregnant Patients with Substance Use Disorder Comparing Race and Ethnicity
ARDS, adult respiratory distress syndrome.
Multivariable regression analyses noted race/ethnicity classification to be an independent predictor of both SMM and APO, as noted in Table 4. More specifically, identifying as a Black pregnant patient was an independent predictor of SMM and APO in pregnancy-related hospitalizations with aOR 2.09 (2.05–2.13) and 1.58 (1.56–1.59), respectively, when compared to White individuals. Identifying as Hispanic was also an independent risk factor, although with a weaker association, for predicting SMM with an aOR 1.40 (1.37–1.43) (Table 4).
Role of Race and Ethnicity as Predictors of Severe Maternal Morbidity and Adverse Pregnancy Outcome
Confounding variables controlled for: SUD, age, income, and insurance.
aOR, adjusted odds ratio; CI, confidence interval; cOR, crude odds ratio; LL, lower limit; SUD, substance use disorder; UL, upper limit.
Predictors of SMM were stratified by race/ethnicity and are presented in Figure 1. Hospitalizations with SUD had a higher rate of SMM in all racial/ethnic groups, however, the strength of the association was most pronounced among Hispanic individuals (aOR 1.90, 1.73–2.07), while adjusting for age, insurance status, and income. While evaluating the impact of other predictors within each racial/ethnic stratum, it was noted that the risk for SMM increased with age, nonprivate (governmental) insurance, and for low-income groups (Fig. 1 and Supplementary Appendix Table SA4).
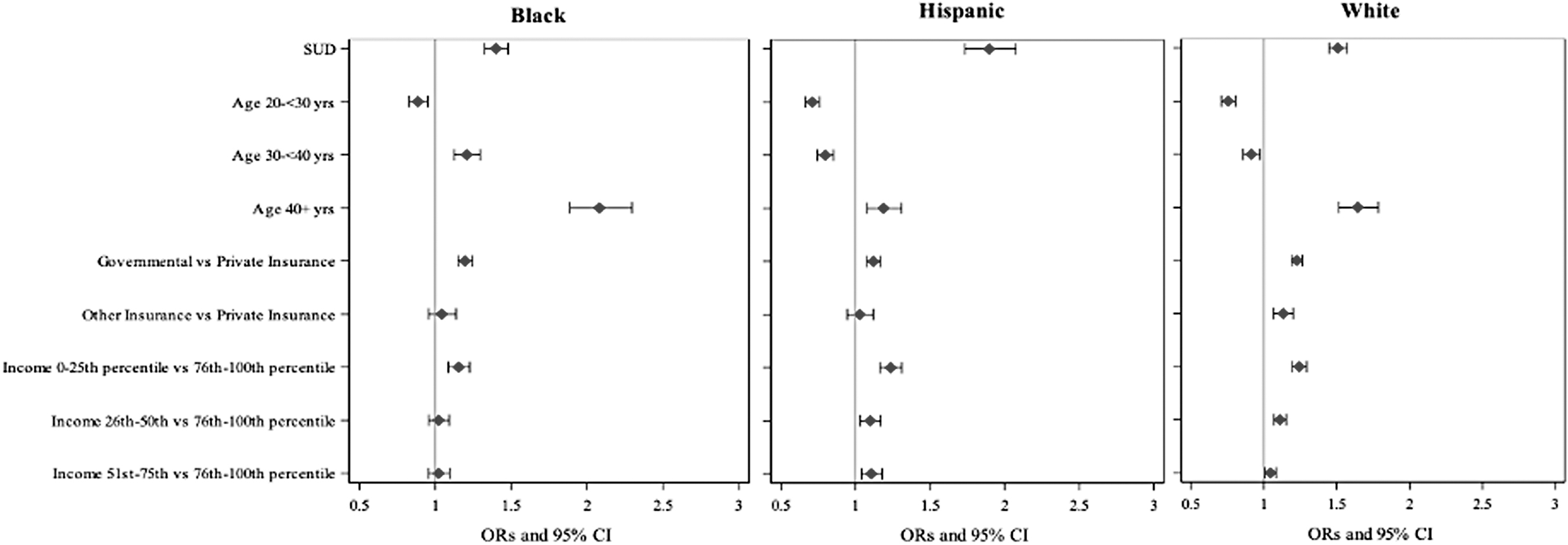
Shows sociodemographic predictors of severe maternal morbidity stratified by race/ethnicity.
Predictors of APO were also stratified by race/ethnicity and are presented in Figure 2. Comparable to SMM, hospitalizations with SUD were associated with increased odds of APOs in all racial/ethnic groups with the strongest association seen among hospitalizations with SUD among Hispanic patients, (aOR 1.91, 1.84–1.98), while adjusting for age, insurance status, and income. Again, within each racial/ethnic stratum—risk for APO was noted to increase with age, governmental insurance, and for the lowest income groups (Fig. 2 and Supplementary Appendix Table SA5).
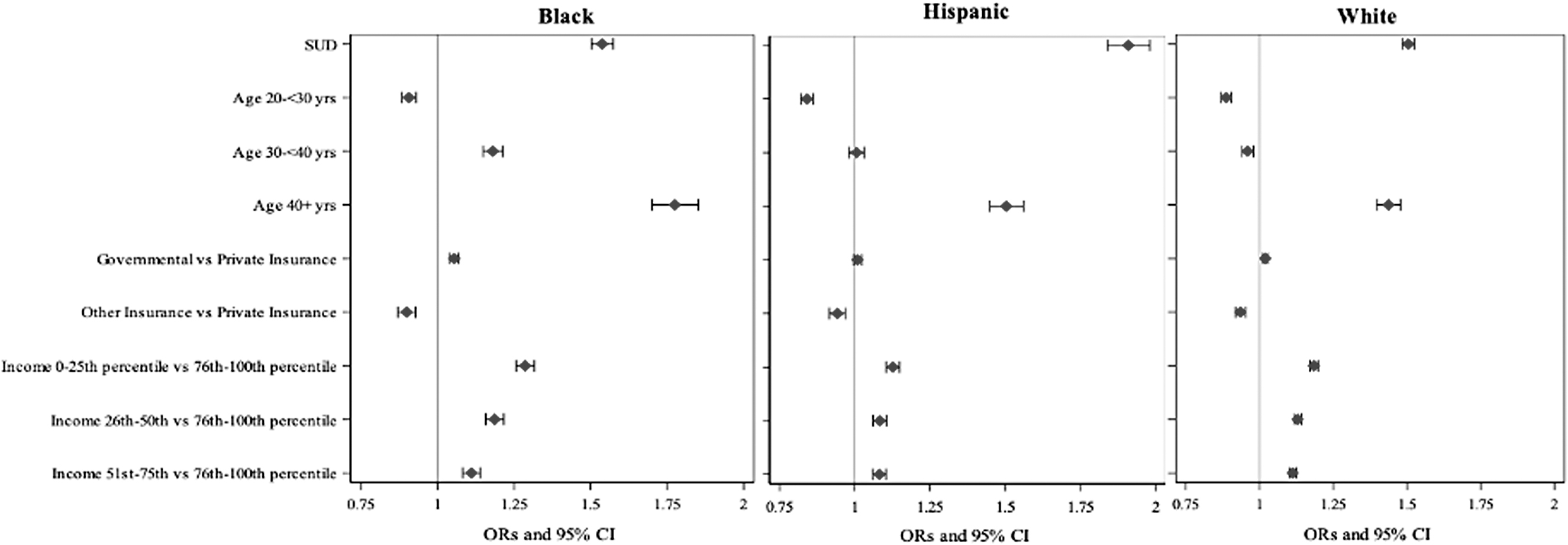
Shows sociodemographic predictors of adverse pregnancy outcome stratified by race/ethnicity.
Discussion
In this nationally representative study on the association of race/ethnicity, SUD, and pregnancy outcomes, we found race/ethnicity to be an independent predictor of SMM and APO, and the impact differed between racial/ethnic groups. In over 2.5 million pregnancy admissions, rates of SMM and APO were significantly higher in hospitalizations affected by SUD and highest among hospitalizations involving Black patients. In subgroup analyses of hospitalizations among pregnant patients with an SUD diagnosis, rates of SMM and APO were highest among Black individuals, followed by those with a Hispanic ethnicity. The results from the crude and aOR estimates evaluating the impact of race show very little difference, indicating the role of race as an independent predictor of both SMM and APO.
Black race was noted to be an independent predictor of SMM and APO in cohort overall. However, in stratified analyses based on racial/ethnic categorization, the strength of association between race and SUD on SMM was the weakest for Black individuals. This suggests that the high rates of SMM among Black patients may not be attributable to SUD alone. In contrast, hospitalizations among Hispanic patients had the lowest rates of SUD exposure, but with the strongest association in the relationship between SUD as a predictor for both SMM and APO in the stratified analyses based on racial/ethnic categorization.
Our study affirms prior evidence demonstrating disparities between race/ethnicity on APO. 13 –16 Consistently, White pregnant patients have been noted to have lower adverse maternal, fetal outcomes, and less pregnancy complications. 13 –16 Our findings echo these previous observations and are in congruence. Differences in rates of maternal morbidity and adverse outcomes based on race/ethnicity have previously been shown to not be explained by other patient characteristics, hospital location, or sociodemographic factors. 14 We found comparable trends in the predictive value of age, insurance type, and income level on outcomes between race/ethnicity.
Our study adds to the existing literature on the impact of racial/ethnic disparities on pregnancy outcomes, by specifically factoring a key consideration—that is, SUD in pregnancy. Notably, our results show that even though rates of SUD were lower among Hispanic patients overall, this select subset was at a higher risk for SMM and APOs—thus identifying a unique at-risk cohort. One prior study using Medicaid data showed that women of minority groups (Hispanic, Black, Asian, American Indian or Alaska Native, Native Hawaiian or other Pacific Islander) are diagnosed with opioid use disorder (OUD) later in pregnancy than non-Hispanic White women, leading to the largest contributor of racial/ethnic disparity in treatment with medication for OUD.
This study, however, was flawed in that it may have overestimated SUD diagnosis given timeframe of gestation recorded. 7 Given the racial/ethnic disparities in SUD treatment, Hispanic women have been found to be less likely to have access or use medication for treatment of OUD and less likely to complete treatment programs during pregnancy compared to White counterparts. 8,11 We must take into account barriers in care, including but not limited to language barriers, health insurance access, cultural beliefs related to health care, and general access to care within the community. Addressing inequities in the care of SUD among Hispanic pregnant patients has the potential to improve pregnancy outcomes in this population and, therefore, decrease the gap posed by racial/ethnic disparities and SUD on pregnancy outcomes.
Similarly, hospitalizations among Black patients were notable for almost twice the rate of SMM and a considerably higher rate of APO compared to White patients. This underscores the importance of other factors within our communities, health systems, and public policies as drivers of APO experienced by Black pregnant patients. Our work emphasizes the need for addressing health inequities and racial/ethnic disparities at higher levels of policy making, community advocacy, and culture change in the approach to mitigating the impact of social inequities on health outcomes.
This study had several limitations, most of which are inherent to utilizing a pre-existing national database. Our study cohort similarly is composed of all inpatient hospitalizations in the context of an ongoing pregnancy. This includes inpatient hospitalizations that may or may not have been related to a birthing or delivery encounter. Our dataset captures hospitalizations that occur in the context of a delivery episode but may also include some of the inpatient hospitalizations in the antepartum period. In addition, the NIS provides the strength of a national sample which allows proper evaluation of race/ethnicity outside of a community or at the hospital level. However, we are unable to confirm or prevent inaccuracies in variable coding at the institution level.
Given limited sample sizes involved, we were unable to include other races, including Asian or Pacific Islander, Native American, or other race/ethnicity groups that may also disproportionately experience SUD. Coding of race/ethnicity within the NIS is also particularly subject to errors especially given inclusion of data that only report one or the other. 29 We recognize that race and ethnicity are two distinct categories with inherent differences which limit our ability to fully understand the impact between race and ethnicity with this data. Our study focuses on SUD as a whole within this framework of assessment, thereby limiting to some extent what can be understood about each individual type of substance exposure. The rationale for adhering to SUD as a composite exposure and also a study strength therefore stems from the finding that many people with SUD use multiple substances.
ICD-10 codes were used for identification of the exposures and outcomes of interest—that is, pregnant women with SUD and those who experiences APOs and SMM. Therefore—the definitions of SUD, APO, and SMM used for this study are inherently contingent upon data interpretation and abstraction from electronic medical records and application of the appropriate ICD-10 codes. We are therefore unable to comment on urine toxicology testing or clinical patterns of substance use in our study cohort, and as such, the focus of our work was to understand the impact of SUDs rather than sporadic instances of illicit substance use as detected by drug screening. ICD-10 codes within these pregnancy-related admissions cannot distinguish between etiology, timing, and misclassification of events.
Events may also be missed using this method. ICD-10 codes also limit our ability to distinguish between true SUD versus sporadic substance use, which is an inherent limitation of our study. We aimed to choose ICD-10 codes which would be the most inclusive to identify and encompass all individuals impacted by SUD. Finally, as noted previously, data and findings pertaining to types of SMM with rare occurrences may be less accurate given the small sample size for evaluation within these groups. We also acknowledge that we were limited by the data available in the NIS database which pertains to adult inpatient hospitalizations, and therefore does not provide infant neonatal data for an understanding of neonatal outcomes, including neonatal abstinence syndrome.
Our research has identified and described disparities in SMM and APOs at the intersection and complex overlay of race/ethnicity and SUD in pregnancy. While our work was focused on elucidating the impact of racial/ethnic disparities on perinatal outcomes in the context of SUDs, we acknowledge that the contribution is largely multifactorial with a collective impact from diverse factors beyond race/ethnicity alone, in the realm of social determinants of health and disease. Our work calls for the need to swim upstream in identifying and addressing individual, interpersonal, societal, and systems level determinants that can alter the course of pregnancy outcomes among women with SUDs. 30,31 Substance use programs during pregnancy that provide improved access to medications for OUD, counseling, and case management have been shown to result in improved perinatal outcomes. 32
Our findings call for the need to recognize disparities not only at the level of clinician-patient relationship, but at the broader health-system level, and emphasize the need to adopt a health equity lens for developing interventions and affecting change.
Footnotes
Authors' Contributions
A.S.R.: conceptualization and writing—original draft preparation. N.A.-H.: conceptualization, methodology, formal analysis, and visualization. S.B.: methodology and investigation. N.R.C.: supervision, conceptualization, and writing—review and editing.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This work is supported through the “Big Ideas” grant from the Saint Louis University Research Institute through research support services from the AHEAD institute.
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Table SA4
Supplementary Appendix Table SA5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.