
Abstract
Background:
Women Veterans have unique health care utilization patterns; however, video-based primary care utilization among and between women and men has not been well examined.
Methods:
In a retrospective cohort study, we calculated gender-stratified video visit adoption (i.e., likelihood) and frequency (i.e., rate of use among users) between April 1, 2020, and March 31, 2022, by demographic and clinical characteristics known to impact health care utilization.
Results:
Among 5,389,139 Veterans (9.2% women), 32% of women and 18.6% of men had a video-based primary care visit over the 2-year study period. Gender interacted with Veteran characteristics and the likelihood of any video care. Men often had associations stronger in magnitude (both positive and negative) than women, including by age, rurality, history of housing instability, mental health conditions, and marital status. The direction of effect never diverged by gender. A positive association among women always coincided with a positive association among men, and vice versa, across all characteristics assessed. Only the risk ratio for video care use comparing Veterans of Black race with White race was stronger among women. In contrast to the video care adoption differences by gender, we found few differences in the frequency of video-based care by gender.
Conclusions:
The findings suggest there are fewer disparities by demographic and clinical characteristics in any video care use among women compared with men and little to no disparities in the frequency of video care use by gender. Understanding the variation in video care utilization by gender could help improve acceptance, appropriate utilization, and uptake of video-based visits for all.
Introduction
Equitable access to health care could be increased through virtually delivered health care (e.g., via phone or video), which offers increased flexibility and convenience by eliminating the need for transportation, lowering patient costs, and reducing lost work time. 1 –10 Video-based care has been identified as an especially promising tool to improve access to high-quality care for women. 11 Although women attend more outpatient health care visits, many also face gender-specific access barriers, such as disproportionate child care constraints and caregiving responsibilities. 12 Access to health care is particularly challenging for women with disabilities and those from minoritized populations who may face additional difficulties related to cost, inaccessible equipment, transportation facilities, and discriminatory attitudes. 13,14 Video-based care obviates the need to travel to a health care provider, which reduces the competing time demands and other barriers related to transportation (e.g., access, convenience, and affordability). 15 Video care can also facilitate more trusting relationships with clinicians and surmount barriers generated by unwelcoming environments, such as those created by stranger harassment or by clinicians without adequate training and awareness of gender- and sex-based care needs. 16 –19 Recent gender-specific patterns in the utilization of video-based care suggest that this modality holds promise. As compared with men, women are ready users of web-based and mobile resources for health care information. 20,21 In addition, evidence from early in the COVID-19 pandemic suggests that women used virtually delivered care at higher rates than men. 22,23
The Veterans Health Administration (VHA) offers a rich environment to explore sex and gender-based differences in the uptake and use of video-delivered health care. The VHA has a well-developed telehealth infrastructure, providing both phone- and video-based care, that predates the rapid expansion in March 2020 because of COVID-19 shelter-in-place orders. 24 Similar to other health care systems, VHA rapidly expanded its provision of virtual care and has since integrated virtual care as a common modality. 25 By 2022, virtual care comprised approximately 30% of VHA outpatient care, 10% of which was provided by video. 23 Although the majority of VHA virtual care is conducted via telephone, VHA leadership has indicated that video-based care is preferred over telephone-based care because of its potential to provide a more comprehensive clinical experience. 22,24 Video-based care increases access to treatment, improves patient satisfaction, reduces costs to patients, 3 –6,10 and may provide effective follow-up. 26 In addition, in response to the rapid growth of the women Veteran population, the VHA has intentionally developed a health care delivery approach that recognizes women as a distinct patient population (e.g., comprehensive women’s health care policy, which created a workforce of dedicated women’s health primary care providers). 27 –29 To inform policy and optimize practice in virtual care delivery, we examined differences in the use of video-based health care visits between men and women. Specifically, we evaluate variation between men and women in the adoption of video-based care and the frequency of video-based care by key characteristics known to impact health care utilization.
Methods
Data sources and study population
Veteran patient data and outpatient encounter history were extracted from VHA electronic health records. 30 Our cohort comprised Veterans who were actively engaged in care in the year before the start of the COVID-19 pandemic (March 11, 2020) and the subsequent widespread adoption of virtual care. 22,23 We excluded Veterans who were deceased as of April 1, 2020 (<1 month of follow-up) and those with missing data on their home zip code or priority enrollment group (<0.5% combined). The analytic cohort comprised 5,389,139 Veterans who met all the criteria.
Outcome
Our primary outcome was having a video-based primary care outpatient visit between April 1, 2020, and March 31, 2022. Outpatient primary care encounters were identified and classified by modality (video, in-person, or phone) using stop codes. 22,23 We restricted to encounters that met evaluation and management criteria to focus on encounters where a physician, or other qualified health care professional, diagnoses or treats injury or illness (Supplementary Data S1). 22,23
Veteran patient characteristics
We identified a priori key demographic characteristics like predisposing factors (i.e., gender, age, race, ethnicity, and marital status), enabling factors (i.e., income and rurality), and clinical characteristics such as need factors for health care utilization (i.e., disability status, history of housing instability, chronic conditions, and mental health conditions). 31 –33 Veteran patient characteristics (Table 1) were identified during the baseline period (March 11, 2019–March 10, 2020).
Characteristics of 5,389,139 Veterans at the Veterans Health Administration in the United States Stratified by Gender
VHA, Veterans Health Administration.
We defined gender using birth sex data captured in each patient’s electronic health record. These data document the Veteran’s sex assigned at birth, but Veterans can opt to update their birth sex to reflect their gender. 34 Therefore, these data are likely capturing some combination of sex and gender for Veterans. We note that sex (biological characteristics typically identified at birth) and gender (a construct representing the sociocultural experiences and identity of an individual) are separate concepts. Data are less reliable for nonbinary or gender-nonconforming Veterans who may be unable to record their gender identity at VHA owing to a lack of trust or a lack of options in VHA electronic health records.
We defined Veteran race and ethnicity as the most frequent self-identified value in patient health records. Missing data on race, ethnicity, or marital status were treated as distinct categories. Veterans home addresses were classified into urban, rural, and highly rural designations based on the zip code of their home addresses. 22,35 We incorporated information from VHA’s priority-based enrollment system, which categorizes Veterans into eight groups based on their disability rating, income, recent military service, and other factors. 35 We further categorized Veterans into the following four condensed groups: high disability, low/moderate disability, low-income, and no special enrollment considerations (Supplementary Data S2). History of housing instability was defined using stop codes and International Classification of Disease, Tenth Edition diagnosis codes in the baseline period (Supplementary Data S3). 7 We calculated the number of chronic conditions and history of a mental health condition for each Veteran (Supplementary Data S4 and S5). 22,36 –39 We also assessed prior utilization of VHA care, which included outpatient encounters between March 10, 2019, and March 10, 2020, classified by care modality (in-person, phone, and video-based care) and by type of care (primary care, mental health, specialty, and diagnostic/ancillary care). 22
Statistical analysis
We used a two-part modeling framework to identify patient demographic and clinical characteristics associated with the risk or likelihood of using any video-based primary care and then, among those with a primary care video visit, assessed the annual rate or frequency of use. First, we used Poisson regression to model the likelihood for any use of video-based primary care among all Veterans. Second, we used a zero-truncated negative binomial model with a log link to model the count of video-based primary care encounters, conditional on prior video care use. To account for variation in the rate of video care use owing to a variation in a Veteran’s utilization of primary care (e.g., Veterans with higher clinical need have more primary care encounters overall), we included an offset in the negative binomial model for the log of total primary care encounters for each Veteran in each year. 40
We fit models separately for women and men. In each model, we adjusted for age, race, ethnicity, marital status, rural/urban status, VHA priority enrollment group, history of housing instability, VHA medical facility of the Veterans Primary Care Management Team, number of chronic conditions, presence of a mental health condition, and baseline prior utilization of VHA services by care type and modality. Standard errors were clustered at the Veteran level to account for the 2 years of observation. We report adjusted risk ratios (RR) for any video care use and adjusted incidence rate ratios for the annual rate of video care use stratified by gender over the 2-year period, with a more conservative confidence interval (CI; 99.75%) to account for multiple comparisons.
To identify differences in risk ratios for demographic characteristics and the use of video-based primary care between women and men (i.e., interaction effect by gender), we also calculated the ratio of the risk ratio (RRR). The RRR is a well-established test of interaction to compare estimates on a log scale, and the reported p-value from these stratified estimates is equivalent to the p-value obtained from one model with an interaction. 41,42 The RRR can be used to understand if the likelihood difference in video utilization for a given patient characteristic (e.g., younger vs. older Veterans) is different for women versus men. We report the RRR (RR women/RR men) and its associated 99.75% CI and p-value (α = 0.0025). An RRR > 1 indicates that the RR for a given characteristic is larger in magnitude among women than men, whereas an RRR < 1 reflects a smaller magnitude among women than men. Careful attention should be paid to the direction of the RR (e.g., lower or higher risk) when interpreting the RRR, as a RR > 1 may reflect a larger positive magnitude among women (2/1 = 2) or a larger magnitude of a protective effect among men (0.9/0.5 = 1.8).
To assess if the use of video care differed across the 2 years, we examined the likelihood and rate of video care in year 1 (April 1, 2020–March 31, 2021) and year 2 (April 1, 2021–March 31, 2022) of follow-up in separate models. As a secondary analysis, we examined differences in the adoption of and frequency of phone care (e.g., audio-only), as barriers may differ. All statistical analyses were conducted in Stata 17 (StataCorp, LLC). This evaluation was conducted as part of the Virtual Access
Results
Among the 5,389,139 Veterans in our cohort, 9.2% were women. Overall women were on average younger, more racially diverse, and more ethnically diverse (i.e., a higher proportion of Hispanic ethnicity) (Table 1). Compared with men, a larger proportion of women were single, divorced, or widowed and living in urban areas. Women were more frequently rated with a high disability rating and were less frequently included in the low-income priority group for VHA enrollment. Men, on average, had more chronic conditions (mean 2.8 vs. 2.4), yet a higher proportion of women had a history of a mental health condition (49.2% vs. 32.7%) or history of housing instability than men (5.2% vs. 3.9%).
Between April 1, 2020, and March 31, 2022, approximately, 1,069,347 Veterans had at least one video-based primary care encounter. A larger percentage of women than men had a primary care outpatient encounter of any modality (90.4% vs. 88.2%) and 32.0% of women compared with 18.6% of men had a video-based visit (Fig. 1). Men had a slightly lower percentage of virtual (phone and video) and in-person encounters than women (Fig. 1).
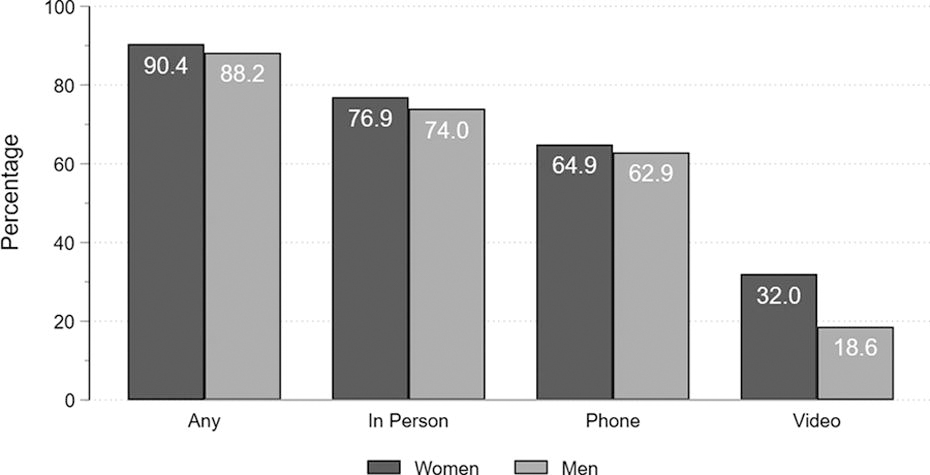
Percentage of 5,389,139 Veterans with a primary care evaluation and management encounter between April 1, 2020, and March 31, 2022: stratified by encounter modality.
Adoption of video care
Although there is variation in the adoption of video-based primary care, both within and between men and women by some demographic and clinical characteristics, there were no instances where the effect for men and women diverged in direction. In other words, a positive association among women always coincided with a positive association among men, and vice versa, across all demographic and clinical characteristics assessed. However, the strength of association (i.e., magnitude of effect) differed between men and women by age, rurality, history of housing instability, presence of mental health conditions, marital status, and Black race.
Patient characteristics such as age, rurality, history of housing instability, having a mental health condition, and being in the low-income priority group were associated with a lower likelihood of adoption of video-based primary care among both men and women (Fig. 2). In adjusted models, both men and women had a lower likelihood of using video-based care with increasing age. Among women, each decade in age was associated with an 8% lower likelihood of having a video care encounter (RR 0.92 [99.75% CI: 0.92, 0.92]), although among men each decade was associated with a 15% decrease (RR 0.85 [0.84, 0.85]). This negative association was 9% stronger among men (RRR 1.09 [1.08, 1.10]). Among both men and women, rural and highly rural Veterans had a lower likelihood of having a primary care video-based encounter compared with urban dwelling Veterans. This negative association between rural and urban Veterans was 6% stronger among male Veterans (RR 1.06 [1.04, 1.08]) but not among highly rural Veterans. Both men and women with a history of housing instability or a mental health condition had lower likelihood of using video care. The negative association of a history of housing instability and the likelihood of using video care was stronger among men (RRR 1.12 [1.09, 1.16]). Both men and women classified as low income in priority enrollment groups had similar lower likelihoods of having any video care compared with Veterans enrolled without special considerations.

Adjusted risk ratios (99.75% CI) for any use of video-based primary care among 5,389,139 Veterans between April 1, 2020, and March 31, 2022, stratified by gender. Age was mean-centered, and rescaled such that risk ratios correspond to a 10-year increase in age from 66 years of age. Models adjusted for variables in tables, missing race, missing ethnicity, VHA medical center, and prior utilization of VHA health care by care type and modality as fixed effects. CI, confidence interval; RR, risk ratio; RRR, ratio of the risk ratio; VA, U.S. Department of Veterans Affairs; VHA, Veterans Health Administration.
Patient characteristics such as identifying as Black or American Indian/Alaska Native, having disability considerations for VHA enrollment, being married, and a greater number of chronic conditions were associated with a higher likelihood of video care adoption. Black women had an 11% higher likelihood of using video care than White women (RR 1.11 [1.10, 1.13]). This association was weaker among men (RR 1.06 [1.05,1.08]) as Black men had a 5% higher likelihood of any video care than White men (RR 1.05 [1.04, 1.05]). There was a slight, but likely clinically insignificant, increase in the risk ratio for video care for American Indian/Alaska Native Veterans compared with White Veterans for both men and women with no evidence of an interaction effect by gender (i.e., null RRR). Married men and women were 17% and 5% more likely, respectively, to have a video care appointment compared with single men and women (with a RRR 0.90 [0.88, 0.91]) reflecting the larger magnitude in positive association among men. There was an increasing exposure–response relationship between the number of chronic conditions and the likelihood of video care among both men and women. The largest effects were seen among Veterans with five or more chronic conditions. Both men and women enrolled with low/moderate disability considerations (e.g., VHA priority enrollment group) had similar higher likelihoods of having a video encounter than Veterans enrolled without special considerations. There were no differences in video-based primary care adoption by Hispanic ethnicity or other race groupings such as Asian and Native Hawaiian/Other Pacific Islander for both women and men.
Frequency of video care
Among both women and men who used video-based primary care, there were very minor, mostly negligible associations between patient demographics and the frequency of video care use. Veterans who were low income had lower rates of video care use, and this association was slightly stronger among men. An increase in the number of chronic conditions was associated with a decreased rate of video-based care utilization, and this pattern was similar among men and women (Supplementary Table S1).
Secondary analysis: Adoption of and frequency of phone care
The adoption of phone-based primary care between men and women showed similar patterns as video-based care for Veteran characteristics such as race, ethnicity, history of homelessness, number of chronic conditions, and presence of a mental health condition (Supplementary Fig. S1). We did not see differences in the adoption rate of phone-based care among Veterans who were older, more rural, or lower income, where we identified a lower adoption rate of video-based care.
The frequency of phone-based primary care between men and women was similar to the patterns identified for video care across where the risk ratios for most characteristics showed negligible differences by Veteran characteristics (Supplementary Table S2). An increase in the number of chronic conditions was associated with a decrease in the rate of phone care for both men and women.
Sensitivity analysis
There were differences in the proportions of Veterans with a primary care visit between the 2 years of the pandemic (Supplementary Fig. S2). More Veterans had a video care encounter in the first year (April 1, 2020, through March 31, 2021) than in the second (April 1, 2021, through March 31, 2022). In both years, a higher proportion of women used video care than men. Sensitivity analyses examining the adoption of and frequency of any video care or phone care between the two years of follow-up were similar (data not shown).
Discussion
In this large nationwide evaluation of Veterans, several factors known to influence the adoption and frequency of video-based primary care were found to interact with gender. We found no divergent associations by gender, and nearly all gender interactions had stronger associations among men. Gender-tailored care at VHA for women’s specific health needs may explain our findings of no divergent associations by gender and less extreme differences in video care use among women than men for Veteran characteristics known to impact health care utilization. Although some Veterans groups had lower adoption rates of video care, our findings support that there are no excessive additional impacts of gender on video care uptake that would impact men and women with divergent associations.
With only one exception, whenever there was a gender interaction effect for the use of video-based primary care and a Veteran characteristic, men Veterans had a stronger association (both positive and negative) than female Veterans. For example, being married is associated with an increased adoption of video care for all Veterans, but this association was much stronger among men. This finding may reflect the supportive nature of having a partner who can help advocate for and coordinate health care utilization for their partner or who may be able to assist in the technical aspects of video-based care. The stronger effect of increased video care use among married men could indicate that married women do not receive as much health care support from their partners as men do, or alternatively, their partner’s support doesn’t confer as much additional benefit. Men Veterans also had larger decreased risk ratios for video care use compared with women regarding older age, increased rurality, history of housing instability, and presence of a mental health condition. Each 10-year increase in age was associated with a 15% decreased risk among men but only an 8% decreased risk among women. Men who were married (compared to single) or who had an increased number of chronic conditions (compared to fewer chronic conditions) had larger increased risk ratios for video care use compared with women. These more extreme associations among men paired with more tempered associations among women, indicate fewer or weaker disparities in video care adoption among women by key Veteran characteristics. Our results suggest more egalitarian care access among women Veterans than male Veterans.
Only when evaluating the risk ratios for video care use comparing Black or African American Veterans with White Veterans was the association stronger among women. This gender difference may reflect the preference of Black women Veterans to seek care virtually. Black women Veterans may find in-person encounters less welcoming than virtual visits owing to high rates of military sexual trauma in this population, as well as higher rates of experiences with discrimination and stranger harassment when receiving VHA care. 16,43,44 In addition, Black women may prefer video care because of opportunities to accommodate challenging work schedules or child care demands. Moreover, Black women also disproportionately use a mobile device as their primary source of internet connection, 45 which may increase their comfort with and empowerment to use video-based care.
Similar to previous analyses, we found that older age, rurality, a history of housing instability, the presence of a mental health condition, and enrollment in the low-income priority group category were associated with a decreased likelihood of primary care video adoption. 46,47 In addition, akin to prior analyses, we also found that Veteran characteristics such as being Black or African American, having disability considerations for VHA enrollment, and having more chronic conditions were associated with increased video adoption. 48 –50
In contrast to previous findings, the frequency of video care and phone care decreased with increasing chronic conditions among men and women. 23 This is likely because the offset in our models accounted for the variation in the frequency of care that is due to the total number of encounters. 40 Because an increase in the number of chronic conditions is correlated with an increased number of all primary care encounters (i.e., sicker Veterans have more health care encounters, including in-person, video-based, and phone-based), when models do not adjust for the exposure denominator of total visits, the rate ratio for the number of chronic conditions is likely picking up variation in the rate of video care that would be explained by the total number of primary care encounters. 40 In short, our models account for the utilization of all primary care encounters, whereas prior work does not and may have biased estimates because of failing to include this consideration.
Our secondary analyses for any use of phone-based care reflect, for the most part, an attenuation of the within and between gender differences found for the likelihood of video care. Therefore, phone-based care may be a more equitable way for Veterans to receive care as it does not require internet access, sufficient broadband speeds, or a video-capable device. In our sensitivity analysis, we found that the relative risk of and the relative frequency of a video/phone encounter across Veteran characteristics was roughly the same each year despite a decrease in phone and video care use overall in the second year.
Although our evaluation was specific to the VHA, non-VHA health care providers looking to improve health care access for women can learn from the VHA experience and take some reassurance that even in a male-dominated system, we did not see a widespread increase in health care access disparities among women. Our findings suggest that health care systems’ pursuit of virtual care expansion as a way to improve access does not necessarily worsen gender-based access disparities and may even be a route to improve access among Black women.
Several limitations should be noted. First, our results may not generalize to other health care systems, as the VHA was an early adopter of virtual care and offers subsidized care to Veterans. 24 Furthermore, because of distinct demographic patterns in the VHA patient population, including the young average age among women with a history of military service, findings might not generalize to a wider population. However, women Veterans who served in VHA also represent a more diverse and historically marginalized population, which can provide insights for care provided to similar civilian women populations. Second, our dependence on gender data derived from VHA health care records introduced imprecision for gender-diverse Veterans. The VHA is currently collecting self-identified gender identity (SIGI) for all Veterans in VHA health records. However, health care records provide the most complete data, as SIGI records exist for only a small fraction of the VHA population (approximately 80,000 Veterans as of fall 2023). Future work should incorporate patient-reported gender information to ensure that findings more accurately reflect the gender identities of the Veterans who served by VHA. Finally, this evaluation focused on the likelihood and frequency of video-based primary care visits and was not able to account for the underlying need or desire for or availability or appropriateness of a video visit for each Veteran.
Nevertheless, this evaluation has several strengths, including its focus on a national sample of Veterans in a large, integrated health care system with a robust electronic health record. Our evaluation is well powered to detect gender differences in the use of video-based primary care, even among underrepresented groups such as racial minorities in the United States.
Conclusions
This evaluation highlights specific demographic characteristics that influence the likelihood of engaging in video-based primary care among women and men Veterans. Overall, there were minor differences by gender in the frequency of video-based care. The negative link between certain characteristics (e.g., older age, rurality, and mental health) and video-based primary care use was not as strong among women compared with men, suggesting that video-based care is more equitable among women or that women Veterans may be better able to overcome some barriers to video-based care use. Understanding the presence of differences in virtual care use within the women Veteran population could help improve acceptance, appropriateness, and uptake of video-based visits in this prioritized VHA population. Efforts to optimize the tailoring of VHA care for women Veterans have been shown to improve health outcomes, reduce disparities, and improve patient satisfaction among women. 51 –53 Our findings can inform further optimization of the integration of virtual care into care provision for women Veterans with the potential to promote equitable access to care. 54
Footnotes
Acknowledgments
The authors thank James Van Campen, Cindie Slightam, the VA Office of Connected Care, the VA Office of Rural Health, and the Virtual Access Quality Enhancement Research Initiative (QUERI) team, as well as the VA Virtual Care Core for their help in supporting this evaluation. We also thank the Center of Innovation to Accelerate Discovery and Practice Transformation at the Durham Veterans Affairs HealthCare System for their support (e.g., computers and office space).
Authors’ Contributions
All authors contributed equally to the conceptualization and writing (reviewing and editing) of the article. J.M.F.: data curation, methodology, formal analysis, visualization, writing—original draft (lead), and funding acquisition. K.M.G.: writing—original draft (supporting). L.L.Z.: writing—original draft (supporting). D.M.Z.:—funding and resource acquisition and supervision.
Author Disclosure Statement
Views expressed are those of the authors, and the contents do not represent the views of the VA or the U.S. government. The authors have no conflicts of interest or disclosures to report.
Data Sharing Statement
Because of VA regulations and our ethics agreements, the analytic datasets used for this study are not permitted to leave the VA firewall without a Data Use Agreement. This limitation is consistent with other studies based on VA data. However, VA data are made freely available to researchers with an approved VA study protocol. For more information, please visit ![]() or contact the VA Information Resource Center at
or contact the VA Information Resource Center at
Funding Information
Funding was provided by the VA ![]() to learn more. This work was also supported by a VA QUERI Partnered Evaluation Initiative (PEI) 18–205 (PI: D.M.Z.), and J.M.F. was directly supported by a VA QUERI Initiative to Advance Diversity in Implementation Leadership Supplement to the QUERI
to learn more. This work was also supported by a VA QUERI Partnered Evaluation Initiative (PEI) 18–205 (PI: D.M.Z.), and J.M.F. was directly supported by a VA QUERI Initiative to Advance Diversity in Implementation Leadership Supplement to the QUERI
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.