
Abstract
Background:
Since the COVID-19 pandemic started, women have experienced more job loss owing to an increase in household and caregiving responsibilities. Gender inequities coupled with pandemic-related stressors have resulted in poor health outcomes among women. Globally, women have reported higher levels of anxiety, depression, and stress in response to the pandemic. Evidence suggests that social determinants of health have contributed to women’s poor health outcomes.
Materials and Methods:
We used the Understanding America Study to describe the social impacts women have experienced during the COVID-19 pandemic when compared with men and to explore the association between partnership status and social impacts in Los Angeles. We hypothesize that women experienced greater social impacts than men and that partnership status modified these social impacts.
Results:
In a sample of predominantly racial and ethnic minorities, we found that women experienced more social impacts related to housing insecurity compared with men. When exploring how partnership status modified these social impacts, we found that women without partners experienced more social impacts specific to financial hardships when compared with women who were in a partnership.
Conclusions:
It is likely that the COVID-19 relief efforts helped women mitigate social impacts but not housing or financial security. The overall goal is to inform policies so that better measures can be implemented to prepare for the next public health disaster or global health threat.
Introduction
The COVID-19 pandemic changed the lives of people around the globe. Measures that were put in place to prevent disease spread, including social distancing and stay-at-home orders, had unintended consequences on women’s ability to progress socially and economically. 1 Women who were overrepresented in minimum-wage industries before the pandemic were burdened by the economic shocks brought upon by the COVID-19 pandemic. 2 –4 Since the pandemic started, women have experienced higher financial instability owing to being laid off, being furloughed, and/or leaving the workforce because of an increase in household and caregiving responsibilities. 2,5,6 According to the Centers for Disease and Control Prevention, 7 two out of every three caregivers are women. Caregivers are at a higher risk of poor physical and mental health. 7 Gender inequities coupled with pandemic-related stressors have resulted in poor health outcomes among women, including those who are caregivers. 6,8,9
Stress-induced conditions such as psychological distress, anxiety, depression, and substance use have been on the rise. 10 –12 Globally, women have reported higher levels of anxiety, depression, and stress in response to the pandemic. 6,8,9 Evidence suggests that social determinants of health (SDH) have contributed to women’s poor health outcomes. 13,14 SDH are social, economic, physical, and environmental or nonmedical factors affecting health. 15 A study examining health-related socioeconomic risk factors among women during the pandemic found that women reported higher food insecurity and intimate partner and other interpersonal violence. 1 Versey and Russell 16 found that the pandemic exacerbated housing instability for African American and Latinx women. A Kaiser Foundation report on women’s health indicated that women delayed health care more than men during the pandemic. 17 It will take women decades to recover from the social impacts inflicted by the pandemic. 1
Recent literature revealed that women who are married or in a cohabiting relationship reported better mental health outcomes during the pandemic. 18 –20 Literature often focuses on how marriage and stable partnerships buffer the effects of stress. 21 Evidence shows that married women and women in stable relationships have better health outcomes and life satisfaction. 22 However, there is a lack of research showing how social impacts experienced during the pandemic have affected women, including those with different partnership status (i.e., those with a partner vs. those without a partner).
We will use the Understanding America Study (UAS) 23 to describe the social impacts women have experienced during the COVID-19 pandemic compared with men and to explore the association between partnership status and social impacts in Los Angeles. We hypothesize that women experienced greater social impacts than men and that partnership status modified these social impacts. The overall goal is to inform policies so that better measures can be implemented to prepare for the next public health disaster or global health threat.
Methods
Study sample
The project described in this article relies on data from surveys administered by the UAS, which is maintained by the Center for Economic and Social Research (CESR) at the University of Southern California (USC). Secondary analyses were performed on the USC, CESR, UAS 23 project. The publicly available UAS uses a longitudinal probability-based internet survey to capture information on an ongoing basis on American household demographics and health nationwide via laptops, PCs, tablets, or smartphones. 23 The UAS uses address-based sampling. 23 With address-based sampling, postal records are used to sample from across the nation via random sampling. 23 Participants completed a baseline survey that collected information on basic demographics and provided consent to participate in future longitudinal surveys. As part of Wave 28 of data collection between May 12, 2021, and June 22, 2021, UAS 347 targeted all Los Angeles area residents who had consented to participate in future surveys (UAS 46). This survey captured information on diet, lifestyle, employment, health, housing, and COVID-19. 23 Adult respondents over 18 years of age were included in the sample. The survey was distributed to 1,626 respondents, of whom 1,117 completed the study (response rate: 68.0%). Response rates vary according to topic, time of the year, population selected, and the amount of time the survey is in the field. 23 A total of 138 (12.3%) respondents indicated they no longer resided in the Los Angeles area and were excluded from further analysis. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of USC or UAS. We received an institutional review board exemption from the University of San Francisco.
Measures
To describe the social impacts of the COVID-19 pandemic, we examined three outcome variables related to the SDH, including financial difficulties, delayed payment of health expenses, and housing insecurity brought on by COVID-19 since the pandemic began in March 2020. The survey items followed a 5-point Likert scale to measure the frequency of each social impact (1 = never, 2 = rarely, 3 = sometimes, 4 = often, and 5 = all of the time) (Figs. 1 and 2). We categorized respondents into dichotomous groups based on self-reported responses: (1) those experiencing any social impact and (2) those experiencing a social impact frequently. We defined those experiencing any social impact as those who reported ever experiencing a social issue. Those who reported never experiencing a social issue were considered to have never experienced a social impact. Those who experienced “frequent” social impacts were defined as those reporting experiencing a social impact all of the time or often. Those who experienced the issue sometimes, rarely, or never were considered to have experienced a social issue infrequently. We examined each outcome by gender to identify whether women experienced greater social impacts during the COVID-19 pandemic compared with men. Gender was defined as those reporting being female or male. We then examined partnership status among women to evaluate whether women in a partnership experienced social impacts differently compared with women not in a partnership. Partnership status was defined as partnership if respondents reported being married or living with a partner and without partnership if respondents reported being separated, divorce, widowed, and never married.
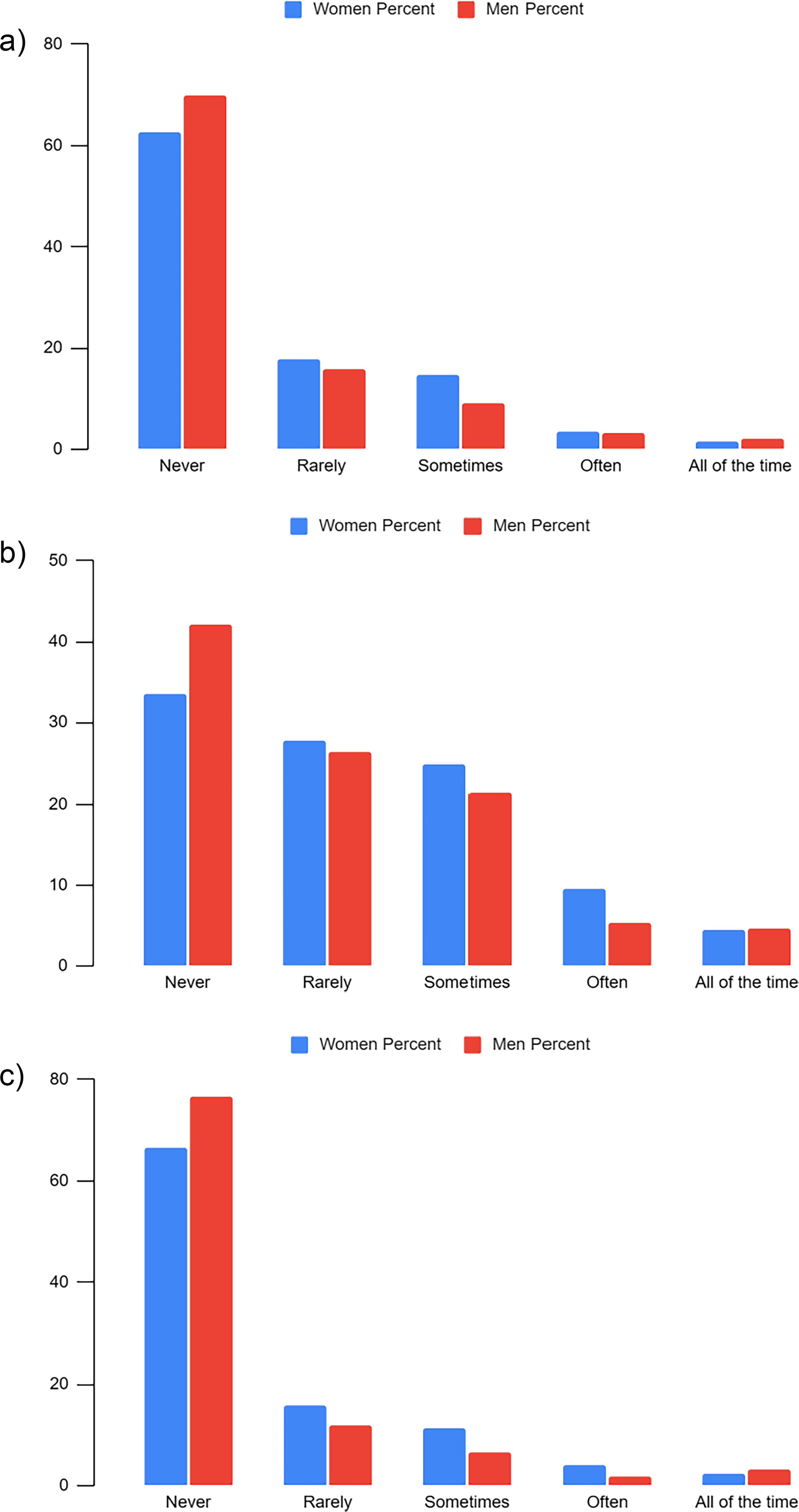
Frequency of self-reported social impacts with
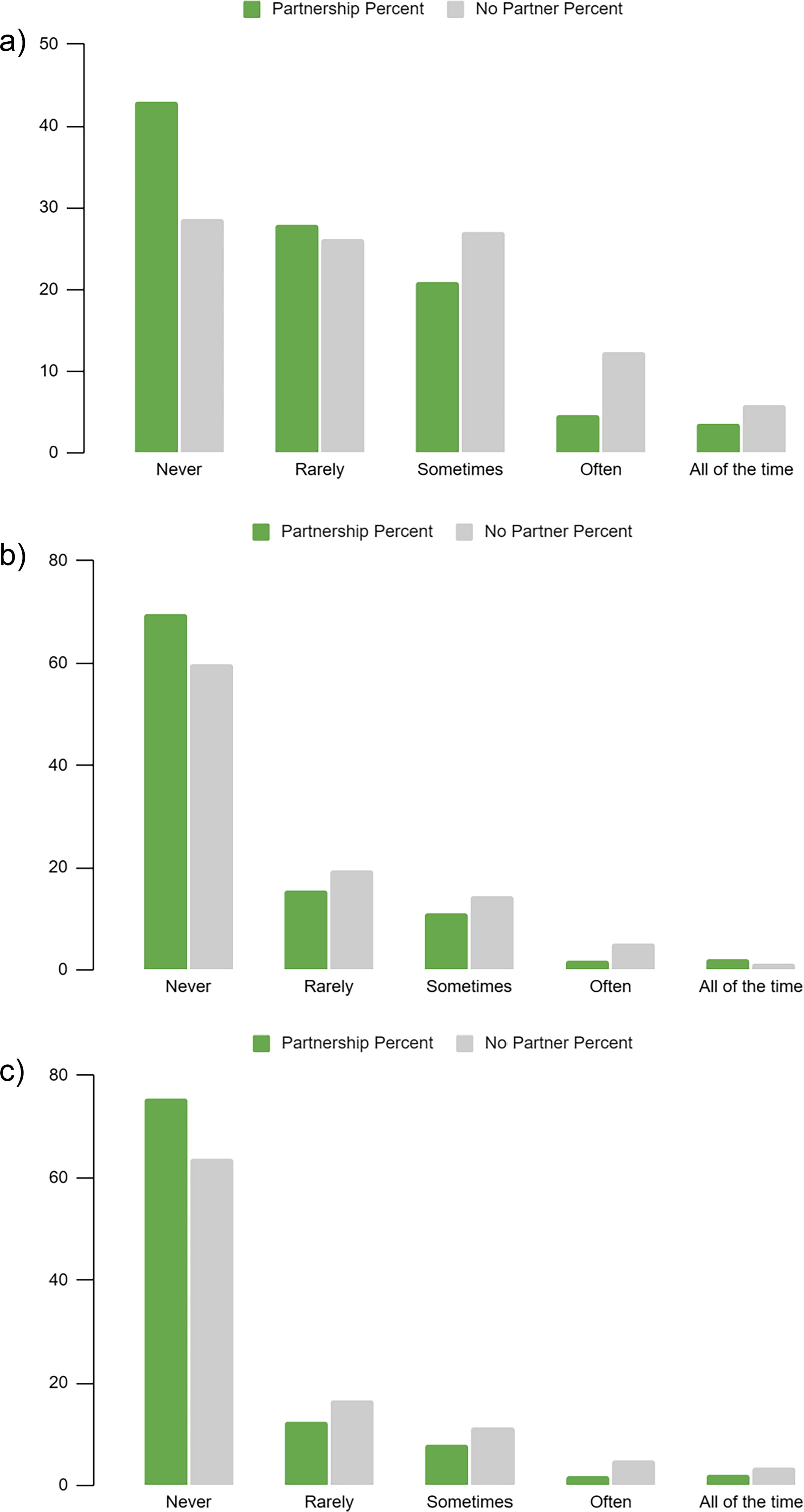
Frequency of self-reported problems with
Statistical analysis
The survey assigned poststratification weights to ensure a representative survey sample. We compared respondents’ demographic characteristics and self-reported social impacts by gender and partnership status groups using chi-square tests. Logistic regression models were used to examine the association between social impacts (outcome) by gender (exposure) and partnership status (among women only). Models were adjusted for age, race, ethnicity, and employment. All models provide adjusted odds ratios (aORs) and corresponding 95% confidence intervals (CIs). All analyses were conducted using Stata statistical software, version 17. 24
Results
Among 979 respondents residing in the Los Angeles area, 592 (60.4%) identified as women and 387 (39.5%) as men (Table 1). The sample was predominantly composed of racial and ethnic minorities. A total of 408 (68.9%) women identified as racial and ethnic minority women compared with 217 (56.1%) men. Non-Hispanic White women and men comprised 154 (26.0%) and 157 (40.6%) respondents in our sample, respectively. Non-Hispanic mixed women and men were 30 (5.1%) and 13 (3.4%) respondents in our sample, respectively. The majority of women and men were between the ages of 19–54 years old (n = 427/592, 72.2%; n = 255/387, 65.4%, respectively). More than one-third of women, (n = 230/592, 38.9%) reported a household income of less than $39,999, whereas one-half of male respondents reported a household income of more than $75,000 (n = 187/387, 48.3%).
Characteristics of Participants—Understanding America Survey, Los Angeles, California, 2021
Social impacts by gender
When exploring any social impacts brought on by the COVID-19 pandemic that women experienced compared with men, we found that the odds of experiencing any financial difficulties and delayed payment for health expenses to afford housing expenses were slightly higher for women compared with men (aOR = 1.14; 95% CI = 0.93, 1.68; and aOR = 1.17; 95% CI = 0.86, 1.59, respectively) (Table 2). The largest disparate social impact was housing insecurity, with women experiencing 42% higher odds of housing insecurity compared with men (aOR = 1.42; 95% CI = 1.03, 1.96). When considering the frequency of these social impacts, more frequent financial difficulties were reported by women compared with men (aOR = 1.22; 95% CI = 0.79, 1.89), but this difference was not significant and frequent issues for other social impacts were not more commonly reported by women compared with men (Table 2).
Unadjusted and Adjusted Odds Ratios Comparing the Odds of Experiencing Social Impacts from the COVID-19 Pandemic Among Women vs. Men—Understanding America Survey, Los Angeles, California, 2021
Models were adjusted for age, race, ethnicity, and employment.
†Significant at p < 0.05.
OR, odds ratio.
Social impacts by partnership status
When exploring any social impacts by partnership status, we found that the odds of experiencing any financial difficulties brought on by the COVID-19 pandemic that affected physical or mental health were higher for women without partnership compared with women in partnership (aOR = 1.72; 95% CI = 1.14, 2.59) (Table 3). The odds of experiencing delayed payment for health expenses to afford housing were higher for unpartnered women compared with partnered women (aOR = 1.21; 95% CI = 0.82, 1.80) (Table 3), although this difference was not statistically significant. Similar results were observed for housing insecurity. When considering the frequency of these social impacts by partnership status, we found that the odds of experiencing frequent financial difficulties were nearly three times higher for unpartnered women compared with partnered women (aOR = 2.77; 95% CI = 1.56, 4.81) (Table 3). Similarly, the odds of frequent housing insecurity was two times higher for unpartnered women compared with partnered women (aOR = 2.12; 95% CI = 0.99, 4.52). Unpartnered women had slightly greater odds of frequent experiences with delayed payment for health expenses compared with partnered women (aOR = 1.17; 95% CI = 0.52, 2.61), and this difference was not statistically significant.
Unadjusted and Adjusted Odds Ratios Comparing the Odds of Social Impacts of the COVID-19 Pandemic among Women in a Partnership vs. Women not in a Partnership—Understanding America Survey, Los Angeles, California, 2021
Models were adjusted for age, race, ethnicity, and employment.
†Significant at p < 0.05.
OR, odds ratio.
Discussion
Results from the UAS administered to a diverse sample of adults in Los Angeles, California, indicate that women experienced more social impacts from the COVID-19 pandemic, particularly women without a partner. The strongest disparities were observed for housing insecurity. It is likely that the COVID-19 relief efforts have helped women mitigate social impacts but not housing. In places such as Los Angeles, housing insecurity continues to be a social factor affecting Black, Latina, and Native American women, single mothers, and the elderly. 25 Housing insecurity is described as not being able to afford rent or mortgage payments, often leading to moving, foreclosure, eviction, overcrowding, and/or spending majority of income on housing. 26,27 Those spending 30% of income on housing are considered cost burdened, whereas spending 50% of income on housing is considered severely cost burdened. 27 Most renters have experienced higher cost burden rates than homeowners during the pandemic. 28
Housing can, directly and indirectly, affect health. 29 Overcrowding has been associated with high mortality rates, infectious diseases, chronic diseases, and other health issues. 30 –32 Because affordable housing and housing stability are fundamental determinants of health for women, COVID-19 relief efforts must be extended to prevent evictions. Literature is being published showing that housing relief efforts have assisted in reducing evictions since the pandemic started. 33 –35 Close to 5.3 million payments were issued for current and outstanding rents with some utility assistance in 2022. 36
As the national COVID-19 relief efforts came to an end in 2023, there is an expectation for measures and policies to be in place to provide long-term assistance for housing. Housing instability is slowly becoming a national problem that requires federal intervention. Federal subsidies appear to reduce housing instability. Reports show that subsidies can lower rent to affordable rates and reduce the cost burden by 15% for those using Section 8 vouchers. 36 Additional measures are needed to expand the development and preservation of housing for low-income households, including constructing affordable housing units. 36 More immediate policies are needed to protect against eviction, given that historically those evicted have been women of color, including single mothers. 37,38
Women who reported being without a partner experienced more frequent financial difficulties than partnered women. Our findings align with research showing that unpartnered adults experience more financial hardships compared with partnered adults. 39 Research shows that having a partner buffers financial stress. 40,41 However, more women are choosing to be alone. It is well documented that socioeconomic factors and other personal matters influence women’s life satisfaction and happiness, whereas men are influenced by pleasurable experiences. 42,43 Globally, women are choosing to reach independence, pursue career opportunities, and restructure who becomes part of their social support system. 44 In this cultural shift, marriage is no longer considered a necessity but a choice. The Pew Research Center published a report on earnings by gender and found that young women are making the same or more money than men in some metropolitan cities. 45 However, this is the case for some but not all women.
The gender pay gap still exists, making it hard for some women to progress socially and economically. The gender pay gap explores the discrepancies in employment, occupations, and pay between all women and men. 46 Historically, women have been paid disproportionately less than men. 47 Factors that contribute to the gender pay gap are overrepresentation in low-wage industries that offer fewer benefits, discrimination, and biases in hiring, promotion, and paying practices among women and men; educational and career choices; lack of workplace accommodations for women caring for children; and greater responsibilities in positions. 46,48,49
The COVID-19 pandemic has exacerbated the gender pay gap for racial and ethnic minority women. A U.S. Government Accountability Office report found that Hispanic women make nearly $0.58 for every dollar White men make. In comparison, Black women make about $0.63 for every dollar White men make. 50 Those reaching parity are Asian and White women. 51 Research has repeatedly shown a strong association between low socioeconomic status and poor health outcomes. 52 Researchers have started to document how socioeconomic status is a significant contributor to racial disparities in health along with other structural factors. 53
Better measures are needed to help all women reach parity with men. Some states, such as California, are implementing policies that require employees to disclose the salary ranges for positions. 54 A study exploring the effects of pay transparency among faculty earnings found that laws could lower the gender pay gap by 20% to 40% between men and women. 55 Pay transparency can reduce the gender pay gap when combined with a salary history ban. 55 –57 A study examining bans on pay history discovered that the gender gap was reduced by 4.2% among hourly pay employees and 4.5% among weekly pay employees. 57 For racial and ethnic minority women, banning salary history increased wages by 5.9%. 56
By not disclosing previous salary and having transparency in pay, women, particularly women of color, can prevent perpetual inequities in pay from persisting. Additional resources and research are needed to help women of color progress socially and economically. Although these associations may apply to other areas of the United States, including other metropolitan cities, our results do not generalize nationally.
Limitations
This study used secondary, retrospective data, thus introducing recall bias. The questions asked respondents to recall events that occurred at the beginning of the pandemic or since March 2020. It relied on self-reported responses, which are prone to social-desirability bias. 58 The study specifically focused on women in the Los Angeles area, and the sample was restricted to those with internet access and technological literacy. As a result, our findings may not generalize to the national population of women. Finally, although the study helped highlight the importance of addressing social impacts brought upon by the pandemic, social impacts have likely decreased, given the amount of resources, programs, and initiatives established to improve gender equity and equality.
Conclusion
For women to recover from current and future public health disasters or global health threats, policies are needed now to mitigate the effects. Designated relief should be provided for single women who are not married or in a partnership to improve their financial and economic well-being, particularly for women of color. Stable housing is critical to reaching optimal health and well-being. Additional resources and measures are needed to keep women sheltered. A more comprehensive approach is needed to help women all around. An intersectional approach focuses on how multiple systems of oppression affect women’s health. Women’s health does not happen in a vacuum. More research is needed on how race, ethnicity, gender, and sexuality interact with social factors to mediate health outcomes. This includes exploring how structural inequalities perpetuate the gender and racial pay gap.
Footnotes
Acknowledgments
This research was conducted in partnership with the Los Angeles County Commission for Women’s Health Committee and the Iris Cantor—UCLA Women’s Health Education & Research Center.
Authors’ Contribution
J.M.: Conceptualization, Methodology, Resources, Writing—Original Draft, Writing—Review & Editing, Project administration. B.G.: Data Curation, Formal Analysis, Visualization, Writing—Review & Editing. A.R.: Writing—Review & Editing, Supervision, Validation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.