
Abstract
Background:
The United States has high and increasing rates of maternal morbidity and mortality, large proportions of which are related to cardiovascular health (CVH).
Methods:
We searched for National Institutes of Health (NIH) supported research as well as that of two other Agencies in the U.S. Department of Health and Human Services (DHHS) for fiscal years (FY) 2016–2021. Grants included maternal health conditions or exposures across all pregnancy stages, but excluded grants that focused entirely on birth, neonatal, infant/childhood outcomes. Results were manually curated by reviewing the abstract and specific aims. Grants deemed to be relevant were grouped by category.
Results:
Between FY 2016–2021, overall Maternal Health grants remained unchanged at an average of 1.4% of total DHHS grant funding. Maternal CVH-specific (MCVH) funding amounted to $278,926,105 for 755 grants, $191,344,649 was for 534 Type-1 grants, representing a twofold increase. Non-NIH DHHS agencies most commonly funded general Maternal Health related to CVH; NIH focused funding classified as hypertensive disorders of pregnancy, maternal morbidity and mortality, obesity, and diabetes. Non-NIH DHSS Agencies most commonly funded clinical applied research. In addition to clinical applied grants, NIH funded substantial proportions of grants classified as basic research, clinical trials, and/or translational. National Heart, Lung, and Blood Institute (NHLBI) MCVH grants studied participants in the pre-partum period (78.5%), followed by the post-partum period (50.5%), with relatively few in pre-pregnancy and peri-partum periods (10.8% and 9.7%, respectively); at the NIH level, the peri-partum period had better representation at 20.3%, whereas the pre-pregnancy period remained low at 9.9%.
Conclusions:
Federal grant funding for maternal health including MCVH increased at the same rate as its funding for overall research, and represented only 1.4% of overall total funding. The pre-pregnancy period was understudied in overall NIH funding and represents a gap area whereby funding agencies could further foster research advances.
Introduction
The high and increasing rates of severe maternal morbidity and mortality in the United States are a cause of concern for women, families, communities, health care professionals, researchers, and policymakers. 1,2 A large proportion of maternal morbidity and mortality is related to cardiovascular disease (CVD) or risk factors for CVD. Cardiovascular conditions (cardiac and coronary conditions, cardiomyopathy, hypertensive disorders of pregnancy (HDP), thrombotic embolism, and cerebrovascular accidents) account for 40% of maternal deaths, with excessive hemorrhage adding another 14%. 3
Four in five maternal deaths are considered to be preventable. 3 Obesity, elevated blood pressure, elevated blood glucose, and dyslipidemia are risk factors for maternal morbidity (including HDP, gestational diabetes mellitus [GDM], and severe maternal morbidity and mortality). 4 –6 HDP (gestational hypertension, pre-eclampsia, and eclampsia) and GDM are both rising and now highly prevalent at >8% and >7% of pregnancies, and are in turn risk factors for future CVD. 7 –10
Thus, prevention or treatment of risk factors for CVD before, during, and after pregnancy may prevent both adverse maternal pregnancy outcomes and future CVD in the mothers. 10 Overlaying the biological factors are social determinants of health (SDOH), and in particular non-Hispanic Black women and American Indian/Pacific Islander women have markedly higher rates of maternal morbidity and mortality, with more recent increases in Hispanic women. 11,12
The aim of this portfolio analysis is to examine trends in Federal funding for maternal health research, and specifically to assess the proportion and direction of funding related to cardiovascular health (CVH). The analysis focuses on maternal rather than fetal health, and while we acknowledge that conditions such as small for gestational age delivery and pregnancy loss may also reflect aspects of maternal health, fetal health falls outside the scope of the current analysis. 2
Methods
The data source was the National Institutes of Health (NIH)'s Office of Portfolio Analysis' iSearch database https://itools.od.nih.gov/help/portfolios. We included NIH-supported research along with those supported by two other Agencies in the U.S. Department of Health and Human Services (DHHS): the Agency for Healthcare Research and Quality (AHRQ) and the Centers for Disease Control and Prevention (CDC) for Fiscal Years (FY) 2016–2021.
We searched for terms related to maternal health in the specific aims and abstracts of grants. We included grants that studied maternal health conditions or exposures across all stages of pregnancy. We included maternal health conditions or exposures even if they were not the primary focus of the research. The terms were obtained from the Research, Condition, and Disease Categorization (RCDC) tool https://report.nih.gov/funding/categorical-spending/rcdc which was established to track NIH funding for diseases and conditions.
We did not use the Maternal Health RCDC itself for this portfolio analysis, because it is NIH specific and is not utilized by the AHRQ and CDC. In addition, the Maternal Health RCDC was created in 2017 and would have missed awards made in 2016. The Maternal Health RCDC encompasses some 200 terms, therefore a simple search for those terms would yield many false positives. Instead, we used the i-Search “minimum should match” feature for terms in the specific aims and abstract to conduct a more controlled search.
We excluded grants that focused entirely on birth, neonatal, infant, or childhood outcomes. We included awards for Type 1 (new)—that is, support of a project that has not been previously funded, Type 2 (competing continuation)—that is, additional funding for a period subsequent to that provided by a current award, Type 3 (supplement)—that is, additional funds during a current project period to support new or additional activities that are not identified in the current award, and Type 7 (change of Institute/Division; competing continuation)—that is, transfer of the legal and administrative responsibility for a grant-supported project or activity from one legal entity to another before the completion date of the approved project period (https://grants.nih.gov/grants/how-to-apply-application-guide/prepare-to-apply-and-register/type-of-applications.htm).
Given the focus of this portfolio analysis on research grants only, we did not include funding by means of Research and Development Contracts or by Other Transactions Authority (OTA). The OTA is an infrequent used funding mechanism available to the NIH for unique circumstances and is not a grant, and thus was not captured in our analysis.
A total of 3,889 grants resulting from the search were manually curated by reviewing the abstract and specific aims for relevance. Two reviewers (E.A. and J.R.) reviewed each grant independently; discordances were resolved by discussion. A total of 1,901 applications were deemed to be not related to maternal health. The remaining 1,988 applications were categorized according to research focus, relevance to CVH, type of research (basic, clinical applied, clinical trial, and translational), stage of pregnancy (pre-pregnancy, pre-partum, peri-partum, which we defined as the period shortly before, during, and immediately after giving birth, and post-partum, which we defined as up to 1 year after giving birth), and the use of e-Health (the use of information and communication technology to support health and health care).
Research focuses were then organized into broader categories of conditions related to CVH and not related to CVH (Supplementary Appendix SA1). Federal Agencies were grouped into National Heart, Lung, and Blood Institute (NHLBI), Other NIH Institutes and Centers (ICs), and non-NIH DHHS Agencies (consisting of CDC and AHRQ).
Results
Over the period of FY 2016–2021 DHHS agencies awarded $948,662,208 for 1,988 grants in maternal health, of which $576,468,462 was for 1,355 grants that are Type 1 (new) (Table 1). There was an absolute growth in overall funding in maternal health from $114,724,727 in 2016 to $346,497,735 in FY 2021, a threefold increase, with the largest increase occurring in FY2021. Our manual review of the individual grants revealed that this large spike in FY 2021 was due to a number of large network grants that were renewed (i.e., Type 2 awards) during that year. There was more linear growth in Type 1 (new) grants, from $88,155,228 in FY 2016 to $145,445,104 in FY 2021, reflecting a 65% increase.
Type of grant refers to stage of grant.
DHHS agencies refer to NIH, CDC, and AHRQ.
Type 1 grant: New Project. Initial request for NIH to fund a project that has not been funded before. Type 1 applications compete with other applications in peer review for funding.
Type 2 grant: Renewal Requests an additional funded project period after the current award. Type 2 applications compete with other applications in peer review for funding.
Type 3: Competing Revision or Administrative Supplement:
Competing Revision: Requests additional funds during an ongoing project period to support new activities that were not identified in the current award. Because the request expands the scope of the award, revision applications need peer review.
Administrative Supplement. Requests additional funds during an ongoing project period to pay for necessary items or activities required due to unforeseen circumstances. Because the request is within the scope of the original award, administrative supplements do not require external peer review.
Type 7: Change of Recipient or Training Institution.
Transfers the rights to and obligations of a grant from one entity to another before the end of the project period
AHRQ, Agency for Healthcare and Research and Quality; CDC, Centers for Disease Control and Prevention; DHHS, U.S. Department of Health and Human Services; NIH, National Institutes of Health.
Table 2 provides an assessment of the portion of all grants awarded by DHHS that were on maternal health topics, stratified by those funded by the NHLBI, other NIH ICs, and the non-NIH DHHS Agencies. The proportion of the total funding allocated to maternal health across DHHS was relatively small, averaging 1.4% overall with little evidence of growth over the years except for the aforementioned large network renewal grants in FY 2021 in the other NIH ICs category, increasing the maternal health proportion to 2.8% in that year. In the non-NIH HHS Agencies category renewals increased the maternal health funding in 2018 (4.3%) and 2020 (8.5%) for relatively smaller amounts.
Dollars and Percent of All Awards by Year in Fiscal Years (FY) 2016–2021 for Maternal Health Research in FY 2016–2021 for National Heart, Lung, and Blood Institute, Other National Institutes of Health (NIH) Institutes and Centers, Non-NIH U.S. Department of Health and Human Services (DHHS) Agencies, and Combined DHHS Agencies
NHLBI, National Heart, Lung, and Blood Institute; FY, fiscal years; ICs, Institutes and Centers.
Maternal health funding specifically for research on CVH amounted to $278,926,105 for 755 grants from FY 2016 to 2021, of which $191,344,649 was for 534 Type 1 (new) grants (Table 3). Funding for Type 1 grants related to CVH showed a twofold increase from 2016 to 2021. However, grants and overall funding for maternal health not related to CVH far exceeded those for CVH, with $669,736,103 for 1,233 grants allocated to areas not related to CVH (Table 4).
Number and Dollars Awarded by Year in Fiscal Years 2016–2021 by Type of Grant Related to Cardiovascular Health for Combined U.S. Department of Health and Human Services Agencies
Maternal Health Grants Related to Cardiovascular Health and Not Related to Cardiovascular Health by Year in Fiscal Years 2016–2021 for Combined U.S. Department of Health and Human Services Agencies
CVH, cardiovascular health.
Over the 6-year period under review, overall funding for maternal CVH research grew from $29,992,347 in 2016 to $77,932,859 in 2021, a 159% increase, whereas funding for non-CVH maternal-health research grew from $84,732,380 to $268,564,876, a 217% increase. There was especially strong growth for maternal CVH grants in 2020 and 2021, and for non-CVH-related maternal-health grants in 2021 (Table 4 and Fig. 1).
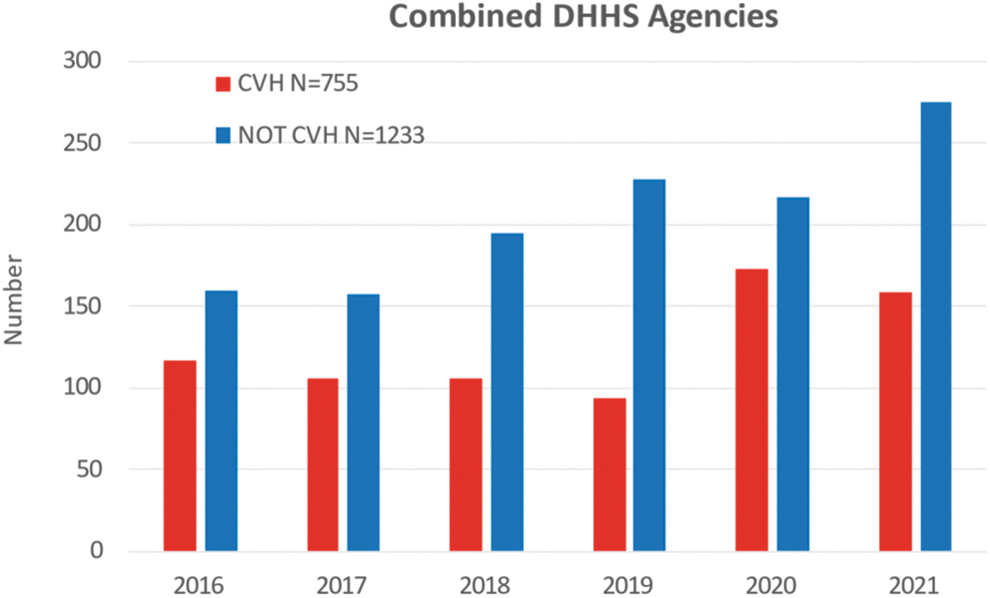
Grants related to CVH and not related to CVH over the years. CVH, cardiovascular health.
The distribution by relationship to maternal CVH varied by agency grouping—for NIH ICs other than NHLBI, the great majority of support was for conditions not related to CVH (mainly HIV and other infections), whereas the reverse was true for NHLBI and for non-NIH HHS agencies where most grants were for conditions related to CVH (Fig. 2). Though all agency groupings showed growth, there was a notable relative jump in CVH grants for NHLBI in FY 2020 and FY 2021, and in non-CVH grants for other NIH ICs in FY 2021 (Supplementary Appendix Tables SA1–SA3). The numbers of grants for non-NIH DHHS agencies vary by year, but represent relatively smaller dollar amounts.
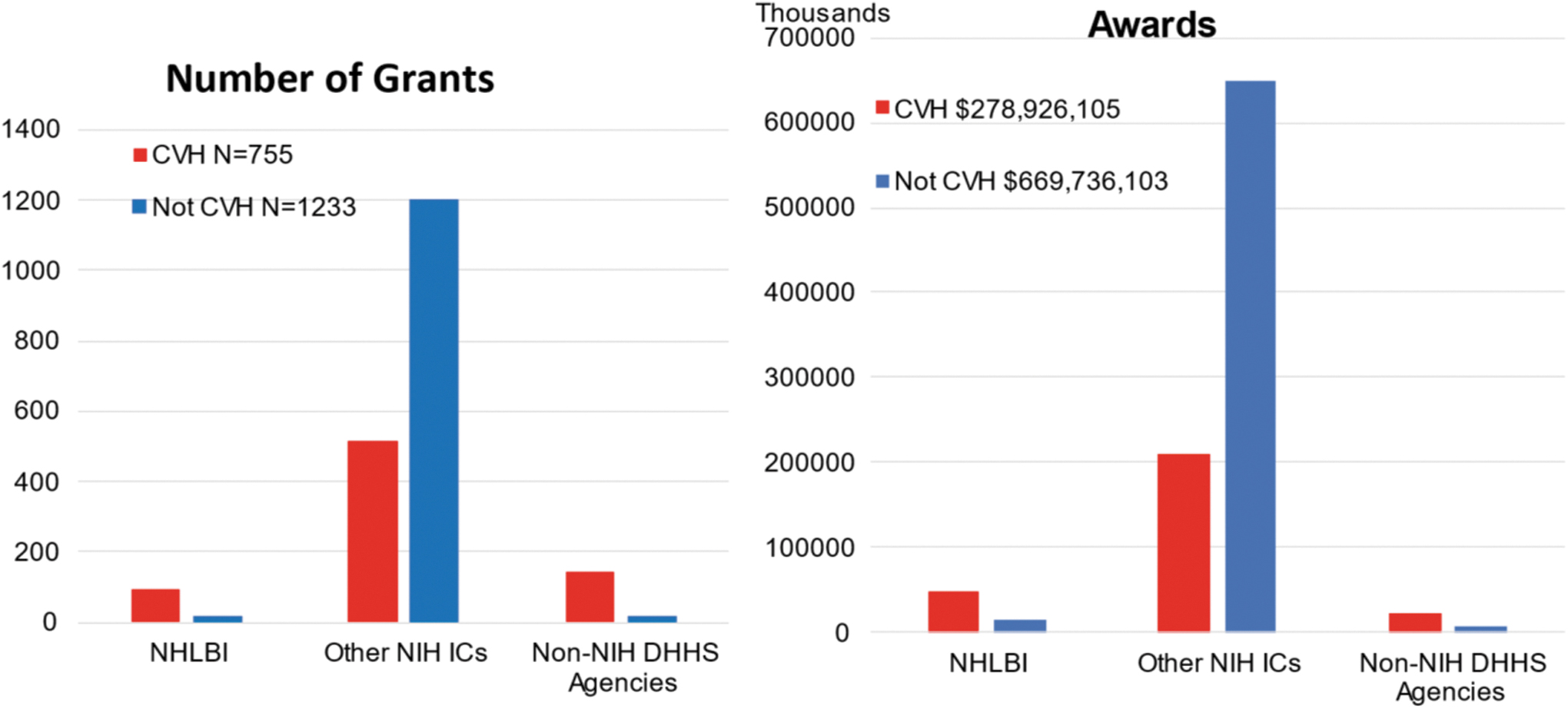
Maternal health grants by funding organization 2016–2021.
Collectively, the most commonly studied condition related to CVH was in the category of general maternal health (Table 5 and Fig. 3). General maternal health refers to grants that include consideration of maternal health without specifying clinical outcomes or exposures, or preventive care, health monitoring, behavioral interventions, physical activity, and short interpregnancy intervals (Supplementary Appendix SA1).
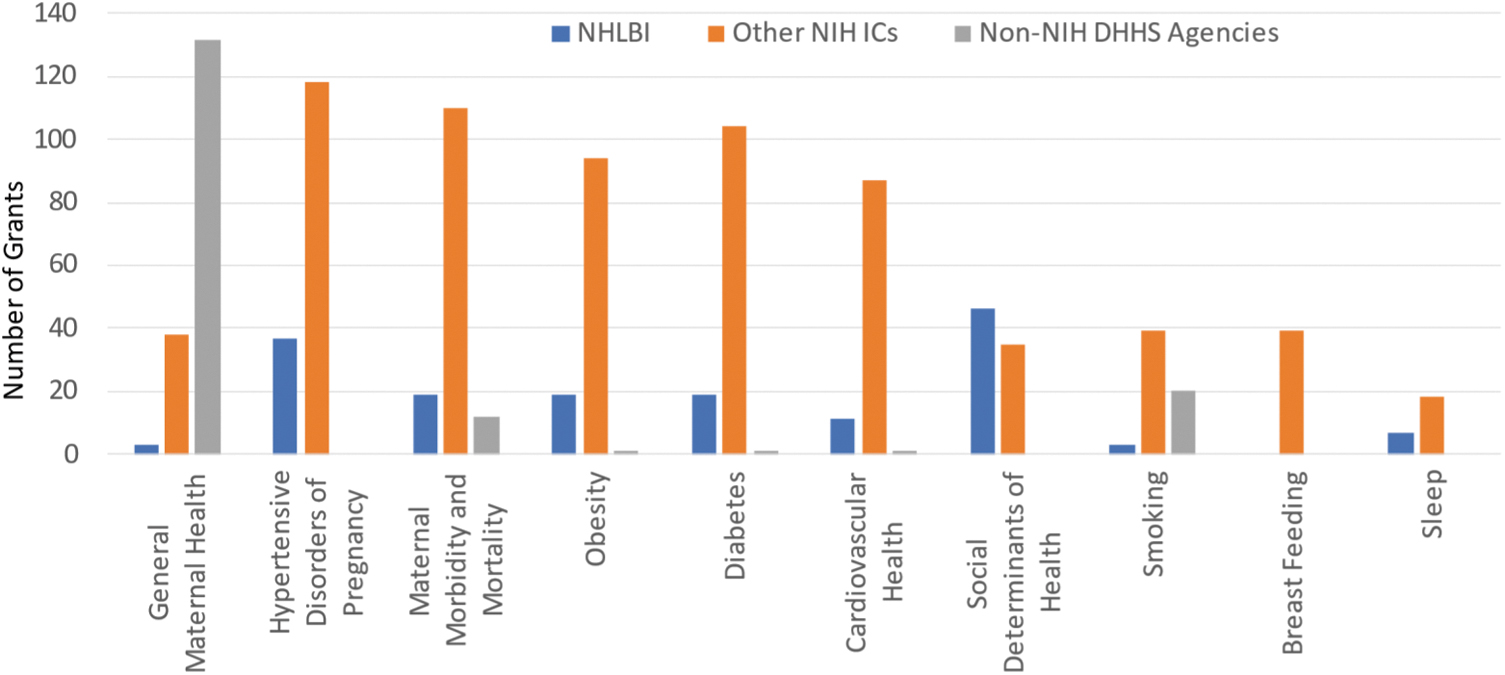
Grants by categories of maternal conditions related to CVH.
Number and Percentage of All Grants by Category of Maternal Condition Related to Cardiovascular Health in Fiscal Years 2016–2021 for National Heart, Lung, and Blood Institute, Other National Institutes of Health (NIH) Institutes and Centers and, Non-NIH U.S. Department of Health and Human Services (DHHS) Agencies, and Combined DHHS Agencies
Awards not calculated because grants may include more than one condition.
Sum of conditions is larger than the sum of the grants.
Most grants funded by non-NIH DHHS agencies were in this area of CVH-related research, whereas most grants by NHLBI and other NIH ICs focused on HDP, maternal morbidity and mortality, obesity, or diabetes. A large proportion (50.5%) of NHLBI grants specifically studied CVH (including cardiometabolic health), and 38.7% studied HDP. Importantly, given the additive effects of SDOH above and beyond other risk factors, about 16% of grants included consideration of SDOH, with similar proportions in NHLBI and in other NIH ICs.
Smaller proportions of NIH grants studied smoking, breast feeding, or sleep. Note that many grants covered more than one area of research, so that the total number of conditions exceeds the number of grants. For this reason, it was not possible to calculate the dollars allocated to each area of research.
Clinical applied research involving human subjects, including epidemiological, behavioral, outcomes, and health services research (we considered clinical trials separately), was the most common type of research in DHHS, particularly in the case of non-NIH DHHS Agencies (Table 6). NIH grants also had a large proportion of clinical applied research, but in addition had substantial proportions of grants classified as basic research, clinical trials, and/or translational.
Characteristics of Grants Related to Maternal Cardiovascular Health in Fiscal Years 2016–2021 for National Heart, Lung, and Blood Institute, Other National Institutes of Health (NIH) Institutes and Centers, Non-NIH U.S. Department of Health and Human Services (DHHS) Agencies, and for Combined DHHS Agencies
Awards not calculated because grants may include more than one characteristic. Sum of characteristics is larger than the sum of the grants.
Late stage clinical trials, in addition to n = 24 pilot studies included in other categories.
NHLBI had relatively fewer clinical trials and/or translational grants compared with other NIH ICs; the latter is due mostly to the large number of grants in the Eunice Kennedy Shriver National Institute of Child Health and Human Development NICHD's Maternal-Fetal Medicine Units (MFMU) network (https://www.nichd.nih.gov/research/supported/mfmu) (data not shown). e-Health featured in 9.7% of NHLBI grants and 14.5% of other NIH IC grants.
Most NHLBI and other NIH IC grants studied participants in the pre-partum period (78.5% and 77.7%, respectively), followed by the post-partum period (50.5% and 37.6%, respectively), with relatively fewer in peri-partum, that is, during the immediate delivery period (9.7% and 20.3%, respectively), and even less in pre-pregnancy (10.8% and 9.9%, respectively) periods (Table 5). High proportions of grants from Other DHHS Agencies included all phases of pregnancy due to the large number of grants in the CDC-funded PRAMS (Pregnancy Risk Assessment and Monitoring System) program (data not shown). 13
The data from PRAMS are retrospectively derived from questionnaires completed by women who have had a live birth. Grants could include more than one type of research, and more than one stage of pregnancy, thus it was not possible to calculate the dollars allocated to each category.
Discussion
We aimed at examining trends in Federal funding for maternal health research and more specifically research into maternal CVH, given increasing concerns about excess maternal morbidity and mortality in the United States. We found that funding for maternal health has been increasing over the period of FY 2016–2021; however, this funding has remained a relatively small component, averaging 1.4% of total grant funding. In other words, funding for maternal health research during this period simply kept pace with the secular increase in total grant funding.
The areas of funded research in maternal and CVH were aligned with the missions of the respective ICs/Agencies. CVH itself predominated in NHLBI grants, followed by HDP. For the other NIH ICs, grants were more evenly spread across the different categories of CVH related to maternal health (Supplementary Appendix SA1). Grants by non-NIH DHHS Agencies featured general maternal health almost exclusively. Overall, grants specifically related to CVH increased over time at about the same rate as grants not related to CVH.
With respect to the phase of pregnancy studied, we found that most NHLBI grants studied participants in the pre-partum period, followed by the post-partum period, with relatively few in the pre-partum and peri-partum periods The peri-partum period was somewhat better represented in other NIH IC grants; however the pre-partum period was the most underrepresented there. This represents a potential opportunity for funding agencies to consider further fostering research, particularly in the pre-pregnancy period.
Pre-pregnancy CVH in the United States has been shown to be associated with risk of adverse pregnancy outcomes (APOs), including a recent analysis of National Center for Health Statistics data that found a consistent and graded association between worse CVH in pre-pregnancy and later APOs. 14 Given that the majority of pregnant women in the United States have unfavorable CVH before pregnancy, 15 more prospective and mechanistic studies of risk factors as well as clinical trials on CVH promotion or preventive treatment during the pre-pregnancy phase would be desirable.
A recent AHA Scientific statement noted that “Because the biological processes leading to adverse pregnancy outcomes begin before conception, interventions focused only during pregnancy may have limited impact on both the pregnant individual and offspring. 16 ” Hence, earlier intervention could also offer great promise of preventing or mitigating the consequences of unfavorable health on maternal outcomes, as opposed to intervening only during the limited early pregnancy time window.
Regarding the characteristics of research, a future greater emphasis on explanatory clinical trials and clinical translational research including implementation science could also provide opportunities to advance the field by facilitating clearer evidence-based pathways to prevention and treatment. The importance of further fostering these types of research has been recognized by the NHLBI and the NIH. With respect to implementation science, in late FY 2020 the NHLBI used the OTA funding mechanism to establish the Maternal Health Community-Implementation Project (MH-CIP).
The MH-CIP was created to fund community-driven research projects in areas of high maternal morbidity and mortality to test implementation strategies to increase uptake and adoption of proven interventions to improve maternal health and address maternal health inequities. Four research projects have been funded and are actively conducting maternal health implementation science projects in their communities.
In FY 2022, the NHLBI established another maternal CVH initiative, the multi-center clinical trial titled Early Intervention to Promote Cardiovascular Health of Mothers and Children (ENRICH). The purpose of the ENRICH trial is to test the effectiveness of an implementation-ready intervention, delivered in the context of home visiting programs, in enhancing maternal and early childhood CVH (https://grants.nih.gov/grants/guide/rfa-files/RFA-HL-22-007.html and https://grants.nih.gov/grants/guide/rfa-files/RFA-HL-22-008.html).
The trial is ongoing and anticipates completion in FY 2029. In FY 2023, the NIH IMPROVE (Implementing a Maternal health and Pregnancy Outcomes Vision for Everyone) Initiative will be awarding its Centers of Excellence, for which several clinical trials are intended to be included in the funding (https://www.nichd.nih.gov/newsroom/news/081622-IMPROVE-CoE). The IMPROVE initiative supports research to reduce preventable causes of maternal deaths and improve health for women before, during, and after delivery with an emphasis on health disparities and populations that are disproportionately affected, including racial and ethnic minorities.
The IMPROVE initiative will also plan to fund in FY 2023 multiple implementation science projects as per its other two funding announcements—that is, Notice of Special Interest: Implementation Science to Advance Maternal Health and Maternal Health Equity for the IMPROVE initiative (https://grants.nih.gov/grants/guide/notice-files/NOT-HD-22-043.html); and Research Opportunity Announcement: IMPROVE Community Implementation Program Solicitation for Research Coalitions (https://www.nhlbi.nih.gov/sites/default/files/media/docs/IMPROVE-CIP_ROA_FINAL_508C.pdf).
This analysis has several strengths, the most prominent of which is the detailed manual curation of many grants. Electronic data extraction and classification is much easier and faster, but for our purposes would have led to substantial misclassification. For example, fully half of the grants classified as being related to maternal health using RCDC terms in iSearch were ultimately deemed upon manual curation to not be related to maternal health.
During the curation, we frequently encountered other examples of misclassification, for example in whether a grant included a clinical trial. The manual curation allowed for subclassifications into important categories such as area of research, type of research, use of E-health, and stage of pregnancy. Inclusion of grants funded by other DHHS Agencies is another strength.
There are some weaknesses to acknowledge. The period under review is relatively short for study of secular trends in funding, and for some categories of interest we could not assign dollar values (because of overlap between categories). Also, funding mechanisms such as OTA and contracts are not captured in iSearch. Finally, while it is an overall strength, manual curation necessarily involves judgement and interpretation. We tried to minimize this by having two independent reviewers who needed to reach agreement; however, a different set of reviewers might come up with somewhat different results.
Conclusions
During FY 2016–2021, Federal grant funding for maternal health and specifically for maternal CVH increased at the same rate as overall research funding. We did not find evidence that maternal health was prioritized over other areas of research during that period. We realize that since FY 2021, NIH and DHHS have begun to create initiatives to mitigate the rising maternal morbidity and mortality in the United States.
Possibly, it may be too early to see the full extent to which recent public and professional focus on the poor statistics on maternal health in the United States will translate into sustained growth in research funding. Although funded studies cover the spectrum of maternal health conditions related to CVH, the pre-pregnancy period is particularly understudied. Clinical trials could help to validate and refine health promotion and preventive treatment options, and implementation studies of known effective interventions might also move the field forward.
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the views of NHLBI, the NIH, or the DHHS.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding associated with this manuscript.
Supplementary Material
Supplementary Appendix
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.