
Abstract
Background:
To address reimbursement challenges associated with long-acting reversible contraception (LARC) in the postpartum period, state Medicaid programs have provided additional payments (“carve-outs”). Implementation has been heterogeneous, with states providing separate payments for the device only, procedure only, or both the device and procedure.
Methods:
Claims data were drawn from 210,994 deliveries in the United States between 2012 and 2018. Using generalized estimating equations, we assess the relationship between Medicaid carve-out policies and the likelihood of LARC placement at (1) 3 days postpartum, (2) 60 days postpartum, and (3) 1 year postpartum, in Medicaid and commercially insured populations.
Results:
Among Medicaid beneficiaries, the likelihood of receiving LARC was higher in states with any carve-out, compared with states without carve-outs, at 3 days (adjusted odds ratio [aOR] 1.49 [95% confidence interval: 1.33–1.67], p < 0.001), 60 days (aOR: 1.40 [95% CI: 1.35–1.46], p < 0.001), and 1 year postpartum (aOR: 1.15 [95% CI: 1.11–1.20], p < 0.001). Adjustments were made for geographic region, seasonality, and patient age. Heterogeneity was observed by carve-out type; device carve-outs were consistently associated with greater likelihood of postpartum LARC placement, compared with states with no carve-outs. Similar trends were observed among commercially insured patients.
Conclusion:
Findings support the effectiveness of Medicaid carve-outs on postpartum LARC provision, particularly for device carve-outs, which were associated with increased postpartum LARC placement at 3 days, 60 days, and 1 year postpartum. This outcome suggests that policies to address cost-related barriers associated with LARC devices may prove most useful in overcoming barriers to immediate postpartum LARC placement, with the overarching aim of promoting reproductive autonomy.
Introduction
Enhancing contraceptive access, especially in the postpartum period, is critical to reproductive autonomy, which is defined as the ability of individuals to freely make decisions and access reproductive health services without interference or coercion. 1 Meeting the high demand for long-acting reversible contraception (LARC), such as contraceptive implants or intrauterine devices, in the postpartum period by promoting access reduces the incidence of unintended pregnancy. 2 In addition, short interpregnancy intervals, which are associated with preterm birth, 3 are less likely by the use of LARC. 4 Extant literature has demonstrated an inverse relationship between unintended pregnancies and interpregnancy intervals. 5 In other words, lengthening the time between delivery and conception of a subsequent pregnancy is associated with a reduced likelihood of unintended pregnancies.
Furthermore, immediate postpartum LARC placement during delivery hospitalization has been associated with increased uptake and, 6,7 importantly, a higher likelihood that individuals are using their preferred contraceptive method. 8 Until recent years, however, the majority of postpartum LARC placements have occurred in the outpatient setting 6 weeks after delivery, 6 as labor and delivery costs have historically been reimbursed through a global obstetric fee. 9 The global obstetric fee refers to the bundled payment rate that is intended to reimburse providers for the full range of services that are involved in labor and delivery, rather than billing for each service individually. Historically, immediate postpartum LARC placements have not been reimbursed by insurance because the global obstetric fee does not account for additional services that a subset of patients receives, such as LARC placement. 10,11 Consequently, LARC placements have often been delayed until 6 week postpartum visits, despite recognition of the barriers to postpartum care. 6,12 Two-thirds of patients who intend to use LARC do not receive it in the postpartum period and must resort to less effective and nonpreferred methods. 13 Among postpartum patients interested in LARC but who were not using it, the most commonly cited reasons were (1) having to come back for a separate insertion visit and (2) missing the postpartum visit. 13
To address the well-established barriers to providing immediate postpartum LARC, South Carolina became the first state to adopt a Medicaid “carve-out” policy, meaning additional reimbursement, beyond the global obstetric fee, would be provided for LARC placements during the inpatient delivery hospitalization. 14 In this way, LARC services were “carved out,” or isolated from other labor and delivery services, and could be billed separately. This Medicaid carve-out took effect in 2012, and evidence has demonstrated that this policy has expanded the availability of postpartum LARC, 10 prompting other states to follow suit (Fig. 1). The implementation of carve-out policies has been heterogeneous across states, as some states offer reimbursement for the device only, the procedure only, or both the device and procedure. This study, therefore, aims to assess the association between Medicaid carve-out policies and the likelihood of LARC placement in the postpartum period among Medicaid beneficiaries, considering differences by carve-out policy type (carve-out for device only, carve-out for procedure only, and carve-out for both device and procedure). As a secondary aim, we evaluate spillover effects that others have reported, 10 with associations between Medicaid policies and changes in postpartum LARC utilization among commercially insured patients.
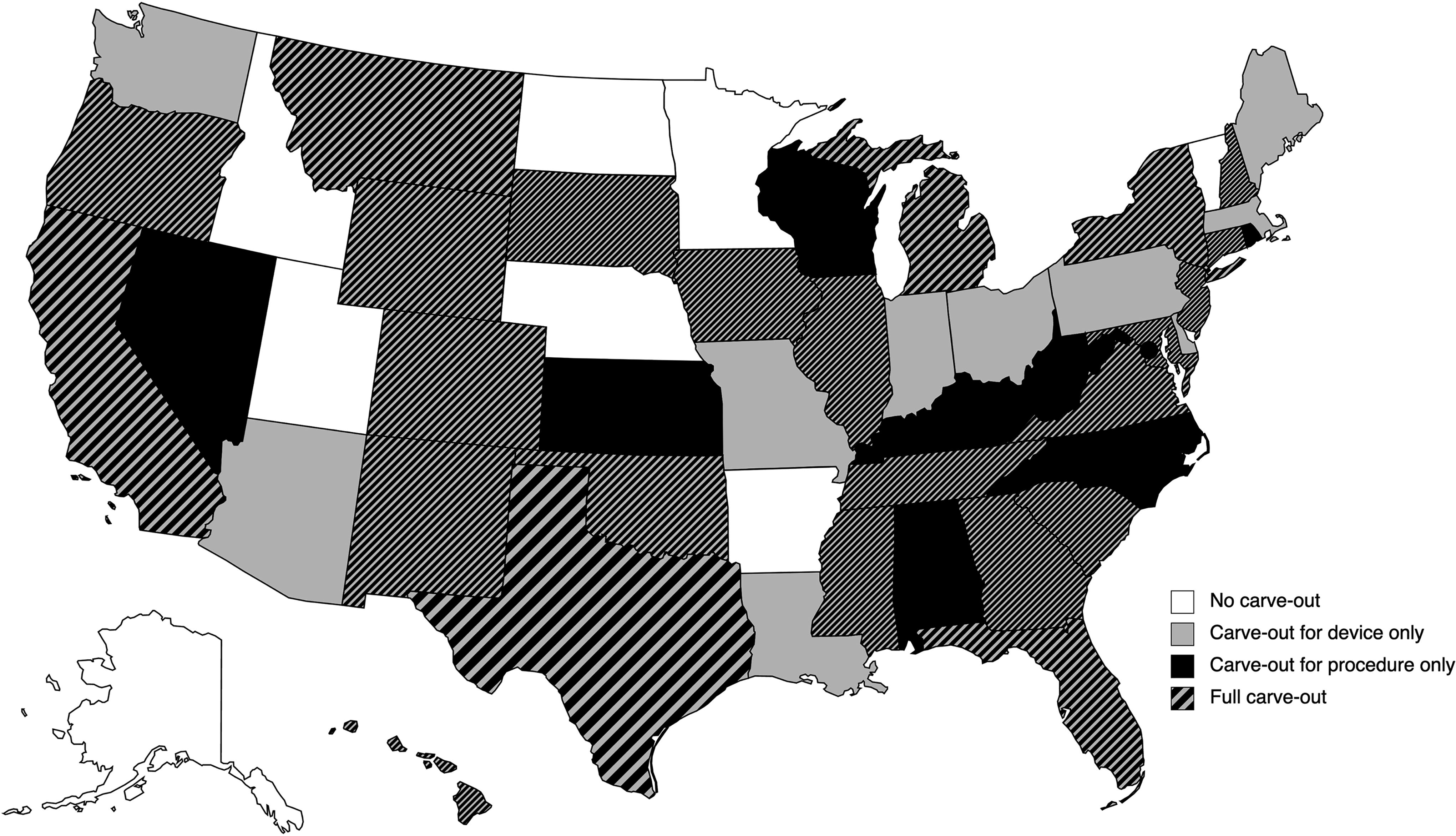
Characterizations of state Medicaid reimbursement policies for postpartum LARC in effect 2023. States were classified in one of the following four ways:
Materials and Methods
Dataset
We used detailed claims data from Symphony Health’s Integrated Dataverse (IDV®), a large medical claims database that contains hospital, medical, and pharmacy claims for U.S. patients covered by all payers, including cash, commercial, Medicaid, and Medicare. 15 These data include all available claims for birth, delivery, pregnancy, and contraceptive use from patients of reproductive age (15–44 years) between 2012 and 2018. While the data are de-identified, individual patients are assigned a unique identifier, enabling tracking across providers and payers over time and across states. 16
Claims for this study were limited to patients with a live birth delivery between 2012 and 2018. To avoid potential conflation of effects, we restricted our sample to only singleton live births identified by the International Classification of Diseases (ICD) codes. Depending on the year of the claim, either ICD-9 diagnosis code V27.0 or ICD-10 diagnosis code Z37.0 was used to identify patients with a singleton birth. We then used the following Current Procedural Terminology fourth version (CPT-4) codes to limit the identified singleton birth claims to live singleton births: 59400, 59409, 59410, 59510, 59514, 59515, 59610, 59612, 59614, 59618, 59620, and 59622. If multiple births occurred for the same patient at different times across our observation period, each birth was included separately in our data. Claims for LARC insertions were identified with CPT-4 codes for Intrauterine device (IUD) insertions (58300, J7296, J7297, J7298, J7300, J7301, J7302, S4981, Q0090, and Q9984) and contraceptive implant insertions (J7306, J7307, and S0180). The codes identified herein were obtained from the Office of Population Affairs Contraceptive Claims Code Sets. 17
The resulting dataset used in this study includes 210,994 singleton live births in an inpatient setting from 117,325 unique patients. The primary analysis was restricted to Medicaid-paid births (fee-for-service or managed care), which included 86,562 singleton live births in an inpatient setting from 49,523 unique patients. The secondary analysis was restricted to commercially paid births, which included 124,432 singleton live births from 67,802 unique patients.
Demographic data were reported to Symphony Health from a variety of sources. 15,18 Sociodemographic characteristics available for the patients included in the present study are summarized in Table 1.
Sociodemographic Characteristics of Patients
All percentages are valid percentages, meaning “unknown” or missing responses were excluded from the denominator. The degree of missing data was high for several demographic indicators: race/ethnicity (61.4 missing), education level (60.8 missing), and income (61.7 missing). No data for patient age or geographic region were missing in the analytic sample.
LARC placement
LARC insertion rates were considered at the following three key, overlapping timepoints: (1) within 3 days of delivery (0–3 days after delivery), (2) within 60 days of delivery (0–60 days after delivery), and (3) within 1 year of delivery (0–365 days after delivery). LARC placement within 3 days of delivery provides a measure of immediate placement, that is, during the inpatient delivery hospitalization. 19,20 LARC placement within 60 days of delivery provides a measure of outpatient LARC placement, which occurs between 4 and 8 weeks after delivery. 6 In addition, placement within 60 days is a performance threshold established by the Office of Population Affairs and endorsed by the National Quality Forum. 21,22 LARC placement within 1 year of delivery provides a measure of LARC placement at any point during the postpartum period, the duration of which is not well-defined, but there is budding consensus in research and clinical practice that conceptualizes it as the 1-year period after childbirth. 23 In addition, the latter two timepoints (60 days and 1 year) are relevant to U.S. policy discourse because federal law requires states to provide pregnancy-related Medicaid coverage, at minimum, through 60 days postpartum, but over the course of the COVID-19 pandemic, many states have extended coverage through 1 year postpartum. 24,25
Medicaid policy classification
Medicaid reimbursement policies were constructed as a categorical variable with the following four levels: (1) no carve-out, (2) carve-out for the device, but not the insertion procedure, (3) carve-out for the insertion procedure, but not the device, and (4) carve-out for both the device and insertion procedure. The current policy landscape is depicted in Figure 1. An additional dichotomous variable was constructed to assess differences between the two broader groups (states with carve-out policies vs. states without).
For states adopting a carve-out policy, we compiled the date of policy implementation (month and year), as shown in the Supplementary Appendix Table SA1. Dates were validated by triangulating our data with those available from Kaiser Family Foundation, 26 Mathematica, 27 State agency documents, 28 and the available literature. 9,14,29 –31 Using patient state, date of delivery, date of LARC placement (if applicable), and date of the state’s Medicaid carve-out policy implementation, all claims were coded to characterize the Medicaid policy in effect within a particular state at the time of service.
Statistical analysis
Generalized estimating equations (GEEs) were used to evaluate the relationship between postpartum LARC uptake and Medicaid carve-out policies. For the primary analysis limited to Medicaid-paid births, models were developed to evaluate the likelihood of LARC placement at the following distinct timepoints: (1) within 3 days of delivery, (2) within 60 days of delivery, and (3) within 1 year of delivery. Two models were developed at each timepoint; the first model treats Medicaid reimbursement policy as a dichotomous variable (no carve-out vs. any carve-out), whereas the latter model treats Medicaid reimbursement policy as a categorical variable (no carve-out vs. device carve-out vs. procedure carve-out vs. full carve-out) to assess differential effects by carve-out type. All models were adjusted for U.S. geographic region (Midwest, Northeast, South, and West), patient age, and seasonality to adjust for fixed-time effects, as seasonal variations have been reported for births and contraceptive use.
Claims were excluded if data from the complete follow-up period were not available. For example, claims for births in 2018 were excluded from models evaluating the likelihood of LARC placement within 1 year of delivery because 2019 data were not available in this dataset. Similarly, claims for births in November–December 2018 were excluded from models evaluating the likelihood of LARC placement within 60 days of delivery, and claims for births on December 28–31, 2018, were excluded from models evaluating the likelihood of LARC placement within 3 days of delivery.
For the secondary analysis limited to commercially paid births, GEE models were developed, considering LARC placement at the same timepoints (3 days postpartum, 60 days postpartum, and 1 year postpartum) and adjusting for the same parameters (geography, time, and patient age).
Statistical significance of model predictors was assessed with the Wald test, using a p-value threshold of 0.05. All analyses were performed with R Statistical Software, version 4.3.1 (R Foundation for Statistical Computing). This research was deemed exempt by the Institutional Review Board at Ohio State University.
Results
Postpartum LARC placement among Medicaid beneficiaries
The dataset used in this study contained claims for 86,562 births and 57,619 postpartum LARC insertions paid by Medicaid between 2012 and 2018. After excluding claims that did not have data from the complete follow-up period (see Supplementary Appendix, Table SA2), 51,254 (63.9%) LARC insertions were placed within 1 year of delivery; 26,152 (30.3%) LARC insertions were placed within 60 days of delivery; and 1,762 (2.0%) LARC insertions were placed within 3 days of delivery. The median LARC placement latency, defined as the time elapsed between delivery and LARC placement, was 64.0 days (interquartile range [IQR]: 46.0–100.0 days).
With regard to timing of placement, a significant relationship between Medicaid reimbursement policies (i.e., carve-outs) and likelihood of LARC placement was observed at 3 days postpartum and 1 year postpartum, but not 60 days postpartum. At 3 days postpartum, the likelihood of LARC placement, compared with states with no carve-out, was significantly higher in states with a carve-out (odds ratio [OR]: 1.44 [95% confidence interval (CI): 1.30–1.60], p < 0.001; adjusted odds ratio [aOR]: 1.49 [1.33–1.67], p < 0.001). Similarly, within 60 days postpartum (OR: 1.43 [1.38–1.49], p < 0.001; aOR: 1.40 [1.35–1.46], p < 0.001) and 1 year postpartum (OR: 1.19 [1.15–1.24], p < 0.001; aOR: 1.15 [1.11–1.20], p < 0.001), the likelihood of LARC placement was significantly higher in states with a carve-out policy in effect (compared with states without a carve-out). These results are summarized in Figure 2.

Relationship between Medicaid carve-out policies and the likelihood of LARC placement in the postpartum period among Medicaid beneficiaries. Compared with states with no Medicaid carve-out policies for postpartum LARC, the likelihood of receiving LARC was higher in states with any Medicaid carve-out policies at 3 days (aOR: 1.49 [95% CI: 1.33–1.67], p < 0.001), 60 days (aOR: 1.40 [1.35–1.46], p < 0.001), and 1 year postpartum (aOR: 1.15 [1.11–1.20], p < 0.001). Adjustments were made for U.S. geographic region, seasonality, and patient age. aOR, adjusted odds ratio; CI, confidence interval; LARC, long-acting reversible contraception.
Differences were observed by carve-out policy type. At 3 days postpartum, the likelihood of LARC placement, compared with states without a carve-out, was the highest among states with a device carve-out (OR: 2.07 [1.80–2.38], p < 0.001; aOR: 2.27 [1.99–2.60], p < 0.001), followed by states with a carve-out for both the device and procedure (OR: 1.27 [1.13–1.43], p < 0.001; aOR: 1.22 [1.06–1.41], p = 0.006), and the likelihood of placement was lower among states with a procedure carve-out (OR: 0.73 [0.51–1.04], p = 0.0841; aOR: 0.66 [0.46–0.95], p = 0.027). At 60 days postpartum, the likelihood of LARC placement was the highest among states with both a device and procedure carve-out (OR: 1.48 [1.42–1.55], p < 0.001; aOR: 1.42 [1.36–1.49], p < 0.001), followed by states with a device carve-out (OR: 1.38 [1.30–1.47], p < 0.001; aOR: 1.40 [1.32–1.49], p < 0.001), and states with a procedure carve-out (OR: 1.28 [1.15–1.42], p < 0.001; aOR: 1.25 [1.12–1.39], p < 0.001), compared with states without a carve-out. At 1 year postpartum, the likelihood of LARC placement was the highest among states with a carve-out for both the device and procedure (OR: 1.26 [1.21–1.32], p < 0.001; aOR: 1.20 [1.15–1.26], p < 0.001), followed by states with a device carve-out (OR: 1.08 [1.01–1.15], p = 0.026; aOR: 1.10 [1.03–1.17], p = 0.006), compared with states without a carve-out. No significant difference in the likelihood of placement was observed among states with a procedure carve-out (OR: 1.06 [0.95–1.18], p = 0.308; aOR: 1.01 [0.90–1.13], p = 0.91). These results are summarized in Figure 3, and comprehensive results are available in the Supplementary Appendix (Tables SA3–SA4).

Likelihood of LARC placement in the postpartum period by carve-out policy type among Medicaid beneficiaries. At 3 days postpartum, the likelihood of LARC placement was the highest among states with a device carve-out (aOR: 2.27 [95% CI: 1.99–2.60], p < 0.001), followed by states with a carve-out for both the device and procedure (aOR: 1.22 [1.06–1.41], p = 0.006), and lower among states with a procedure carve-out (aOR: 0.66 [0.45–0.95], p = 0.0164), compared with states without a carve-out. At 60 days postpartum, the likelihood of LARC placement was the highest among states with carve-outs for both the device and procedure (aOR: 1.42 [95% CI: 1.36–1.49], p < 0.001), followed by device carve-outs (aOR: 1.40 [95% CI: 1.32–1.49], p < 0.001) and procedure carve-outs (aOR: 1.25 [95% CI: 1.12–1.39], p < 0.001), compared with states without a carve-out. At 1 year postpartum, the likelihood of LARC placement was the highest among states with a carve-out for both the device and procedure (aOR: 1.20 [95% CI: 1.15–1.26], p < 0.001), followed by states with a device carve-out (aOR: 1.10 [95% CI: 1.03–1.17], p = 0.006), whereas no significant difference in likelihood of placement was observed among states with a procedure carve-out (aOR: 1.01 [95% CI: 0.90–1.13], p = 0.907), compared with states without a carve-out. Adjustments were made for U.S. geographic region, seasonality, and patient age. aOR, adjusted odds ratio; CI, confidence interval; LARC, long-acting reversible contraception.
Postpartum LARC placement among commercially insured patients
The dataset used in this study contained claims for 124,432 births and 78,828 postpartum LARC insertions paid by commercial insurers between 2012 and 2018. After excluding claims that did not have data from the complete follow-up period (see Supplementary Appendix, Table SA2), 57,213 (55.6%) LARC insertions were placed within 1 year of delivery, 30,785 (24.9%) LARC insertions were placed within 60 days of delivery, and 2,508 (2.0%) LARC insertions were placed within 3 days of delivery. The median LARC placement latency was 70.0 days (IQR: 49.0–112.0 days).
A significant relationship between Medicaid reimbursement policies and the likelihood of LARC placement in the postpartum period was observed among commercially insured patients, at all timepoints. At 3 days postpartum, the likelihood of LARC placement was significantly higher in states with a Medicaid carve-out (OR: 3.14 [2.84–3.47], p < 0.001; aOR: 4.85 [4.34–5.41], p < 0.001), compared with states without a carve-out. This association persisted at 60 days postpartum (OR: 2.70 [2.44–2.99], p < 0.001; aOR: 4.15 [3.70–4.65], p < 0.001) and 1 year postpartum (OR: 1.91 [1.66–2.19], p < 0.001; aOR: 2.98 [2.54–3.50], p < 0.001). These results are summarized in Figure 4.
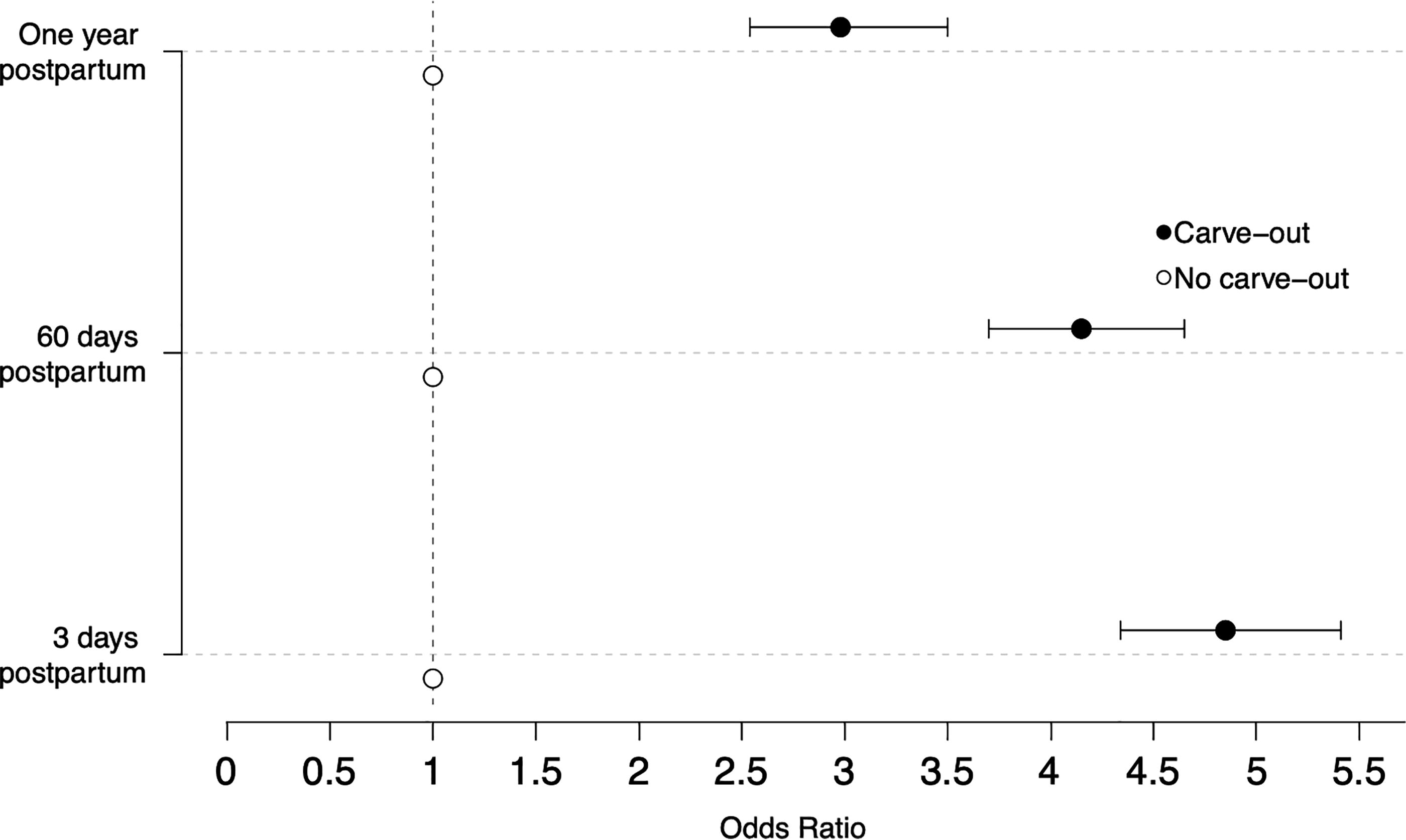
Relationship between Medicaid carve-out policies and the likelihood of LARC placement in the postpartum period among commercially insured patients. Compared with states with no Medicaid carve-out policies for postpartum LARC, the likelihood of receiving LARC was higher in states with Medicaid carve-out policies at 3 days postpartum (aOR: 4.85 [95% CI: 4.34–5.41], p < 0.001), 60 days postpartum (aOR: 4.15 [3.70–4.65], p < 0.001), and 1 year postpartum (aOR: 2.98 [2.54–3.50], p < 0.001). Adjustments were made for U.S. geographic region, seasonality, and patient age. aOR, adjusted odds ratio; CI, confidence interval; LARC, long-acting reversible contraception.
Differences were observed by Medicaid carve-out type, at all timepoints. At 3 days postpartum, the likelihood of LARC placement was the highest in states with a device carve-out (OR: 7.70 [6.93–8.55], p < 0.001; aOR: 7.08 [6.37–7.88], p < 0.001), followed by states with a carve-out for both the device and procedure (OR: 1.22 [1.07–1.38], p = 0.003; aOR: 2.02 [1.70–2.40], p < 0.001), compared with states without a carve-out. No statistically significance difference in the likelihood of placement was observed in states with a procedure carve-out (OR: 0.64 [0.40–1.02], p = 0.058; aOR: 0.69 [0.44–1.10], p = 0.12). The same trends were observed at 60 days, with heightened odds of placement in states with a device carve-out (OR: 6.95 [6.24–7.74], p < 0.001; aOR: 6.42 [5.76–7.16], p < 0.001) and states with a carve-out for both the device and procedure (OR: 0.89 [0.77–1.03], p = 0.12; aOR: 1.38 [1.15–1.66], p < 0.001), but not states with a procedure carve-out (OR: 0.63 [0.39–1.00], p = 0.051; aOR: 0.65 [0.40–1.04], p = 0.071), compared with states without a carve-out. At 1 year postpartum, the likelihood of placement, compared with states without a carve-out, was the highest in states with a device carve-out (OR: 6.00 [5.20–6.93], p < 0.001; aOR: 5.67 [4.92–6.53], p < 0.001), and reduced odds of placement were observed in states with a carve-out for both the device and procedure (OR: 0.34 [0.26–0.44], p < 0.001; aOR: 0.43 [0.31–0.59], p < 0.001) and states with a procedure carve-out (OR: 0.31 [0.11–0.82], p = 0.019; aOR: 0.32 [0.12–0.86], p = 0.024). These results are summarized in Figure 5, and comprehensive results are available in Supplementary Appendix (Tables SA5–SA6).
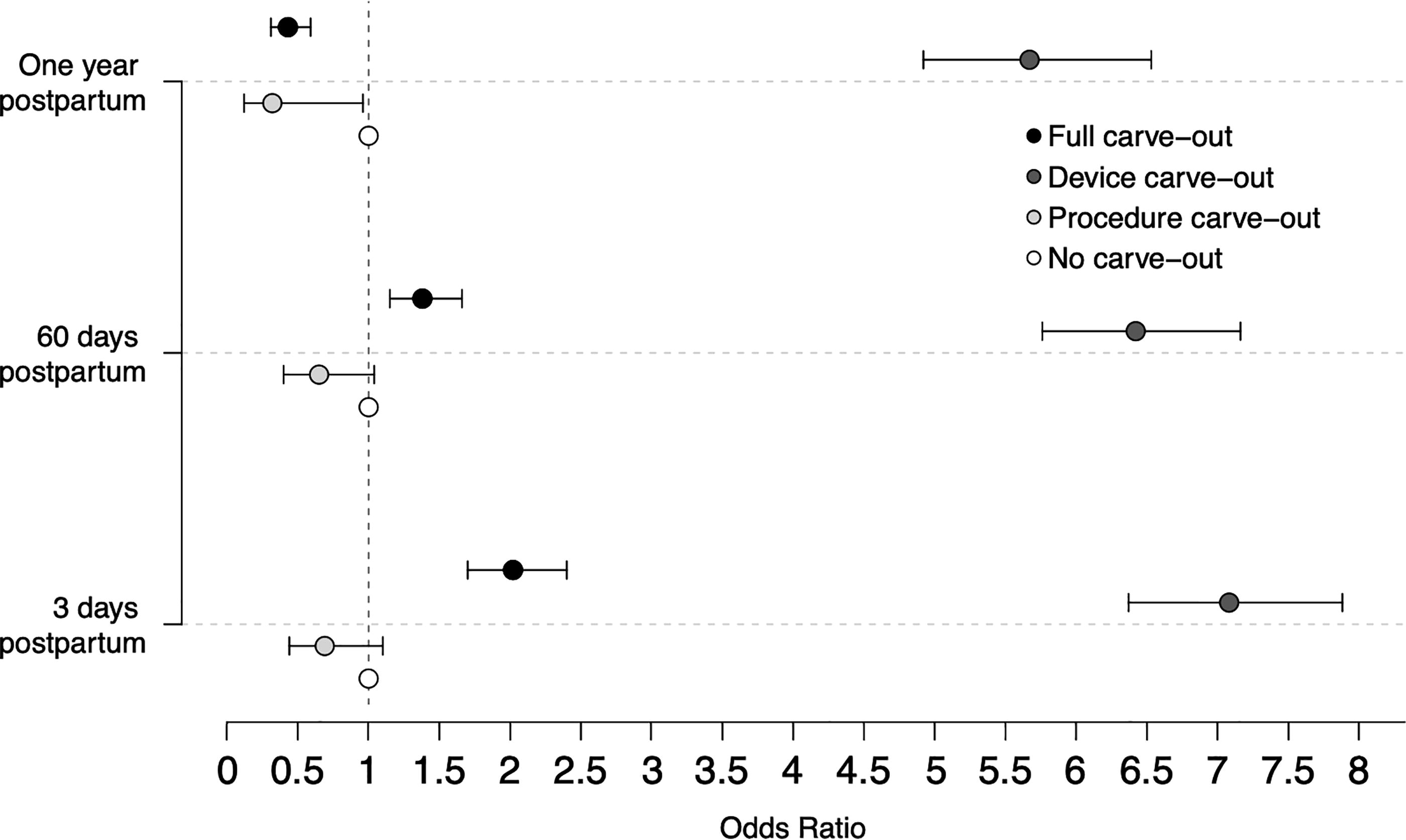
Likelihood of LARC placement in the postpartum period by carve-out policy type among commercially insured patients. At 3 days postpartum, the likelihood of LARC placement was the highest among states with a device carve-out (aOR: 7.08 [95% CI: 6.37–7.88], p < 0.001), followed by states with a carve-out for both the device and procedure (aOR: 2.02 [95% CI: 1.70–2.40], p < 0.001), whereas no significant difference in likelihood of placement was observed among states with a procedure carve-out (aOR: 0.69 [95% CI: 0.44–1.10], p = 0.122), compared with states without a carve-out. At 60 days postpartum, the likelihood of LARC placement was higher among states with a device carve-out (aOR: 6.42 [95% CI: 5.76–7.16], p < 0.001) and a carve-out for both the device and procedure (aOR: 1.38 [95% CI: 1.15–1.66], p = 0.0006), compared with states with no carve-out. No significant difference in the likelihood of placement was observed among states with a procedure carve-out (aOR: 0.65 [95% CI: 0.40–1.04], p = 0.0714). At 1 year postpartum, the likelihood of LARC placement was the highest among states with a device carve-out (aOR: 5.67 [95% CI: 4.92–6.53], p < 0.001) and, compared with states with no carve-out, lower among states with a carve-out for both the device and procedure (aOR: 0.43 [95% CI: 0.31–0.59], p < 0.001) and procedure carve-outs (aOR: 0.32 [95% CI: 0.12–0.96], p = 0.024). Adjustments were made for U.S. geographic region, seasonality, and patient age. aOR, adjusted odds ratio; CI, confidence interval; LARC, long-acting reversible contraception.
Discussion
Using claims data of Medicaid beneficiaries in the United States with a singleton live birth delivery between 2012 and 2018, we found a significant relationship between Medicaid reimbursement policies and postpartum LARC uptake at all three timepoints in the postpartum period. Heterogeneity was observed by carve-out policy type, with the strongest associations in increased postpartum LARC placement observed among states with device carve-out policies. This suggests that the high cost of LARC devices may be particularly prohibitive, 9,19,31 making device carve-out policies well-positioned to overcome barriers to postpartum LARC placement. Similarly, full carve-outs (i.e., carve-outs for both the LARC device and insertion procedure) were associated with a greater likelihood of LARC placement at 3 days and 60 days postpartum, but not 1 year postpartum. However, a consistent relationship between the likelihood of LARC placement and procedure carve-out policies was not observed.
Results from the secondary analyses restricted to commercially insured patients closely paralleled the patterns observed among Medicaid beneficiaries, providing further evidence of a spillover effect, where Medicaid policy changes impact commercially insured patients, that has been observed after carve-out policies were implemented in Georgia, New York, Rhode Island, and Maryland. 10 More specifically, Medicaid carve-out policies were associated with an increased likelihood of LARC placement at all the postpartum timepoints studied, namely, (1) within 3 days of delivery, (2) within 60 days of delivery, and (3) within 1 year of delivery. Again, device carve-out policies were consistently associated with an increased likelihood of LARC placement at all timepoints, and full carve-outs were associated with an increased likelihood of LARC placement within 3 days and 1 year postpartum. The likelihood of LARC placement in states with procedure carve-outs was comparable to states with no carve-out policies.
In both Medicaid and commercial populations, the relationship between policy and likelihood of LARC placement was strongest at 3 days postpartum. This is to be expected, as carve-out policies aim to address the challenges associated with reimbursement for LARC during inpatient delivery hospitalization by providing separate payments for LARC services, which are not sufficiently covered by the global obstetric fee for labor and delivery costs. 11,30 The majority of postpartum LARC services in this study, however, were performed outpatient, with less than half performed within 60 days of delivery. This finding is particularly relevant to contemporary discourse about pregnancy-related Medicaid coverage. Federal law requires states to provide pregnancy-related Medicaid coverage through 60 days postpartum, but over the course of the COVID-19 pandemic, many states have extended coverage through 1 year postpartum. 24,25 Extending coverage through 1 year postpartum may mitigate barriers to outpatient postpartum LARC placement, but additional policy interventions should be pursued to reduce delays in LARC placement during the postpartum period to best accommodate patients’ expressed needs and preferences for contraceptive methods and timing.
Our study is subject to a few key limitations. For one, data are drawn from a national sample, but the sample may not be nationally representative. Demographic data are rather limited, hindering our ability to assess if the relationship between Medicaid reimbursement policy and LARC outcomes was uneven across demographic groups. Challenges in assessing the representativeness and generalizability of administrative datasets are well documented, 32 and while our data provide demographic information for part of the sample, it suffers from missing observations for several demographic indicators, such as race/ethnicity (61.4% missing), income (61.7% missing), and education level (60.8% missing). In addition, patient state data come from the medical provider location associated with the patient’s most recent claim in the Symphony Health IDV database and may be subject to error if a patient moves across state lines. Further studies should assess differences between demographic groups and identify structural determinants of any disparities observed, considering both access to care and reproductive coercion. The timeframe of this study, 2012–2018, limits our ability to assess the full impact, as many states have implemented carve-out policies between 2017 and 2020. Thus, the results presented herein likely underestimate the true relationship between Medicaid carve-out policies and postpartum LARC utilization.
An additional limitation of this study is that claims did not include data on facility characteristics, such as Catholic affiliation, teaching status, obstetric level of care, and rural status. Facility characteristics may affect the availability of contraceptive services offered, 33,34 as previous research has shown that hospitals offering postpartum LARC services were disproportionately urban, teaching hospitals that are not owned by or affiliated with a Catholic organization. 10 Emerging research has shown that Catholic hospitals managed over 15% of total births in the United States in 2020, and in >10% of U.S. counties, Catholic hospitals predominate. 35 The prevalence of Catholic hospitals is particularly salient in this regard because these hospitals limit access to contraception following delivery, 33 –35 and thus, may present a barrier to LARC uptake even in states where carve-out policies have been implemented. Delivery hospital characteristics are strong correlates of access to postpartum LARC, 36 which suggests that policy implementation has been uneven and could benefit from additional interventions to close gaps between patient contraceptive preference and usage in order to effectively promote reproductive autonomy.
As one final limitation, it is important to note that states without LARC carve-out policies may be different from states with carve-out policies in critical ways, especially as it relates to access to reproductive healthcare and the strength of the reproductive healthcare system in the state. 37 –39 As such, the findings presented herein, where we highlight an association between carve-out policies and postpartum LARC utilization, could be attributable to other aforementioned ecologic factors. 37 –39
Despite its limitations, our study findings are supported by a growing evidence base of the effectiveness of Medicaid carve-outs on postpartum LARC provision. Existing literature has demonstrated that, following policy implementation, postpartum LARC services have become increasingly available, with evidence of this relationship at the level of a single health system, 40 single state, 41 –43 and multiple states. 10 We extend upon these findings, demonstrating that (1) nationally, carve-out policies were associated with postpartum LARC uptake and (2) within states with carve-out policies, there are notable differences in postpartum LARC uptake by carve-out type. This outcome suggests that device carve-out policies may be more effective than procedure carve-out policies, which is likely because of the high cost of LARC devices. 9,19,31 In other words, the cost of the LARC device may present a greater barrier to immediate placement during inpatient hospitalization than the cost of the insertion procedure. When there is a carve-out policy for the LARC device, it is likely that hospitals are more likely to have the devices on hand, reducing the barrier to patients requesting postpartum LARC. By contrast, a carve-out for the LARC procedure does not change the likelihood that there will be a trained provider to perform the insertion at the time of delivery. The providers would now receive reimbursement for the service, but the hospital may not maintain a high inventory of LARC devices, given their high cost, 9,19,31 required to perform the procedure in the first place. Procedure carve-out policies, therefore, may be attempting to address a barrier that is not the principal barrier to postpartum LARC placement.
Emerging evidence supports the effectiveness of Medicaid carve-out policies in increasing LARC access during the postpartum period, but challenges in implementation remain. In states with a carve-out for the LARC device, for example, hospitals must purchase expensive devices upfront and receive delayed reimbursement in order to have a stocked inventory for patients expressing a desire for immediate postpartum LARC placement. 31 This financial risk associated with device procurement has hindered access to postpartum LARC in New Mexico, 31 for example, and has catalyzed efforts at the University of California, San Francisco, to provide guidance to health systems on forecasting patient demand, obtaining and covering the cost of LARC, and maintaining LARC inventory. 44 Similar challenges have been cited in Georgia, where varying levels of readiness to offer postpartum LARC services were observed across hospitals, and among hospitals offering postpartum LARC placement, options were limited. 45 Some facilities only offered intrauterine devices, whereas others offered only contraceptive implants, and others offered both. 45 Significant investments have been made to overcome barriers, 44,46,47 identifying key facilitators for effective implementation, which include provider champions, 20 an enabling financial environment, hospital administrator engagement, 48 and structured learning collaboratives. 44,49,50 Enhancements in medical training, especially as it relates to shared decision-making in contraceptive counseling, 51,52 may also aid in overcoming barriers to patients’ preferred method of contraception.
Conclusions
This study provides further support for the positive association between Medicaid carve-out policies and postpartum LARC uptake, 10,40 –43 using national data to compare states with carve-out policies to states without carve-out policies. Overall, carve-out policies were associated with enhanced postpartum LARC access, but heterogeneity was observed among states with carve-out policies. States with device carve-outs were consistently associated with increased LARC uptake at (1) 3 days, (2) 60 days, and (3) 1 year postpartum, among both Medicaid and commercial populations. Significant barriers to LARC access loom large, even in states with Medicaid carve-out policies, owing to implementation challenges in hospitals and restrictions on service offerings in Catholic facilities. 10,33 –36 Additional policy interventions may aid in achieving widespread access to LARC in the postpartum period, with the ultimate aim of promoting reproductive autonomy.
Footnotes
Acknowledgment
The authors extend their thanks and appreciation to members of the Ohio Policy Evaluation Network and faculty in the Division of Health Services Management and Policy for their thoughtful feedback and comments.
Authorship Contribution Statement
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a philanthropic foundation that makes grants anonymously. The funder had no role in the analysis, writing, or decision to submit the article for publication.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.