
Abstract
Background:
Pelvic organ prolapse (POP) affects a considerable proportion of women. Limited information exists regarding the incidence of POP as women transition through menopause. Using data from the Study of Women’s Health Across the Nation (SWAN), this diverse community-based longitudinal cohort study assessed the incidence of symptomatic POP and risk by race/ethnicity.
Methods:
Self-reported POP was ascertained by questionnaire at 11 approximately annual SWAN visits over a median of 13.3 years of follow-up. We estimated probabilities for reporting POP using interval-censored Kaplan–Meier survival plots. We estimated hazard ratios (HR) and 95% confidence intervals (CI) using interval-censored Cox proportional hazards models.
Results:
The estimated cumulative probability of POP increased linearly from 2.1% at age 45 to 10.1% by age 65 (4.0% per decade). At age 65, the probability was 4.2%, 4.8%, 8.9%, 9.7%, and 33.9% for Japanese, Chinese, Black, White, and Hispanic women, respectively. Compared with White women, the unadjusted HR for POP was 3.09 (95% CI = 2.18–4.39), 0.96 (0.71–1.31), 0.43 (0.22–0.85), and 0.48 (0.26–0.88) for Hispanic, Black, Chinese, and Japanese women, respectively. After adjustment for financial strain and vaginal birth, the low hazards among Chinese and Japanese women and the high hazard for Hispanic women remained significant.
Conclusion:
Incidence of symptomatic POP increased as women aged through midlife. Risks varied by race and ethnicity and were not accounted for by population differences in socioeconomic life contexts or the probability of having had a vaginal birth. Although not associated with menopause, health providers should incorporate screening for and information about POP when treating menopausal symptoms and health needs of midlife women. Research on pathophysiological factors associated with increasing POP in midlife is warranted.
Introduction
Pelvic organ prolapse (POP) is a common gynecological condition. POP, including uterine prolapse, cystocele, and rectocele, has been diagnosed clinically in 25–50% of postmenopausal women participating in Women’s Health Initiative (WHI) studies. 1 –3 Described as the descent of the bladder, uterus, rectum, or any combination of the three, this medical condition accounts for more than 300,000 surgical interventions each year in the United States 4,5 at a cost of over $1 billion annually. 6,7 Despite the high prevalence of clinically observable POP, the condition is asymptomatic for many women. 8 Symptoms include predominantly a sensation of vaginal bulging, with associated symptoms such as vaginal pressure, vaginal dryness, pelvic pain, pain with intercourse, urinary retention, urinary incontinence, and/or constipation. 9 The severity and degree of discomfort and dysfunction caused by these symptoms can adversely affect women’s quality of life and are prime determinants in the course of treatment. 10
Risk factors for POP include age, parity, past vaginal delivery, and, in some studies, increased body mass index (BMI). 11 –16 Most prior studies have been cross-sectional and focused on women with surgically treated or clinically recognized POP. Limited information exists regarding the incidence of self-reported POP as women age or risk factors associated with the onset of new symptomatic POP from nonclinical samples of midlife women, aged 40–65. Identification of individuals at the risk of developing symptomatic POP in midlife would enhance clinical management and could potentially suggest prevention or early intervention strategies. Risk by race/ethnicity is unresolved in the current literature. 17
The multiracial/ethnic, community-based Study of Women’s Health Across the Nation (SWAN) followed midlife women, aged 42–52 at enrollment, for two decades over the menopausal transition. The objectives of this study were to document the incidence of self-reported, symptomatic prolapse in midlife women transitioning through the menopause and to assess the association of race/ethnicity with the incidence and timing of self-reported POP. We also evaluated the association between self-reported POP and subsequent hysterectomy.
Materials and Methods
Study population
SWAN is a longitudinal cohort study of the menopausal transition that commenced in 1996 and was conducted at seven geographical sites. The study design has been described elsewhere. 18 To be eligible for participation, women had to be 42–52 years old, have an intact uterus and at least one ovary, and in the previous three months must have had at least one menstrual period and not used exogenous reproductive hormones. Each site recruited White women and women from one additional racial/ethnic group as follows: African Americans in Pittsburgh, Boston, southeast Michigan, and Chicago; Japanese women in Los Angeles; Hispanic women in Newark, New Jersey; and Chinese women in Oakland, California. In total, 3,302 women were enrolled and followed up approximately annually.
Women were asked to report presence of symptoms suggesting POP beginning at the second follow-up visit (V2) in 1998/99 and then again at each of the 11 subsequent follow-up visits through 2012. Of the 3,302 women enrolled at baseline, 2,999 (90.8%) participated in at least one visit on or after V2 and were eligible for this analysis. We excluded 80 women who had had a hysterectomy after enrollment but prior to V2 or their first eligible visit if they did not complete the V2 visit, resulting in a final analytical sample of 2,919 women. At the 2012 follow-up interview, we remained in contact with 2,502 (78.1%) of surviving women.
Measures
At each study visit, women completed a set of self-administered and interviewer-administered questionnaires. In the self-administered questionnaire, symptomatic POP was ascertained by an affirmative response to a question, derived from the validated Pelvic Floor Distress Inventory. 19,20 Participants were asked, “Since your last study visit, have you had any of the following conditions?” with the list of gynecological conditions including “pelvic prolapse or relaxation (the uterus, bladder, or rectum drops, sometimes bulging out of vagina)? (yes/no).” According to the American Gynecological and Obstetrical Society, an affirmative response to the sensation and/or the observation of a vaginal bulge is consistent with the definition of symptomatic POP and the presence of a clinical POP. 19 –21 Information about surgeries since the last visit, including whether the participant had had a hysterectomy, was ascertained too.
Covariates assessed at the baseline interview included study site, self-reported race/ethnicity (African American, White, Hispanic, Chinese, or Japanese), educational level (high school or less, college, postsecondary), financial strain, and reproductive history. Financial strain was assessed by asking how difficult it was to pay for basic necessities (very, somewhat, or not at all). The reproductive history included questions about the number of pregnancies, live births, miscarriages, and abortions and, for live births, the delivery method (vaginal or cesarean section). Menopausal status was assessed at each study visit based on women’s self-reported menstrual characteristics. If they had had a menstrual period in the previous 3 months women were classified as premenopausal, if they reported no change in menstrual regularity, as perimenopausal if they reported decreased regularity in their menses in the past 12 months or if they had had no menses in the past 3–11 months and as postmenopausal if they had no menses for the past 12 or more months or if they had had a bilateral oophorectomy since their last study visit. Weight and height were measured at each visit, and BMI was calculated.
Statistical analysis
Means and standard deviations were calculated for continuous covariates, and frequencies were calculated for categorical covariates, both overall and for women who ever reported POP (yes/no). We used t-tests for continuous covariates and chi-square tests for categorical covariates to assess whether women differed significantly by whether or not they ever reported POP. We calculated the percentage of women reporting POP, as well as the percent reporting a hysterectomy both at V2 and at any visit during the study period. We estimated survival curves of POP by age for the total population and by race/ethnicity, using interval-censored Kaplan–Meier plots.
We estimated the hazard ratio (HR) and 95% confidence interval (CI) for incident POP using interval-censored Cox proportional hazards models, which enabled us to incorporate data on prevalent cases at V2 in the analysis and to account for the lack of precise information on the date of onset. Women were right-censored at age at the final visit. Assuming that women were very unlikely to experience POP prior to age 20, all women who reported POP at V2 were left-censored at age 20. Unadjusted associations were examined between POP and each covariate. We assessed parity both as a continuous variable and as parous versus nulliparous and also assessed the mode of delivery considering both only cesarean and ever vaginal delivery. The final Cox model was adjusted for all covariates except for BMI and menopausal status, which were not associated with POP, and parity. Vaginal delivery was selected for the final model instead of parity as the risk of POP did not increase beyond the first birth, the effect size for having a vaginal birth only versus a vaginal birth and a cesarean section did not differ, and the effect size for having only had a cesarean section was small and not significantly associated with the risk of POP after adjustment. We conducted sensitivity analyses excluding women who reported POP at V2 and also limiting the analyses to the four sites that enrolled Black and White women to assess geographic differences in POP reporting.
The prospective data enabled us to examine the association between self-reported POP and subsequent hysterectomy. We estimated the unadjusted and adjusted HRs and 95% CIs for incident hysterectomy using a time-dependent Cox proportional hazards model and adjusting for race/ethnicity and study site. POP was modeled as a time-varying variable. Statistical significance was defined at α < 0.05. Analyses were performed using RStudio version 1.1.456 (R Foundation for Statistical Computing) and SAS version 9.4 (SAS Institute).
Results
The 2,919 participants in this analysis included White (48.0%), Black (27.9%), Japanese (9.2%), Chinese (8.3%), and Hispanic women (6.7%) (Table 1). Their average age at V2 was 48.45 (±2.69 standard deviation) years. The overall median year of follow-up was 13.3 years and was 13.2, 13.4, 13.5, 12.9, and 13.3 for Black, White, Chinese, Hispanic, and Japanese women, respectively.
Population Characteristics at Baseline and Percent Ever Reporting Pelvic Organ Prolapse over a 15-Year Period: The Study of Women’s Health Across the Nation
p-Value compares those who ever report POP versus those who never report POP.
POP, pelvic organ prolapse.
Over the course of the study, 241 women ever reported symptoms of POP. At V2, 2.74% of women reported POP. By the 13th follow-up visit, an additional 5.52% of women had reported POP, resulting in 8.26% of women ever reporting POP. The proportion of women who ever self-reported POP in this study was highest among Hispanic women (22.1%), lower among White (8.2%) and Black (7.7%) women, and lowest among Japanese and Chinese women (4.1% and 3.7%, respectively). A higher proportion of women with less education (9.0–9.1%) and women with difficulty paying for basics (10.1–13.8%) ever reported having POP as compared with women with more than a college education (5.2%) and women without financial strain (6.6%). A higher proportion of parous women (9.4%) and women who had had any vaginal delivery (10.3%) ever reported POP compared with nulliparous women (2.4%). The proportion of women ever reporting POP did not differ significantly by number of births, BMI, or menopausal status.
Kaplan–Meier survival curves for POP are presented in Figure 1. When we estimated cumulative probability of reported POP as women aged, we observed an approximately linear increase in prevalence from 2.1% at age 45 to 10.1% by age 65, with the probability of POP increasing by an average of approximately 4.0% each decade after age 45.
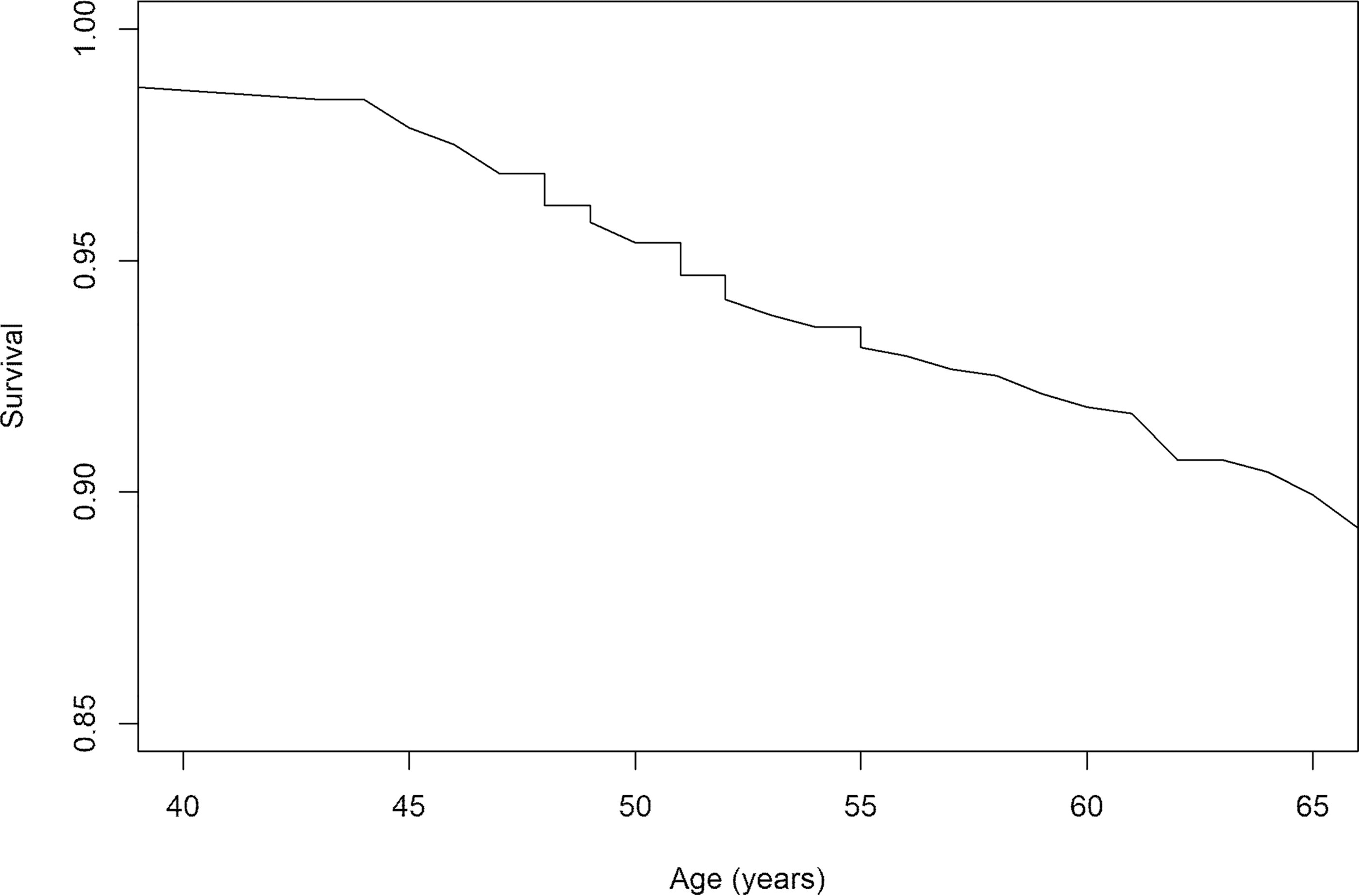
Interval-censored Kaplan–Meier survival curves for not reporting pelvic organ prolapse: The Study of Women’s Health Across the Nation (n = 2,919).
The Kaplan–Meier survival curves for POP are presented by race/ethnicity in Figure 2. Chinese and Japanese women have the flattest curves with an estimated probability of POP by age 65 of 4.8% and 4.2% of women, respectively. Both Black women and White women had a somewhat steeper curve with an estimated probability of POP of 8.9% and 9.7% by age 65, respectively. Hispanic women had the steepest curve, with an estimated probability of POP of 12.1% by age 50 and 33.9% by age 65.

Interval-censored Kaplan–Meier survival curves for not reporting pelvic organ prolapse by race/ethnicity: The Study of Women’s Health Across the Nation (n = 2,919).
Table 2 presents the unadjusted and adjusted HRs for POP over the 15 years of follow-up from V2 to V13. The unadjusted hazard of POP did not differ between White and Black participants. Hispanic women had a significant 3.1-fold increase in the unadjusted hazard compared with White women, whereas Chinese and Japanese had significantly lower unadjusted relative hazards that were less than half that of White women, 0.43 and 0.48, respectively.
Unadjusted and Adjusted Hazard Ratios of Pelvic Organ Prolapse by Sociodemographic and Reproductive History in the Study of Women’s Health Across the Nation
Model includes race/ethnicity, education, financial strain, and ever vaginal delivery.
Women with more than a college education had an unadjusted relative hazard that was approximately half that of women with less education (HR = 0.55). Women who had a somewhat or very hard time paying for basics had a significant 1.6-fold and 2.4-fold increase, respectively, in the hazard of POP compared with women who had no difficulty. Having given birth, specifically a vaginal birth, was strongly associated with the hazard of POP with a 4-fold increase in the hazard for parous women compared with nulliparous women and a 3.4-fold increase for women who reported ever having had a vaginal birth versus women who never had a vaginal birth. Menopausal status at follow-up V2 was not associated with POP.
After adjustment for race and ethnicity, education, financial strain, and ever vaginal delivery, the direction of effects for race/ethnicity and other covariates remained similar. The relative hazard of POP for Hispanic women remained double, whereas the hazards for Chinese and Japanese remained less than half that of White women. The hazard for Black women declined to 0.74, but the CI still included 1. The adjusted relative hazards for POP among women reporting substantial economic hardship at baseline and for women with prior vaginal deliveries were slightly attenuated but remained significant. When analyses were limited to White women, site was not associated with POP. In sensitivity analyses excluding reported POP at V2, results were essentially unchanged.
Across the study period, 7.91% of women reported having a hysterectomy. Of note, women reporting POP were more likely to report having a subsequent hysterectomy than were those without POP (adjusted HR = 3.47, 95% CI [2.42, 4.96] after adjustment for site and race/ethnicity).
Discussion
This study is among the first community-based prospective studies to describe a linear increase in reported POP as women age through the midlife from their early 40s through their mid-60s. In this multiracial/ethnic population of midlife women, the estimated probability of reporting POP was already notable by age 45 with 2.1% of women reporting POP. With an incidence of 4.0% in each subsequent decade, POP was reported by 10% of women by age 65. The probability of POP differed by race/ethnicity. Hispanic women had approximately a twofold higher risk of reporting POP, whereas Chinese and Japanese women had less than half the risk of White women, such that by age 65, the estimated probability of a symptomatic POP for Hispanic women was 1 in 3 women, compared with about 1 in 10 for White women and about 1 in 20 for Chinese and Japanese women. Risks for Black women differed little from that of White women. These race and ethnic differences persisted after the adjustment for population differences in socioeconomic status and reproductive history. As noted in other studies, POP was strongly associated with vaginal birth and was more frequent among women of lower socioeconomic status as assessed by education and financial strain. 22,23 Presence of POP increased women’s risk of having a hysterectomy. Others have also reported that the risk of POP increases following hysterectomy; 24 however, women with prior hysterectomy were not eligible for enrollment in SWAN, limiting our ability to further examine this issue.
In this community-based sample, we found that incidence of self-reported POP increased across the midlife as women aged from 45 to 65 years. Evidence for the impact of age on POP prevalence is somewhat inconsistent with cross-sectional studies, with small numbers of cases, reporting little change with age, whereas prospective studies observe increasing risk with age. In a cross-sectional analysis of the National Health and Nutrition Examination Survey’s data, the prevalence doubled from 1.6% to 3.8% after age 40 changing little thereafter, but only 58 cases were ascertained. 25 The Kaiser Reproductive Risks for Incontinence study also reported little difference in prevalence with age, 5% of women aged 40–49 and 6% in women aged 50–69. However, in a secondary analysis of the WHI among women aged 50–79 years, the five-year incidence of POP based on clinical examination was 16.2% in White, 9.4% in Black, and 20.1% in Hispanic participants. 26 In a large nationally representative sample of Norwegian women aged 30 years and older, the Nord-Trøndelag Health Study reported that POP surgery increased from 0.7% in women under age 40 to 3.1% in women aged 40–59 years and to 10.8% in women aged 60 years and older with a cumulative incidence of 14.6% by age 85. 15
Some authors suggest that an increase in risk for POP as women transition through the menopause could be in part the product of hormonal changes arising during and after menopause, when a decrease in the tissue perfusion of estrogen erodes the elasticity of pelvic ligamentous architecture. 27,28 Few studies have specifically considered the effect of menopause; however, Sze and Hobbs reported that menopause was associated with an increased probability of prolapse beyond the hymen. 27 An analysis of national U.S. hospital discharge rates documented that the annual surgery rates for prolapse increased across the stages of reproductive aging from 7/10,000 in reproductive-age women to 24/10,000 in perimenopausal and 31/10,000 postmenopausal women and then declined to 17/10,000 in elderly women. 29 Neither of these studies adjusted for age. However, consistent with our findings, a recent systematic review and meta-analysis confirmed increasing age but not menopausal status as a risk factor for POP. 30 The mechanisms by which POP develops over time are multiple, but aging is an important factor. 31 Birth-related muscle tear and consequent loss of pelvic floor muscle attachment, along with wear and tear over time on the ligamentous architecture, are additional contributing mechanisms. Ultimately, the occurrence of POP relates to wear and tear of birth, time, and aging. 10,28,32 If further follow-up confirms a leveling off of risk after age 60, it would be consistent with the WHI studies that have found that POP may anatomically regress leading to a decrease of self-reported POP over time, 2,3,26 although the lower prevalence in older women may also reflect prior surgical intervention. 15,29
Another key observation of this study was the difference in risk by race/ethnicity as women aged. Consistent with other studies, we found that self-reported POP increased rapidly with age among Hispanic women when compared with all other ethnic groups, 1,12,13 which could be related to higher levels of symptoms reported among Hispanic women. 33,34 Chinese and Japanese women had much lower risk, with just 1 in 20 women reporting POP by age 65, consistent with some studies showing lower risks of POP in Asian women. 35,36 In contrast to most but not all previous studies, 36 we observed little difference in risk between White and Black women. Prior studies have reported a higher prevalence in White women compared with Black women; 12,25,37 however, these studies had relatively small numbers of Black women. Not only did our analysis of SWAN data had a larger sample size, but this sample also followed premenopausal women through menopause. Future studies should assess protective factors associated with Asian/Japanese ethnicity and assess whether race/ethnicity associations differ by age. The observed differences by race/ethnicity were not explained by differences in parity and the probability of vaginal birth or by socioeconomic status and financial strain, but our measures do not fully account for differences in life contexts. For example, the SWAN Hispanic population is derived from an inner-city population with limited resources who were more likely than other SWAN participants to have had jobs involving heavy lifting. Lifting elicits high intra-abdominal pressure, another risk factor for POP due to pronounced downward pressure on the pelvic organs. 15,23 Post-college education and economic well-being were both negatively associated with the occurrence of POP. Post-college education is associated with a higher age at first birth, advanced maternal age and low birth weight, and nulliparity or lower parity. 38 –40 All these factors may delay or reduce strains to the pelvic floor and, by extension, delay or reduce POP occurrence in this particular group.
POP symptoms vary in severity and frequency depending on the degree of the anatomical defect. 41 In the United States, among women seeking medical attention to address these symptoms, hysterectomy is performed as a last recourse. However, Hispanic women have voiced concerns that POP may be related to cancer and tend to prefer aggressive surgical treatments including hysterectomy when available, 42 which might partially explain a threefold increase in the risk of hysterectomy observed following the self-report of POP. However, a recent meta-analysis provides evidence that uterine-sparing prolapse repair does not increase the risk of POP recurrence in the short term. 43
Consistent with one recent systematic review and meta-analysis, 44 BMI was not associated with risk of prolapse in this study, although another systematic review and meta-analysis reported an increased risk with overweight and obesity. 45 In SWAN, 58% of women were overweight/obese at follow-up V2, and, although BMI increased as participants aged through the midlife, 46 our modeling approach did not permit time-varying covariates, potentially limiting our ability to evaluate risks associated with BMI in this cohort.
Limitations of this study include the fact that POP was self-reported and that women did not undergo a clinical examination to confirm diagnosis, nor the size of the POP was documented. Thus, the study includes only self-reported POP and may underestimate the true prevalence and incidence of the condition. The single-item question used to identify POP has been shown to be a valid and reliable measure of the presence of prolapse. 20,21 However, although specificity of this question is high, sensitivity declines with population prevalence. Thus, age-related incidence of prolapse is likely underestimated in this study. In addition, knowledge and awareness of the condition may vary by race/ethnicity. Self-report may reflect that women have been told they have a prolapse during a pelvic exam for an unrelated matter, that they have self-identified an asymptomatic anatomical defect, or that they have experienced a bothersome symptom or increase in symptom severity that led to the discovery of a prolapse. Left truncation of women with POP may have occurred, as women who had had a hysterectomy were not eligible for inclusion in SWAN, and African American women were more likely to be excluded than other race/ethnicities because of their higher prevalence of hysterectomy. Finally, the sample size of some race/ethnic groups was small with few POP cases reported by Japanese and Chinese women.
This study also has several strengths. It is one of the first prospective, population-based studies to estimate the incidence of symptomatic POP as women aged through the midlife and menopause. With 15 years of follow-up in a nonclinical, multiracial/ethnic population, it has documented that the midlife is a period of increased risk for self-reported POP. Future studies should evaluate whether this observed increase in self-reported POP is related to development or progression of clinically confirmed POP.
Conclusions
The prevalence of self-reported POP increases markedly in the midlife as women age from their mid-40s to their mid-60s, coincident but not associated with menopause. The proportion of women reporting POP varied by race/ethnicity that was not accounted for by population differences in socioeconomic life contexts and the probability of having had a vaginal birth. The highest risk was observed among Hispanic women and the lowest risk among Japanese and Chinese women. Despite discrepancies in the literature, gyneco-obstetrical history, socioeconomic status, health literacy, language barriers, and access to health care likely play an important role in race and ethnic disparities in presentation and care for POP. Nevertheless, increased focus on POP in midlife women may help identify the relative roles of these various physiological and sociological factors occurring as women age and their relative impact on the development of and women’s awareness of POP. Further investigation of factors associated with the reduced prolapse incidence among Chinese and Japanese women with a larger sample size is warranted as are studies of the impact of clinical evaluation and intervention during midlife on women’s quality of life.
Although not associated with menopausal status, health care providers should incorporate screening for and information about POP when treating menopausal symptoms and addressing health needs of midlife women given the low health care utilization rate for prolapse especially among Black and Hispanic women. Particular attention should be given to ensuring services for women of limited economic resources, especially those with a history of vaginal birth, as these women may be at an increased risk of POP and are more likely to have greater challenges in accessing care and limited awareness of treatment options. Research on pathophysiological factors associated with POP and potential increases in symptoms, dysfunction, or bother as women age through the midlife is warranted.
Footnotes
Acknowledgments
Clinical Centers: University of Michigan, Ann Arbor, MI—Carrie Karvonen-Gutierrez, Principal Investigator (PI) 2021 – present, Siobán Harlow, PI 2011–2021, MaryFran Sowers, PI 1994–2011; Massachusetts General Hospital, Boston, MA—Sherri‐Ann Burnett‐Bowie, PI 2020 – Present, Joel Finkelstein, PI 1999–2020, Robert Neer, PI 1994–1999; Rush University, Rush University Medical Center, Chicago, IL—Imke Janssen, PI 2020 – Present, Howard Kravitz, PI 2009–2020, Lynda Powell, PI 1994–2009; University of California, Davis/Kaiser—Elaine Waetjen and Monique Hedderson, PIs 2020 – Present, Ellen Gold, PI 1994 – 2020; University of California, Los Angeles—Arun Karlamangla, PI 2020 – Present, Gail Greendale, PI 1994 – 2020; Albert Einstein College of Medicine, Bronx, NY—Carol Derby, PI 2011 – present, Rachel Wildman, PI 2010–2011, Nanette Santoro, PI 2004–2010; University of Medicine and Dentistry—New Jersey Medical School, Newark—Gerson Weiss, PI 1994–2004; and the University of Pittsburgh, Pittsburgh, PA—Rebecca Thurston, PI 2020 – Present, Karen Matthews, PI 1994–2020. NIH Program Office: National Institute on Aging, Bethesda, MD—Rosaly Correa-de-Araujo 2020 - present, Chhanda Dutta 2016–present, Winifred Rossi 2012–2016, Sherry Sherman 1994–2012, Marcia Ory 1994–2001; and National Institute of Nursing Research, Bethesda, MD—Program Officers. Central Laboratory: University of Michigan, Ann Arbor, MI—Daniel McConnell (Central Ligand Assay Satellite Services). Coordinating Center: University of Pittsburgh, Pittsburgh, PA—Maria Mori Brooks, PI 2012–present, Kim Sutton-Tyrrell, PI 2001–2012; and New England Research Institutes, Watertown, MA-Sonja McKinlay, PI 1995–2001. Steering Committee: Susan Johnson, current chair, Chris Gallagher, former chair. We thank the study staff at each site and all the women who participated in SWAN.
Authors’ Contributions
S.D.H. and J.M.M. contributed to the conception, planning, carrying out, analyzing, and writing up of the study. A.M., M.M.H., B.R., and S.A.D. contributed to analyzing and writing up of the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
SWAN has grant support from the National Institutes of Health (NIH), Department of Health and Human Services, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR), and the NIH Office of Research on Women’s Health (ORWH) (Grants U01NR004061; U01AG012505, U01AG012535, U01AG012531, U01AG012539, U01AG012546, U01AG012553, U01AG012554, U01AG012495, and U19AG063720). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH, or the NIH. S.D.H. gratefully acknowledge use of the services and facilities of the Population Studies Center at the University of Michigan, funded by NICHD Center Grant R24 HD041028.
ETHICS APPROVAL
Procedures of this study received ethical approval from each clinical site. Northern California—Institutional Review Board Administration, University of California at Davis (March 19, 2020) 260339-8 and Institutional Review Board for the Protection of Human Subjects, Kaiser Foundation Research Institute (March 10, 2020) CN-94BSter-01-H. Los Angeles—Office of Human Research Protection, University of California at Los Angeles (February 26, 2020) IRB#11–002274. Southeastern Michigan—The Health Sciences and Behavioral Sciences Institutional Review Boards, University of Michigan (IRB-HSBS) (October 29, 2019) HUM 00083308. Boston—Partners Human Research Committee (PHRC), Partners HealthCare System (July 15, 2019) 1999P006353. Newark—Office of Human Research Affairs (OHRA), Albert Einstein College of Medicine (May 18, 2020) 2005-012. Pittsburgh—Human Research Protection Office (HRPO), University of Pittsburgh (December 12, 2019) IRB 0402168 (Clinical Center) and CR19030365-002 (Coordinating Center). Chicago—Institutional Review Boards, Rush University Medical Center (July 5, 2020) 13021201-IRB01-CR06.