
Abstract
African American women suffer under the burden of cervical cancer as they are first in mortality, diagnosed at later stages, and have a survivorship rate that is lower than the national average. The aim of our review is to evaluate the effectiveness of cervical cancer screening and prevention interventions for African American women living in the United States and to assess their commitment to health equity. A literature search was conducted using PubMed, Embase, CINAHL, and Scopus using MeSH terms related to cervical cancer, human papillomavirus (HPV), screening and prevention, and African Americans. This resulted in 1970 articles. Studies were included if they promoted cervical screening or prevention, sampled African American women aged 18 and over, and evaluated interventions. Among the 23 articles that met inclusion criteria, there were a wide variety of intervention strategies, that is, community health workers, patient navigation, patient reminders, self-sampling collection, and HPV vaccination. Health education interventions, when coupled with patient navigation or community health workers, were effective in promoting screening participation (odds ratio: 2.43, 95% confidence interval: 1.47–4.02). There were mixed results regarding the incorporation of health equity principles. This review supports the importance of incorporating health equity principles and community based methods in screening and prevention interventions. Future research and practice should incorporate African American women's perspectives in intervention development and implementation.
Introduction
Cervical cancer treatment and prevention has improved over the past few decades, as basic sciences, policy, and screening work toward the elimination of the disease. 1 In the United States in 2023, an estimated 13,900 women will be diagnosed with cervical cancer and 4,310 will die from the disease. 2 Incidence and mortality has been trending downward over the years, with a 54% decrease between 1973 and 2007. 3,4
Unfortunately, not every racial and ethnic group has experienced these improvements. Inequities exist for African American women who rank third overall in incidence and first in mortality compared with other racial and ethnic groups. 2 African American women are more likely to be diagnosed at advanced stages of the disease compared with other groups, 2 and with White women in particular. 5
In addition to being diagnosed at later stages of the disease, the 5-year survivorship rate for African American women is poor: 56% compared with the 67% national average. 2 Depending on the region, there are even treatment disparities between African American and White American cervical cancer patients, with African American women receiving less aggressive treatment options. 6
Screening and prevention are critically important to promoting early detection and improving survivorship outcomes. African American women experience barriers to screening that potentially explain the inequities in incidence and mortality. Examples of these are lack of health insurance and cost, 7 lack of knowledge and awareness about cervical cancer screening, 8 and past negative experiences in the health care system including medical trauma. 9
Although a high percentage of African American women report having had a Pap smear test within the past year, 10 there is a potential for over- and under-reporting. 11 –13 In general, there is a discrepancy between self-reported cervical cancer screening and medical record documentation, with an estimated 39%–52% of under screened women over-reporting their most recent screening history. 14
One of the benefits of cervical cancer screening programs is the reduction in new cervical cancer cases and related deaths. 15 Intervention strategies have focused on increasing Pap smear uptake and human papillomavirus (HPV) vaccination. 16,17 These strategies have ranged from targeting African American women solely, to using community-based methods, and tailored interventions with varying levels of success.
It is important to assess cervical cancer screening and prevention interventions not only for their effectiveness in promoting health behavior change but also in their commitment to health equity. Health equity “is the principle underlying a commitment to reduce—and, ultimately, eliminate—disparities in health and in its determinants. Pursuing health equity means striving for the highest possible standard of health for all people and giving special attention to the needs of those at the greatest risk of poor health, based on social conditions.” 18 Here, we use a health equity focus to center the experiences of African American women and recognize the impact of racism on cervical cancer screening and prevention.
The purpose of our review is to evaluate the effectiveness of cervical cancer screening interventions for African American women, and to assess their attention to health equity. We aim at (1) describing the characteristics of screening and prevention interventions that target African American women, (2) comparing the effectiveness of these interventions, and (3) determining whether these studies address health equity factors.
Methods
This review's protocol was registered with PROSPERO and can be found at: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=210691 It was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement Equity 2012 Extension. 19
Search strategy
We conducted an electronic search of PubMed, Embase, CINAHL, and Scopus databases from inception to November 2023. Each database was searched using the same MeSH terms related to these terms: cervical cancer, cervical cancer screening, cervical cancer prevention, Pap smear, Pap smear test, HPV, African American women, Black Women, intervention, and psychosocial interventions. Search strings for each database are available in the Supplementary Data.
In addition to searching electronic databases, the reference sections of the included studies, along with relevant systematic reviews, were searched for additional articles that may fit the inclusion criteria.
After eligible studies had been identified, they were uploaded to Rayyan, a web-based tool for systematic review collaboration. Two reviewers independently assessed titles and abstracts for eligibility and then evaluated the full text articles for inclusion. Any disagreements were discussed until a consensus was reached between the two reviewers.
Eligibility criteria
Inclusion criteria included: (1) primary aim to promote cervical cancer screening and prevention, (2) at least one-third of sample was African American women, (3) participants were age 18 and older, (4) English language, and (5) used a randomized control trial, quasi-experimental, or non-experimental design to evaluate an intervention.
Articles were excluded if they did not have a sufficient sample of one-third or more African American women, were descriptive studies, or did not promote cervical cancer screening and prevention intervention strategies.
Data extraction
A data extraction sheet was developed and piloted by the reviewers. Data extracted were patient characteristics, theoretical frameworks (such as Social Determinants of Health, Health Belief Model, and Theory of Planned Behavior), intervention setting, data collection methods (self-report vs. medical record review), intervention design and duration, intervention provider, measures of interest, and intervention outcomes.
Measures of health equity and quality assessment
To assess study quality, the reviewers used the Quality Assessment Tool for Reviewing Studies with Diverse Designs (QATSDD), which facilitates uniform assessment across differing study designs. QATSDD domains include: description and rationale of data collection tools, fit between stated research question and method of data collection quantitative methods, description of recruitment strategy, fit between research question and method of analysis, justification for analytical method selected, user involvement in intervention or study design, and critical assessment of study's strengths and limitations. Scores for each domain range from 0 (not at all) to 3 (complete), where higher scores indicate higher quality.
In addition to the reviewer-developed data extraction sheet, the authors used CONSORT-Equity 2017, an extension of CONSORT 2010, to extract information related to health equity. The CONSORT-Equity 2017 extension aims at improving reporting on intervention trials where health equity is relevant due to participants experiencing social disadvantage. 20
CONSORT-Equity 2017 provides health equity reporting standards that include information about place of residence, social capital, socioeconomic status, and whether studies included health equity in their rationale, design, and intervention. Studies were rated yes, no, or partial according to whether they met each standard. A score was assigned for each item with yes equaling 1-point, no equaling zero points, and partial equaling 0.5 points. The score reported in Table 2 is the sum of the items.
Addressing root causes of health inequities
In addition to the CONSORT-Equity 2017 extension, we drew on the Healing ARC framework 21 and Ford's Public Health Critical Race (PHCR) praxis 22 to inform further questions to assess commitment to health equity. These questions include: (1) Does the study acknowledge the impact of racism on health and use of preventative services, (2) does the study redress the previous harm done to the priority population through the use of restitution, (3) does the study describe key characteristics of societal racialization for its time period, (4) does the study acknowledge and attempt to address how racialization may shape a project and how knowledge is constructed throughout the study, and (5) do the researchers use the knowledge gained to take action to address inequities?
Meta-analysis
Using the dichotomous outcome of adherence to Pap smear screening or not, a meta-analysis was conducted on studies, where appropriate. Data were extracted from the studies based on the number of women who were either self-reported or through medical record review deemed to be adherent to screening guidelines. In addition to the systematic review, we performed a meta-analysis with studies that provided data comparing adherence to Pap smear screening in an intervention group versus a control group or usual care group.
We then used SPSS 28 to calculate the odds ratio (OR) and overall effect size for screening adherence based on intervention conditions versus control or usual care. Due to I 2 of 89% indicating high heterogeneity, a random effects model was considered the more conservative and appropriate model for pooling effect sizes. Egger's test was used to determine whether there is publication bias.
Results
Figure 1 displays the flow diagram of study selection. A total of 1,970 titles and abstracts were found via database searching, and 45 duplicates were removed. The remaining 1,925 titles/abstracts were screened by 2 authors who were blind to each other's screening results. Once the blind was removed, disagreements were resolved via discussion. A total of 59 full-text articles were reviewed, and 36 were excluded for not meeting the criteria. Reasons for exclusion include wrong population, wrong outcomes, and wrong study design. The final sample was 23 articles.
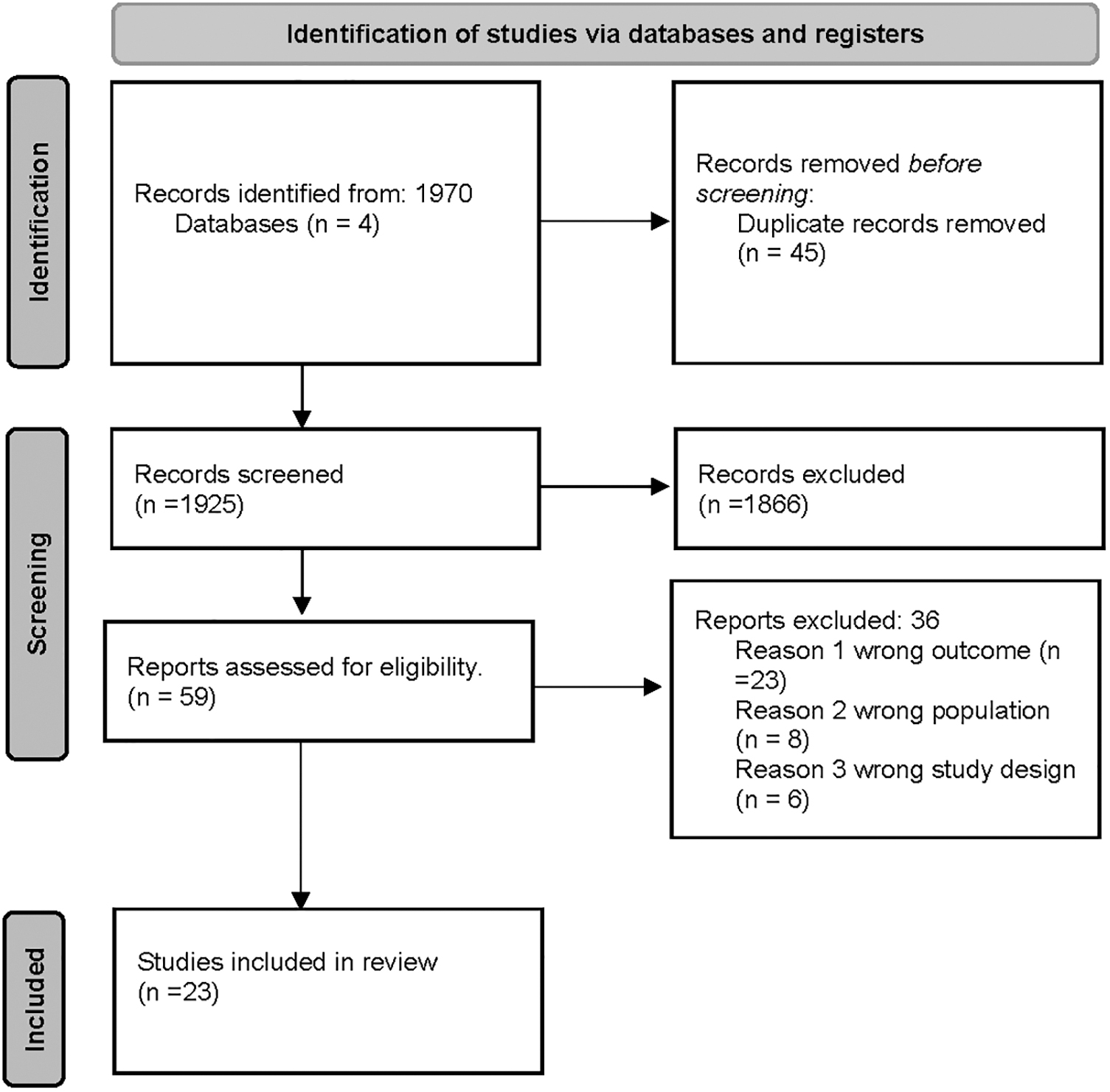
PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
Table 1 summarizes the study characteristics of the 23 included studies. The 12,786 total participants ranged in age from 20 to 70, and the majority had at least a high school education. Eight studies 23 –28 listed the majority of their participants as low income.
Summary of Studies Included in the Review
AA, African American; CHW, community health worker; CI, confidence interval; CT, culturally tailored; HPV, human papillomavirus; LHW, lay health worker; OR, odds ratio; QATSDD, Quality Assessment Tool for Reviewing Studies with Diverse Designs; RN, registered nurse.
Intervention characteristics
There were a wide range of intervention settings: community clinics, 29 –36 regional hospitals, 37 social service agency, 34 university, 38 –40 in collaboration with faith-based organizations, 41 and participants' homes, 28,33,42 mass media campaigns, 24,27 and mailed kits. 26,43 Interventions included health education classes 29,44 or forums, 39 health education and patient navigation services, 34 health education home visits 42,45 ; and health literacy program coupled with navigations services, 35 case management services, 30 text reminders, 31,41 and personalized forms or tailored letters. 32
Five studies incorporated self-sampling kits into their intervention. 23,25,26,36,43 In addition, three of those five included health education on self-sampling by community health workers. 23,25,36
Outcomes of interest
For the majority of the studies, the primary outcome of interest was to increase the participation in cervical cancer screening or the intention to screen. 24,28,29,31,32,34 –37,42 –44,46 Other outcomes of interest were cervical cancer screening knowledge and attitudes 24,29,38 –41 health literacy, 35 and knowledge of HPV. 25,39,40
Study designs and theoretical frameworks
Ten studies used a quasi-experimental design, 24,27,29 –31,33,34,37,44,46 nine used some form of randomization, 23,25,28,32,35,36,38,42,43 and four were non-experimental in design. 26,39 –41 The majority of studies did not explicitly report a theoretical framework, 23,29,31,34,37 –39,43,44,46 and four used community-based participatory methods. 25,30,40,47
Among those that explicitly reported using a theoretical framework, a wide variety were used: Social Determinants of Health, 30 communication models and theories, 24,27,42 social learning, 24,27,33,48 Health Belief Model, 32,36,47 and Precede-Proceed model. 33,35,42 Eight of the studies used medical record reviews 26,30,31,35 –37,44,46 to determine whether their outcomes were met, whereas the rest relied on self-report measures.
Use of cultural tailoring and community-based methods
Cultural tailoring is the practice of developing interventions that are consistent with the shared values, norms, roles, and assumptions of a group that shape a group's beliefs, attitudes, and behavior. 49 Many studies employed cultural tailoring in an effort to improve cervical cancer screening or knowledge.
Tailoring practices varied from adapting material into lay language, communicating about risk factors relevant to the priority population, highlighting community-specific needs, and ensuring representation in media use. 23,24,33 –36,39 –41,46 Of the studies that used cultural tailoring strategies, several found an increase in either screening behavior 23,33 –35,46 or knowledge. 39 –41
A popular method of cultural tailoring for the included studies was the use of images of African American women to reflect the priority population of the intervention; for most, this was a successful endeavor that improved screening from baseline. 23,24,35,36,39 Two exemplar studies were Staples et al., 39 who used a bitmoji of an African American woman, and Scarinci et al., 36 who used a designed graphic character reflecting African American women from the Mississippi Delta region.
Both saw an increase in their respective primary outcomes of knowledge, intention, and behavior. Le and Holt 41 were the only study that tailored their educational intervention to have a spiritual focus, tying in with messages that resonated to church-attending; they saw an increase in cervical cancer knowledge and intention.
Several studies used community advisory boards or community input to help tailor the health messages of their intervention or guide intervention development. 23,24,30,33,41 Carrasquillo et al., 23 for example, used the help of community health workers, clinic staff, and a community advisory board to design and tailor educational brochures in three different languages for their priority population.
Han et al. 35 used women from their priority population, HIV advocates, and clinical staff to create and tailor a picture guidebook to reinforce health literacy skills learned in an educational setting.
Effectiveness of interventions
Given next are general summaries and highlights from the included studies, additional information regarding intervention effectiveness can be found in Table 1.
Health education classes or forums
Several studies found that cervical cancer screening and prevention knowledge increased after participation in their health education intervention. 23,29,38 –41 Of the four studies, Staples et al. 39 and their educational forums at several Historically Black Colleges and Universities reported the highest number of items correct regarding cervical cancer knowledge. They saw a rise in knowledge scores from 74 ± 24.9 to 91 ± 21.8 (p = 0.0055).
Appointment reminders and mobile health
Of the studies that incorporated text messages and mobile health in their intervention, 31,41 only one saw a significant increase after intervention participation. Le and Holt 41 found that cervical cancer knowledge increased after participants used CervixCheck with a mean difference in score of 0.619 [t(41) = −3.64, p = 0.001]. They also reported that participants were highly satisfied with the intervention. Personalized form letters as reminders were effective in increasing Pap smear screening and mammography use, and were reported to be more effective than the personalized letters with individual medical data included as 53.3% of the women in the personalized form group were screened versus 39.7% in the personalized letters. 32
Self-sampling kits
Five studies used self-sampling as their primary strategy for increasing Pap smear screening participation. 23,25,26,36,43 Of the five, Scarinci et al. 36 saw the largest increase in uptake with their intervention of self-sampling kits, tailored educational material featuring a graphic design character of an African American women from the Mississippi region. According to the authors, there was an increase in screening participation in their intervention group of 63 out of 102, especially in comparison to their control group, which saw only 16 out of 154 women participate.
Screening uptake
Only seven studies had a control group or more than one group to compare intervention strategies and their effectiveness. Several studies used a one-group design, and thus would not be appropriate for a meta-analysis. However, three of the studies reported at least a 75% or higher screening uptake rate. 33,34,38 The studies that reported an 80% or higher screening uptake rate 33,34 used health education coupled with patient navigation services or activities that addressed practical barriers to screening.
Murphy et al. 38 used a multimedia intervention with culturally influenced narratives to increase screening uptake, reporting both short- and long-term (6-months post) differences in screening behavior and attitudes.
Four studies reported high screening uptakes at baseline which made it difficult to assess the effectiveness of their intervention strategies. 27,28,33,42 In these studies, at least 70% of their participants self-reported being up to date in their screening habits at baseline. Another study reported that Pap smear screening did not improve over time after the intervention. 27 While Whitman et al. 44 observed improvement in the proportion of women engaging Pap smear screening after participating in their intervention, the proportion was less than 30%.
Meta-analysis
Seven studies had enough information to be used in a meta-analysis that compared intervention versus control or usual care groups (Fig. 2). Overall, participants receiving interventions were almost three times as likely to report participating in cervical cancer screening (OR: 2.43, 95% confidence interval [CI]: 1.47–4.02).

Forest plot of seven included studies evaluating cervical cancer screening interventions. *Criteria for inclusion: randomized control trial, evaluation of an intervention to increase cervical cancer screening. **Interventions included are described in greater detail in Table 1.
Scarinci et al. 36 had the largest OR, observing that women who were randomized into the “Choice” towns (given a choice between participating in self-sampling or standardized screening care) and who received health education and community worker navigation were six times as likely to been screened than women living in a town with only the standard of care offered (OR: 5.94, 95% CI: 3.25–10.87).
Jibaja-Weiss et al. 32 had the smallest OR, with those receiving the intervention being only slightly more likely to participate in screening (OR: 1.06, 95% CI: 0.85–1.31). Egger's test for a regression intercept was non-significant (p = 0.663), indicating no evidence of publication.
Health equity assessment
CONSORT-Equity 2017 scores are presented in Table 2 along with how each study measured against the criteria. Studies were conducted in major cities in the North, South and West regions of the United States. 31 Four included rural residents. 24,26,36,42 The majority of the studies clearly stated health equity objectives; included a rationale for focusing on health equity; discussed context and relationship to health inequity; and discussed methods of recruitment and focus on populations experiencing inequities.
CONSORT-2017 Health Equity Extension
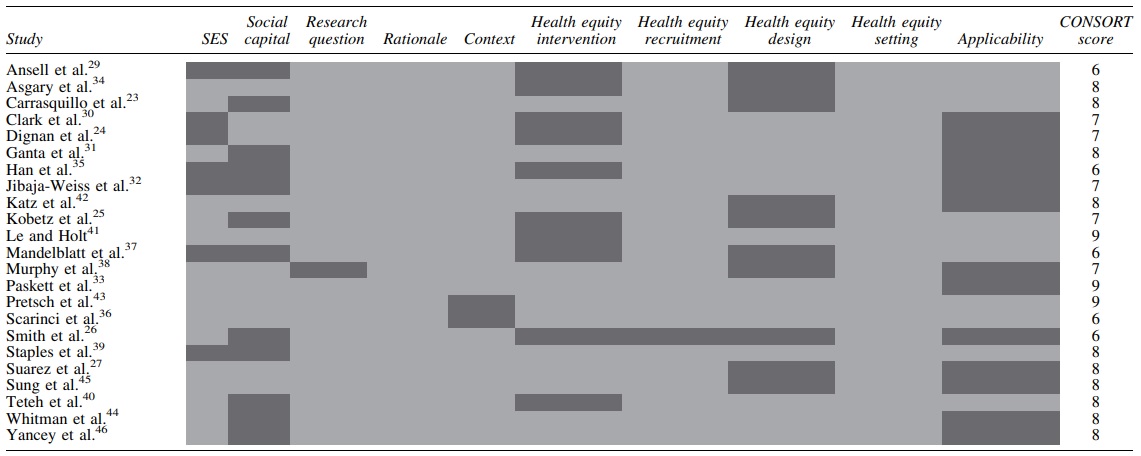
Colors in the table are defined as follows: Dark grey = no, light grey = yes.
Approximately half of the included studies struggled with the design of their intervention and study to address health equity concerns according to CONSORT-Equity 2017. For those who struggled, they did not discuss how their intervention differed from usual care or what aspects of their study and intervention were designed to answer equity questions.
Results of the health equity assessment informed by the Healing ARC Framework and PHCR praxis are presented in Table 3. None of the studies addressed all of the criteria, however three studies did meet three out of five criteria. 30,32,40 Only five studies acknowledged the impact of racism on health and use of preventative services. 30,36,38 –40 The majority of the studies attempted to redress the impact of cervical cancer disparities by improving or attempting to increase access to care.
Adapted Healing ARC Framework and Ford's Public Health Critical Race Praxis Health Equity Assessment

Colors in the table are defined as follows: Dark grey = no, light grey = yes, white = partially addressed.
None of the studies acknowledged or discussed the temporal nature of racialization and how that impacted their study. Thirteen studies acknowledged the impact of race and the importance of knowledge co-construction through the use of either community advisory boards or cultural tailoring. 23,24,32,34 –36,39 –42,46,50,51 Finally, only five studies included a call to action or discussed how the results of their work would impact their future action and planning. 25,30,32,40,44
Quality of assessment
QATSDD summary scores ranged from 7 to 35 and are presented in Table 1. Of the included studies, nine studies were considered to be of high quality based on their consistency in scoring across the QATSDD. Seven of the studies were considered lower quality due to scoring low on all 17-items.
Discussion
Cervical cancer disparities have existed for decades, and while improvements have been made, they have yet to eliminate or largely reduce disparities, particularly for African American women. Williams notes that although interventions may promote health behavior change, unless there is a concentrated effort to address the fundamental causes of racism and discrimination, then the impact will not result in lasting changes. 52
The aim of our review was to examine the effectiveness of cervical cancer screening and prevention interventions for African American women and to assess this literature's attention to health equity principles. Overall, we found that the majority of studies reported an increase in screening uptake and cervical cancer knowledge; however, some of the older articles did not find an increase. The few studies that were randomized or had a control group showed a strong increase in screening and knowledge. Notably, studies that engaged participants in intervention development observed the largest increases in either knowledge or screening adherence.
In 2018, the United States Preventive Services Task Force recommended including high-risk HPV testing as one of three cervical cancer screening strategies. 53 The inclusion of HPV testing has allowed the use of self-sampling, which is currently used as a primary screening strategy in over 40 countries. 54 Five of the studies in this review used self-sampling as their primary intervention strategy.
Self-sampling is an intervention that is gaining traction, as it is considered a convenient and easy alternative to traditional Pap smear screening. 55 For African American women who experience barriers to screening including mistrust of the health care system, 56 lack of awareness and knowledge about cervical cancer screening, 8 and financial cost and time, 57,58 self-sampling paired with health education is a potential avenue to mitigate those barriers.
It is important to mention that self-sampling is not FDA approved at this time and would require that many patients present for either colposcopy or triage cytology testing. Further research into self-sampling is necessary to ensure adequate care and timely follow-up for abnormal screening results.
Health education was a common primary or secondary aim for the majority of studies included in this review. Most of the studies found an increase cervical cancer knowledge, and notably, those that used cultural tailoring observed the largest increases. Cultural tailoring has been used to address health concerns and disparities in the African American population for almost 20 years 59 –61 and has been found to increase knowledge and promote health behavior change. 62 Tailoring methods varied, in both the media used (physical, verbal or multi) and in the level of tailoring involved (surface or deep).
Surface-level cultural tailoring focuses on matching intervention material with observable traits of the priority population through the use of language, places, and people familiar to the group. 63 Deep cultural tailoring goes beyond the surface-level approaches to tailoring messages to the values, beliefs, and norms that a group shares rather than merely observable traits. 64,65 One study's cultural tailoring did not address African American women specifically, but even so, a Mexican American women's narrative still resonated with African American participants and resulted in increased knowledge. 38
The largest increase in knowledge was found in a study that used an African American woman bitmoji and tailored facts about cervical cancer and HPV toward their participant population. 39 This reflects other findings that deep cultural tailoring health interventions to the culture and norms of the priority group are effective in encouraging health behavior change. 61
We found mixed results regarding the extent to which studies addressed health equity. Notably, a few of the included studies either did not include or minimally addressed health equity principles. 29,37 These studies tended to be older and had small outcome effects on their priority population. Half of the included studies incorporated cultural tailoring or community-based methods to address barriers to cervical cancer screening and health inequities.
There were missed opportunities with the other remaining studies that did not attempt to tailor their interventions to the culture and needs of the targeted population or include the perspective of African American women in their intervention development. Our findings highlight the need to incorporate thoughtful and detailed cultural influences that go beyond targeting a specific population without acknowledging culture, history, and the impact of racism.
The CONSORT-Equity 2017 extension, along with our additional criteria for assessing health equity principles in this body of literature, yielded important insights into areas of improvement to better address health inequities. None of the studies discussed the impact of societal racialization during the study's time period and how that may have impacted intervention development, implementation, and results.
According to Ford and Airhihenbuwa, 22 societal racialization is important in the health context because it describes how society uses race to establish social order. Thus, cervical cancer disparities are attributed to structural racism, not race, inhibiting access to care. A few studies acknowledged the impact of racism on health and use of preventative services. Even less used the word “racism.”
A small number of studies ended their discussions with a call to action or plan with how they would use their findings to carry the work forward. As is becoming increasingly important, community dissemination and implementation of intervention research not only democratizes knowledge but also aids in the empowerment of impacted communities. This is an area for improvement for many studies, not just the ones included in this review, as researchers work toward sustainable partnerships with communities.
Implications
Two major implications for future research and practice are self-sampling and deep cultural tailoring. Additional research is needed on the feasibility and sustainability of using self-sampling interventions for African American women, particularly among those who have expressed practical barriers to screening or reluctance to directly engage the health care system. Self-sampling is easy and convenient. When paired with health education initiatives, it can potentially promote health behaviors, intention, and attitudes.
Future research and practice should incorporate deep cultural tailoring and community-based approaches when targeting African American women. Tailoring allows participants to have a deeper connection with the material and intervention as they relate it to their lived experiences and the experiences of their community members.
One way that future research and practice can work toward tailoring or personalizing screening and prevention is to embrace relevant aspects of community-based participatory research methods to their studies and practice. After all, community members know how to best reach other members of their community. Using a community advisory board or pilot testing and refining with input are a few of the ways to incorporate African American women into research and practice.
Conclusions
We surveyed the current landscape of cervical cancer screening and prevention interventions targeting African American women, examining their effectiveness and commitment to health equity. We found that cervical cancer screening and prevention interventions that use self-sampling, a combination of health education and either navigation or lay health workers, or deep cultural tailoring are most effective in increasing cervical cancer knowledge and promoting screening adherence. Future research and practice should consider incorporating these.
Footnotes
Acknowledgments
The authors like to thank Kate Saylor, a senior associate research librarian, for her help and research skills with this review.
Authors' Contributions
A.W.: Conceptualization, Methodology, Writing—original and editing, Formal analysis, and Investigation; L.S.: Conceptualization, Methodology, Investigation, and Writing—editing; J.R.: Writing—editing; G.A.: Writing—Editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by NIH/NCI grant #T32-CA236621: Interdisciplinary Research Training Center in Cancer Care Delivery.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.