
Abstract
Objectives:
This study used 2000–2020 Pregnancy Risk Assessment Monitoring System data to estimate trends in smoking before, during, and after pregnancy, as well as quitting smoking during pregnancy.
Materials and Methods:
Weighted prevalence and 95% confidence intervals (CIs) were calculated by year for each smoking-related measure. Annual percent change (APC) and average annual percent change (AAPC) in prevalence were estimated using Joinpoint regression to characterize trends over time.
Results:
Between 2000 and 2020, significant decreases in the prevalence of smoking before (23.0% to 14.0%; AAPC = −2.3% [95% CI = −2.9% to −1.7%]), during (13.2% to 6.5%; AAPC = −3.4% [95% CI = −4.0% to −2.7%]), and after pregnancy (18.9% to 8.8%; AAPC = −3.6% [95% CI = −4.3% to −2.9%]) were observed. For each measure, the fastest declines occurred largely throughout the 2010s (before: APC = −5.5% [2012–2020]; during: APC = −5.1% [2009–2020]; and after: APC = −6.4% [2012–2020]). The proportion of people who quit smoking during pregnancy significantly increased from 43.2% in 2000 to 53.7% in 2020 (AAPC = 1.0%; 95% CI = 0.2%–1.9%); however, Joinpoint regression detected relatively no change in quitting during pregnancy between 2010 and 2020 (APC = 0.0%; 95% CI = −0.4% to 0.5%).
Conclusions:
The prevalence of smoking before, during, and after pregnancy has reduced dramatically in the United States between 2000 and 2020, with the fastest declines occurring throughout the second decade of the twenty-first century. However, prevention and cessation efforts are still needed since approximately half of people who smoked before pregnancy continue to smoke during pregnancy.
Introduction
The negative consequences of smoking during pregnancy have been evaluated for decades. 1 –3 Studies have found cigarette use during pregnancy to be associated with several adverse reproductive and birth outcomes, including miscarriage, 4 low birthweight, 5,6 and orofacial clefts. 7 Prenatal cigarette smoking has also been found to be associated with sudden unexpected infant death 8 and poor neurologic and lung development among exposed infants. 9,10 Regardless of these continued research efforts, prenatal cigarette smoking continues to be a leading preventable cause of infant mortality and morbidity in the United States. 11,12
The Pregnancy Risk Assessment Monitoring System (PRAMS) is a surveillance system used to monitor perinatal smoking patterns in the United States. PRAMS has previously been used to estimate trends in smoking before, during, and after pregnancy between 2000 and 2005, 13 as well as 2000 and 2010. 14 However, while the analysis of 2000–2010 PRAMS data did estimate aggregated and site-specific trends in these perinatal cigarette use behaviors, trends for different demographic subgroups (e.g., age groups, racial and ethnic groups, etc.) were not estimated across this time period. 14
Moreover, trends in these smoking behaviors have not been quantitatively described using more recent PRAMS data. Thus, the objective of this study was to estimate trends in smoking before, during, and after pregnancy overall and by selected characteristics using PRAMS data from 2000 to 2020. These data were also used to describe the trend in quitting smoking during pregnancy across the same time period.
Materials and Methods
Study design and study population
PRAMS data collected between 2000 and 2020 (Phases 4–8) were used in this study. The design and methodology of PRAMS have been described in detail previously. 15 In brief, PRAMS is an ongoing multi-site, population-based, cross-sectional surveillance system used to monitor behaviors and experiences during and around the time of pregnancy. PRAMS is a joint effort between the US Centers for Disease Control and Prevention (CDC) and several state, territorial, and local health departments. The CDC and each participating site's institutional review board approved the PRAMS protocol.
Since a site's birth certificate records serve as the sampling frame, residents who delivered a live birth during the surveillance year are eligible to be sampled into PRAMS. Individuals are selected ∼2–6 months after delivery and complete the PRAMS questionnaire by mail or phone. Data are weighted to account for survey design, nonresponse, and noncoverage. Data from participating sites are only released for analytic purposes if a site meets the minimum response rate threshold for a given year. The minimum response rate thresholds for the years included in this study are 70% from 2000 to 2006; 65% from 2007 to 2011; 60% from 2012 to 2014; 55% from 2015 to 2017; and 50% from 2018 to 2020. Supplementary Table S1 contains a list of PRAMS sites that met the annual response rate thresholds for the years, and therefore are included in this study.
Measures
Cigarette use questions from PRAMS were used to characterize this study's four main measures: (1) smoking during the 3 months before pregnancy; (2) smoking during the last 3 months of pregnancy; (3) smoking after delivery (i.e., at the time of the PRAMS interview); and (4) quitting smoking during pregnancy (among people who smoked before pregnancy).
The three questions used to estimate these measures were as follows: (1) “In the 3 months before you got pregnant, how many cigarettes did you smoke on an average day?”; (2) “In the last 3 months of your pregnancy, how many cigarettes did you smoke on an average day?”; and (3) “How many cigarettes do you smoke on an average day now?” Similar to previous PRAMS studies, 13,14 if a person reported any cigarette use during a question's specified time period, they were categorized as a cigarette smoker for that time period. A person was considered to have quit cigarette smoking during pregnancy if they indicated any cigarette use in the 3 months before pregnancy, but reported no cigarette use during the last 3 months of pregnancy.
In addition to the cigarette smoking measures, information on select demographic characteristics most commonly evaluated among pregnant people were included. The demographic characteristics incorporated in this study were as follows: pregnant parent's age (<20, 20–24, 25–34, and ≥35 years), race/ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic, and other), and educational level (<high school, high school, and >high school). Time of first prenatal care visit (first trimester, after first trimester, and none) was also included as a prenatal health care indicator.
Statistical analyses
Annual weighted prevalence and 95% confidence intervals (CIs) were calculated for all four smoking-related measures. The annual weighted prevalence and 95% CIs for smoking before, during, and after pregnancy were also estimated by the selected demographic characteristics. All weighted prevalence and 95% CI estimations were completed using SAS-callable-SUDAAN (SAS version 9.4; SUDAAN version 11.0.4) to account for PRAMs' complex survey design.
Joinpoint (version 4.9.1.0) regression analysis was used to estimate unadjusted trends over time. Joinpoint regression models linear segments on the logarithmic scale and connects the segments at “joinpoints” if a change in trend is detected. In this study, a maximum of three joinpoints (i.e., four segments) were allowed, the maximum number suggested by the software for studies incorporating 17–21 data points. To describe trends for the individual segments, annual percent change (APC) in prevalence and 95% CIs were calculated for each of the smoking measures.
Average annual percent change (AAPC) in prevalence and 95% CIs were also calculated to summarize the trend over the entire time interval (i.e., 2000–2020). The best fitting model was selected using the permutation test approach with an alpha level of 0.05. APCs and AAPCs were determined to be significantly different from zero (i.e., no trend) using an alpha of 0.05. All analyses were conducted between July and October of 2022.
Results
Smoking before pregnancy
Weighted prevalence estimates for smoking before pregnancy are presented by year in Table 1 and also illustrated in Figure 1. The prevalence of smoking before pregnancy decreased significantly from 23.0% in 2000 to 14.0% in 2020 (AAPC = −2.3%; 95% CI = −2.9% to −1.7%). However, when evaluating the individual segments, relatively no change in prevalence was observed between 2000 and 2012 (APC = −0.1%; 95% CI = −0.8% to 0.5%), followed by a significant decrease between 2012 and 2020 (APC = −5.5%; 95% CI = −6.8% to −4.2%) (Table 1).
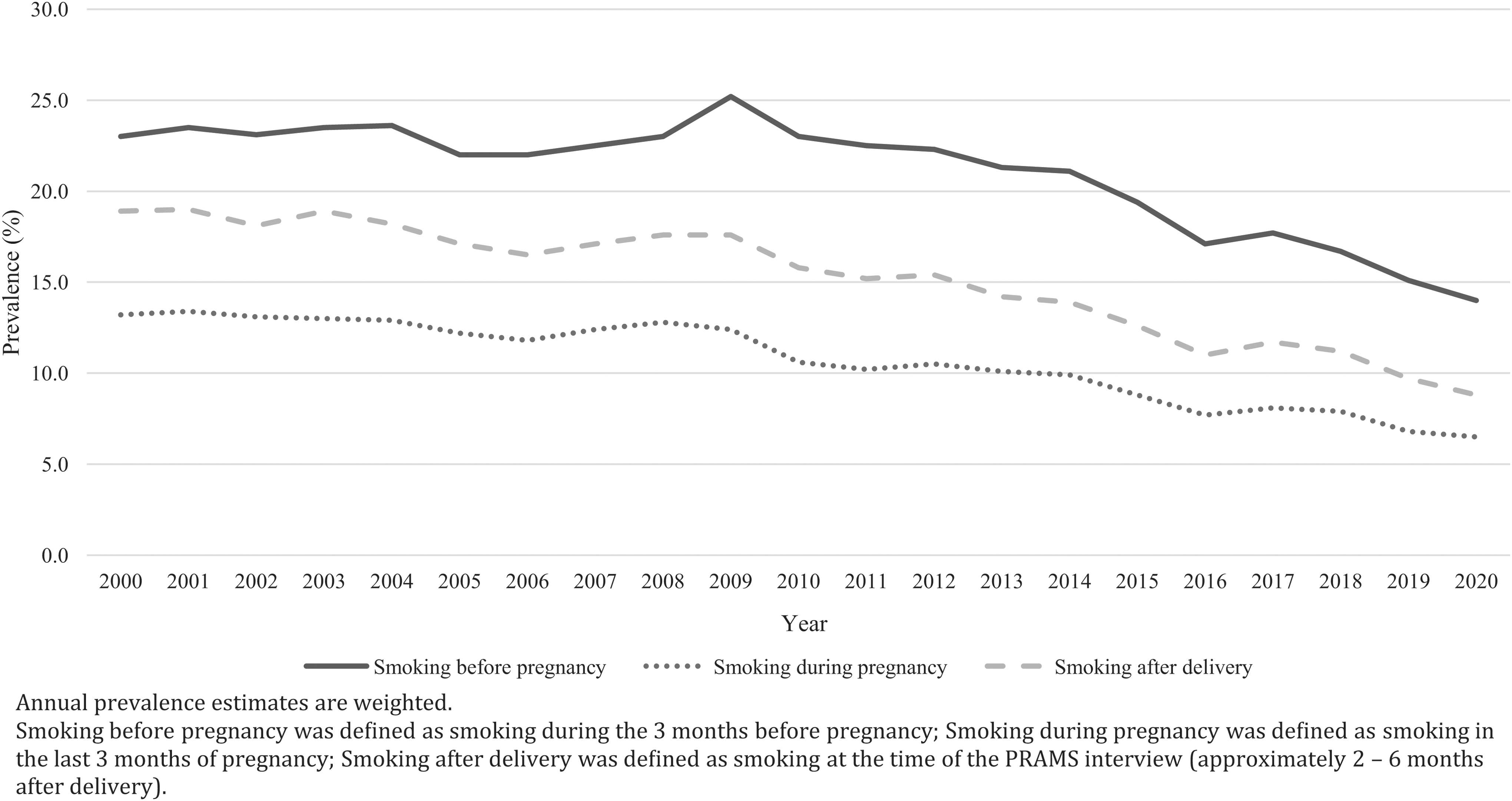
Prevalence of smoking before, during, and after pregnancy, Pregnancy Risk Assessment Monitoring System, United States, 2000–2020.
Prevalence of Smoking Before, During, and After Pregnancy by Year, Pregnancy Risk Assessment Monitoring System, United States, 2000–2020
Annual sample sizes (n) are unweighted. Prevalence estimates (%) and associated 95% CIs are weighted.
Smoking before pregnancy was defined as smoking during the 3 months before pregnancy.
Smoking during pregnancy was defined as smoking in the last 3 months of pregnancy.
Smoking after delivery was defined as smoking at the time of the PRAMS interview (∼2–6 months after delivery).
Joinpoint regression is used to identify statistically significant trends. The permutation test approach with an overall significance level of 0.05 was used for model selection, allowing for up to three joinpoints.
Asterisk indicates that the APC or AAPC is significantly different from zero at the alpha = 0.05 level.
“—” indicates no additional trend was identified.
AAPC, average annual percent change; APC, annual percent change; CI, confidence interval; PRAMS, Pregnancy Risk Assessment Monitoring System.
Supplementary Table S2 provides the annual prevalence of smoking before pregnancy by age, race/ethnicity, education, and time of first prenatal care visit. The trends for these demographic subgroups are described in Table 2. The most rapid declines in the prevalence of smoking before pregnancy by demographic characteristic were observed among people who were younger than 20 years (AAPC = −2.8%; 95% CI = −4.4% to −1.2%), non-Hispanic White (AAPC = −2.3%; 95% CI = −2.8% to −1.8%), had greater than a high school level education (AAPC = −1.8%; 95% CI = −2.6% to −1.1%), and had prenatal care during the first trimester (AAPC = −2.4%; 95% CI = −3.0% to −1.8%) (Table 2).
Trends in Prevalence of Smoking Before Pregnancy by Selected Characteristics, Pregnancy Risk Assessment Monitoring System, United States, 2000–2020
Smoking before pregnancy was defined as smoking during the 3 months before pregnancy.
Joinpoint regression is used to identify statistically significant trends. The permutation test approach with an overall significance level of 0.05 was used for model selection, allowing for up to three joinpoints.
Race/ethnicity excludes respondents from Vermont for whom data on race/ethnicity were not publicly available. Hispanic persons could be of any race. Other category includes American Indian or Alaska Native; Asian; Native Hawaiian or other Pacific Islander; and mixed race.
Asterisk indicates that the APC or AAPC is significantly different from zero at the alpha = 0.05 level.
“—” indicates no additional trend was identified.
A significant decrease in the prevalence of smoking before pregnancy between 2000 and 2020 was detected among all demographic subgroups, except for people who identified as non-Hispanic Black (AAPC = −0.2%; 95% CI = −1.5% to 1.1%) or Hispanic (AAPC = −1.5%; 95% CI = −2.9% to 0.0%). For both racial/ethnic groups, Joinpoint regression identified an initial significant increase in prevalence followed by a period of significant decrease (Table 2). For example, among non-Hispanic Black individuals, the prevalence of smoking before pregnancy significantly increased between 2000 and 2012 (APC = 4.2%; 95% CI = 2.8%–5.7%) and then significantly decreased from 2012 to 2020 (APC = −6.6%; 95% CI = −9.1% to −4.0%).
APC estimates for individual segments of time demonstrated similar trend patterns among three other demographic subgroups: (1) people who were 25–34 years of age, (2) people with a high school level education, and (3) people with greater than a high school level education (Table 2). In 2020, the highest prevalence in smoking before pregnancy by demographic characteristic was observed among people who were 20–24 years of age (18.5%), non-Hispanic White (17.7%), had a high school education (22.1%), and no prenatal care (24.3%) (Supplementary Table S2).
Smoking during pregnancy
The prevalence of smoking during pregnancy decreased from 13.2% in 2000 to 6.5% in 2020 (AAPC = −3.4%; 95% CI = −4.0% to −2.7%) with significant APCs of −1.2% (95% CI = −2.3% to 0.0%) and −5.1% (95% CI = −6.0% to −4.2%) for 2000 to 2009 and 2009 to 2020, respectively (Table 1). The fastest decreases in the prevalence of smoking during pregnancy by demographic characteristics were observed among people who were younger than 20 years (AAPC = −4.9%; 95% CI = −7.0% to −2.7%), non-Hispanic White (AAPC = −3.3%; 95% CI = −3.8% to −2.8%), had greater than a high school level education (AAPC = −3.2%; 95% CI = −4.2% to −2.2%), and had prenatal care during the first trimester (AAPC = −3.4%; 95% CI = −4.2% to −2.7%) (Table 3).
Trends in Prevalence of Smoking During Pregnancy by Selected Characteristics, Pregnancy Risk Assessment Monitoring System, United States, 2000–2020
Smoking during pregnancy was defined as smoking in the last 3 months of pregnancy.
Joinpoint regression is used to identify statistically significant trends. The permutation test approach with an overall significance level of 0.05 was used for model selection, allowing for up to three joinpoints.
Race/ethnicity excludes respondents from Vermont for whom data on race/ethnicity were not publicly available. Hispanic persons could be of any race. Other category includes American Indian or Alaska Native; Asian; Native Hawaiian or other Pacific Islander; and mixed race.
Asterisk indicates that the APC or AAPC is significantly different from zero at the alpha = 0.05 level.
“—” indicates no additional trend was identified.
All demographic subgroups exhibited a significant decrease in the prevalence of smoking during pregnancy between 2000 and 2020 (Table 3). While a significant decrease in the prevalence of smoking during pregnancy was observed among non-Hispanic Black people over the entire period (AAPC = −1.6%; 95% CI = −3.1% to −0.2%), it is important to note that non-Hispanic Black people also had a time period of significant increase in prevalence (i.e., 2000–2009: [APC = 3.2%; 95% CI = 0.7%–5.7%]) (Table 3). In 2020, the highest prevalence in smoking during pregnancy by demographic characteristic was observed among people who were 20–24 years of age (7.8%), non-Hispanic White (8.7%), had less than a high school education (13.4%), and had no prenatal care (17.1%) (Supplementary Table S3).
Smoking after delivery
From 2000 to 2020, the prevalence of smoking after delivery significantly declined from 18.9% in 2000 to 8.8% in 2020 (AAPC = −3.6%; 95% CI = −4.3% to −2.9%) (Table 1). Joinpoint regression estimated a moderate, significant decline in the prevalence of smoking after delivery between 2000 and 2012 (APC = −1.7%; 95% CI = −2.5% to −1.0%) followed by a more rapid decrease between 2012 and 2020 (APC = −6.4%; 95% CI = −7.8% to −4.9%) (Table 1).
The swiftest declines in the prevalence of smoking after delivery by demographic characteristic were observed among people who were under the age of 20 years old (AAPC = −4.7%; 95% CI = −6.5% to −2.8%), non-Hispanic White (AAPC = −3.5%; 95% CI = −3.9% to −3.0%), had greater than a high school level education (AAPC = −3.2%; 95% CI = −3.9% to −2.4%), and had prenatal care during the first trimester (AAPC = −3.7%; 95% CI = −4.3% to −3.0%) (Table 4). All demographic subgroups experienced a statistically significant decrease in the prevalence of smoking after delivery between 2000 and 2020, except for non-Hispanic Black people (AAPC = −1.2%; 95% CI = −2.4% to 0.0%) (Table 4).
Trends in Prevalence of Smoking After Delivery by Selected Characteristics, Pregnancy Risk Assessment Monitoring System, United States, 2000–2020
Smoking after delivery was defined as smoking at the time of the PRAMS interview (∼2–6 months after delivery).
Joinpoint regression is used to identify statistically significant trends. The permutation test approach with an overall significance level of 0.05 was used for model selection, allowing for up to 3 joinpoints.
Race/ethnicity excludes respondents from Vermont for whom data on race/ethnicity were not publicly available. Hispanic persons could be of any race. Other category includes American Indian or Alaska Native; Asian; Native Hawaiian or other Pacific Islander; and mixed race.
Asterisk indicates that the APC or AAPC is significantly different from zero at the alpha = 0.05 level.
“—” indicates no additional trend was identified.
Non-Hispanic Black people were also the only demographic subgroup evaluated to have a period marked by a statistically significant increase in prevalence (i.e., 2000–2010: [APC = 3.4%; 95% CI = 1.7%–5.2%]) (Table 4). In 2020, the highest prevalence of smoking after delivery by demographic characteristic was observed among people who were 20–24 years of age (11.9%), non-Hispanic White (11.1%), had less than a high school education (15.7%), and had no prenatal care (15.3%) (Supplementary Table S4).
Quitting during pregnancy
The proportion of people who quit smoking during pregnancy increased from 43.2% in 2000 to 53.7% in 2020 (Table 5). When evaluating the entire time period, a statistically significant positive trend was observed for this measure (AAPC = 1.0%; 95% CI = 0.2%–1.9%). Joinpoint regression also detected three unique trends in the proportion of people who quit smoking during pregnancy, with a significant increase between 2007 and 2010 (APC = 6.2%; 95% CI = 0.5%–12.2%) and relatively no change in the years before (2000–2007: APC = 0.3%; 95% CI = −0.6% to 1.1%) and after (2010–2020: APC = 0.0%; 95% CI = −0.4% to 0.5%) that time period (Table 5).
Proportion of Smokers Who Quit Smoking During Pregnancy by Year, Pregnancy Risk Assessment Monitoring System, United States, 2000–2020
Annual sample sizes (n) are unweighted. Proportions (%) and associated 95% CIs are weighted. Quitting smoking during pregnancy was defined as no smoking during the last 3 months of pregnancy among people who smoked 3 months before pregnancy.
Annual sample sizes (n) represent total number of people who reported smoking cigarettes the 3 months before pregnancy.
Joinpoint regression is used to identify statistically significant trends. The permutation test approach with an overall significance level of 0.05 was used for model selection, allowing for up to three joinpoints.
Asterisk indicates that the APC or AAPC is significantly different from zero at the alpha = 0.05 level.
“—” indicates no additional trend was identified.
Discussion
This study used PRAMS data to estimate trends in the prevalence of smoking before, during, and after pregnancy and smoking cessation during pregnancy between 2000 and 2020. While a recent review article used published PRAMS statistics from 2010 and 2016–2019 to generally describe recent trends in perinatal cigarette use patterns, 16 PRAMS data have not been used to quantitatively estimate trends in these behaviors since Tong et al.'s evaluation of 2000–2010 data. 14 With the inclusion of 10 additional years of PRAMS data, this study observed dramatic reductions in the prevalence of smoking before, during, and after pregnancy between 2000 and 2020.
For each of these perinatal cigarette use measures, the fastest declines in prevalence occurred during second decade of the twenty-first century. In addition, a moderate increase in smoking cessation during pregnancy was observed when assessing the entire time period; however, trend analyses demonstrate that the proportion of people who quit during pregnancy remained relatively stable between 2010 and 2020. Finally, this study identified notable trends in cigarette use during and around the time of pregnancy among different demographic subgroups between 2000 and 2020.
The reductions in prevalence observed in this PRAMS study are generally consistent with other recent studies that have used different data sources to evaluate trends in perinatal smoking behaviors in the United States. 17 –20 For example, a study that used 2002–2016 National Survey on Drug Use and Health data reported that the prevalence of smoking during pregnancy declined significantly from 17.50% in 2002 to 10.34% in 2016. 17
Another study that used CDC's National Center for Health Statistics' natality public-use file, which represents information collected on birth certificates, found the prevalence of smoking during any trimester of pregnancy to decline from 9.2% in 2010 to 6.9% in 2017. 18 While prevalence and trend estimates are expected to vary across these different sources for a multitude of reasons (e.g., data collection, survey instrument, methodology, etc.), 21 –23 results from this study reinforce findings previously noted in the published literature and demonstrate a continued reduction in perinatal smoking in the United States.
In this study, the greatest reductions in perinatal smoking prevalence were observed during the 2010s. One factor that may have contributed to these reductions is the introduction of certain tobacco-control policies during this time period, including an Affordable Care Act policy that has required Medicaid programs to cover tobacco cessation counseling and medications for pregnant people as of October 2010. 24 Another potential contributing factor is the launch of the Tips From Former Smokers campaign in 2012, the first federally funded mass media antismoking campaign in the United States, 25 a research that has demonstrated to be positively associated with cessation among pregnant people. 26
Finally, it is possible that these swift reductions in perinatal smoking prevalence may be a result of increased use of electronic nicotine delivery systems among pregnant people and people who could become pregnant throughout the 2010s. 27 –31 Therefore, it is important to continue monitoring cigarette and other tobacco use during the perinatal period as new tobacco-control strategies emerge and the tobacco product landscape continues to evolve.
Although dramatic reductions in the prevalence of smoking before, during, and after pregnancy were observed, this study also found that the proportion of people who quit smoking during pregnancy remained relatively unchanged between 2010 and 2020. Research findings indicate that several psychosocial factors may hinder a person's ability to successfully quit smoking during pregnancy such as relationships with significant others, personal well-being, and poor understanding of associated risks. 32,33
Other factors such as barriers to cessation treatments among certain disadvantaged populations (e.g., individuals covered by Medicaid) 34,35 and gaps in health care provider cessation counseling services among pregnant people who smoke 36 may also partially explain the leveling off of quitting rates observed in this study. It is advantageous that both the US Preventive Services Task Force and American College of Obstetricians and Gynecologists recently provided updated recommendations for tobacco cessation among pregnant tobacco users, 37,38 since findings from this study demonstrate an opportunity for increased tobacco cessation efforts among this population.
For smoking before, during, and after pregnancy, the swiftest declines in prevalence by demographic subgroup were observed among people who were younger than 20 years, non-Hispanic White, had greater than a high school level education, and had prenatal care during the first trimester. When evaluating the entire time period, individuals who identify as non-Hispanic Black had the slowest declines among the race/ethnicity subgroups evaluated and only observed a statistically significant decline in the prevalence of smoking during pregnancy. Moreover, throughout approximately the first half of the evaluated period, statistically significant increases in prevalence were observed among non-Hispanic Black people for each cigarette use measure.
While statistically significant declines were observed during the 2010s, the overall trends highlight the barriers and inadequacies experienced by non-Hispanic Black pregnant people in the United States. For example, non-Hispanic Black pregnant people are more likely to receive inadequate prenatal care and have lower initiation of prenatal care during the first trimester than other racial and ethnic groups. 39,40 In qualitative studies, life stress, costs, transportation and insurance limitations, and poor perceptions of health care quality have also been reported as barriers to obtaining prenatal and reproductive care services among this population. 41,42 In addition, a recent study noted that an array of interpersonal and structural barriers may impede non-Hispanic Black women from successful cessation. 43 Thus, there is a continued need for tobacco cessation programs for pregnant people and people who could become pregnant to be accessible, targeted, and culturally relevant.
Strengths and limitations
There are limitations to this study, which should be considered. First, the smoking-related behaviors evaluated in this study are sensitive, self-reported measures that may have been impacted by recall or social desirability bias. Thus, there is a potential for underestimation of cigarette use and overestimation of quitting. In addition, the estimates reported in this study are not representative of all pregnant people since PRAMS only collects information among people who delivered a live birth and does not include all pregnant people such as those who experienced a miscarriage or stillbirth. Given the association between these adverse reproductive outcomes and perinatal cigarette use, the exclusion of these individuals from the PRAMS sample may further contribute to the underestimation of cigarette use and overestimation of quitting.
The PRAMS questionnaire also only asks about smoking during the last 3 months of pregnancy. Therefore, the reported prevalence of smoking during pregnancy does not provide a complete picture of cigarette use during the entirety of pregnancy and is potentially underestimated as a result. 23 The prevalence and trend estimates reported in this study may have also been impacted by variation in PRAMS sites over the study period. Since only five sites (i.e., Illinois, Maine, Vermont, Utah, and Washington) (Supplementary Table S1) had data for each year included in the study and the reported trend estimates were not adjusted for factors such as site, there is a potential for the estimates reported in this study to be affected by site variation throughout the study period.
Strengths of this study include the use of a large, population-based sample of US pregnant people to characterize prevalence and trends in perinatal smoking behaviors overall and by different demographic characteristics. Moreover, by using Joinpoint, this study was able to estimate an overall trend for each measure and up to four unique trends within the observation period if a change in trend was detected. Finally, since the PRAMS survey is conducted 2–6 months after delivery, this study was able to estimate the prevalence and trend in smoking after delivery, which cannot be quantified by sources such as birth certificate records.
Conclusions
The prevalence of smoking before, during, and after pregnancy significantly declined from 23.0%, 13.2%, and 18.9% in 2000 to 14.0%, 6.5%, and 8.8% in 2020, respectively. For each of these measures, reductions in prevalence were greatest during the 2010s. By demographic subgroup, the fastest overall declines in prevalence were observed among people who were younger than 20 years, non-Hispanic White, had greater than a high school level education, and had prenatal care during the first trimester. A moderate, statistically significant increase in the proportion of people who quit smoking during pregnancy was observed between 2000 and 2020; however, this measure remained relatively unchanged between 2010 and 2020. Thus, while the prevalence of perinatal smoking has dramatically decreased across the first two decades of the twenty-first century, there is a need for continued and increased prevention since approximately half of people who smoked before pregnancy continue to smoke during pregnancy.
Footnotes
Acknowledgments
The authors thank Lisa Flowers for facilitating data access. The authors also thank the PRAMS Working Group and the PRAMS respondents for their roles in providing these data.
Authors' Contributions
I.Z.: Conceptualization, methodology, formal analysis, and writing—original draft. R.D.K.: Methodology, validation, and writing—review and editing. J.N.K.: Methodology and writing—review and editing. M.D.S.: Methodology, supervision, and writing—review and editing. K.A.C.: Conceptualization, methodology, supervision, and writing—review and editing.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the US Food and Drug Administration.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.