
Abstract
Background:
Atherosclerotic cardiovascular disease (ASCVD) remains the most common cause of death in women. Pregnancy is an exposure unique to women leading to significant changes in maternal cardiovascular function. However, studies of the relationship between the number of pregnancies and ASCVD are rare. We aimed to clarify the association between the number of pregnancies and ASCVD.
Methods:
In this cross-sectional study, we used publicly available data from the National Health and Nutrition Examination Survey from 1999 to 2018. The number of pregnancies was divided into 0 (reference), 1, 2–3, 4–5, or ≥6, to create more stable estimates. A multiple logistic regression approach was used to examine the correlation between pregnancy and ASCVD in women aged 45 years or older who reported no menstruation in the past 12 months due to menopause, as well as in those aged 55 years or older, encompassing various age groups. We also separately estimated the association between the exposure of pregnancy and individual components of ASCVD.
Results:
In this study, age-adjusted data showed that women with six or more pregnancies had a doubled risk (odds ratio [OR]: 2.07) of ASCVD. The risk remained elevated at 1.69 times in women with four to five pregnancies and further increased to 1.90 times in women with six or more pregnancies, after adjusting for social factors. Similar patterns were observed when considering reproductive health and cardiovascular risk factors. Across the full population, every model that accounted for these variables consistently indicated that with an increasing number of pregnancies, we observed higher ORs for ASCVD risk (all p values <0.05).
Conclusions:
A higher number of pregnancies was associated with a higher risk of ASCVD after menopause, especially among women aged 45–64 years. Moreover, this association is particularly significant in the risk of stroke, cardiovascular heart disease, and heart attack.
Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality worldwide, 1,2 with an estimated 422.7 million CVD cases and 17.92 million CVD deaths in 2015. Atherosclerotic cardiovascular disease (ASCVD), which mainly includes coronary heart disease (CHD) and stroke, 3 is the leading cause of CVD health loss in the United States and industrialized countries. 4 –6
Although CVD has been considered a male disease for decades, it is more common in women. Among the European population, 43% of women die from CVD compared with 39% of men, 7 and in the United States, nearly 48 million women are affected by ASCVD. 8 Much of the burden of ASCVD can be explained by a range of traditional risk factors affecting both men and women, including elevated blood pressure, smoking, overweight and obesity, diabetes mellitus (DM), and elevated cholesterol. 9 However, the high mortality rate of ASCVD in women compared with men has raised interest among women’s cardiovascular health workers, 10 where some researchers have focused on the impact of gender on ASCVD. 11,12 Recent studies have found evidence for specific female ASCVD risk factors such as medical conditions during pregnancy, such as gestational hypertension and diabetes. 13 However, more studies are still needed to explore the specific cardiovascular risk factors for women compared to those of men.
Pregnancy is a cardiometabolic stressor that may expose potential vascular and metabolic abnormalities. One study found that a higher number of pregnancies was an independent risk factor for gestational diabetes. 14 A systematic review suggested that an increasing number of pregnancies were associated with an increased risk of atrial fibrillation in a dose–response relationship. 15 However, previous studies looking at the relationship between number of pregnancies and CVD were inconsistent. 16,17 It is necessary, therefore, to use a national cohort to investigate the association between the number of pregnancies and the risk of ASCVD.
Therefore, we explored the relationship between the number of previous pregnancies and ASCVD in menopausal women and used data from the 2011–2018 National Health and Nutrition Examination Survey (NHANES). From this, we hope to contribute to further research on the pathogenesis of CVD in women and help control cardiovascular risk in the future.
Methods
Data source and participants
In this cross-sectional study, we used publicly available data from the NHANES from 1999 to 2018. NHANES is a nationally representative health survey designed and administered by the National Center for Health Statistics (NCHS) at the Centers for Disease Control and Prevention and was approved by the NCHS Research Ethics Review Board (Protocol #98e12; available on the web at NHANES-National Health and Nutrition Examination Survey Homepage [cdc.gov]).
We conducted a retrospective analysis of a cohort of the population using NHANES in the United States from 1999 to 2018. Written informed consent was obtained from each NHANES participant. The menopausal status was determined based on responses to a reproductive health survey questionnaire. Specifically, women were asked: “Have you had at least one menstrual period in the past 12 months? (Please do not include bleedings caused by medical conditions, hormone therapy, or surgeries).” Subjects who answered “no” to the first question were subsequently asked, “What is the reason that you have not had a period in the past 12 months? (Options: pregnancy; breastfeeding; hysterectomy; menopause/change of life; other).” Accordingly, women aged 45 years or older who had not experienced menstruation in the preceding 12 months, attributing this absence to menopause, as well as those aged 55 years or older, were classified as postmenopausal. 18
As shown in Figure 1, this study included 11,936 women aged ≥ 45 years after menopause during the NHANES 1999–2018 survey cycle. Of these participants, 5,878 were excluded based on the following: (1) 4,151 participants had hysterectomies and (2) 1,727 participants lacked data on their number of pregnancies. Thus, 6,058 participants were finally included in the present study.
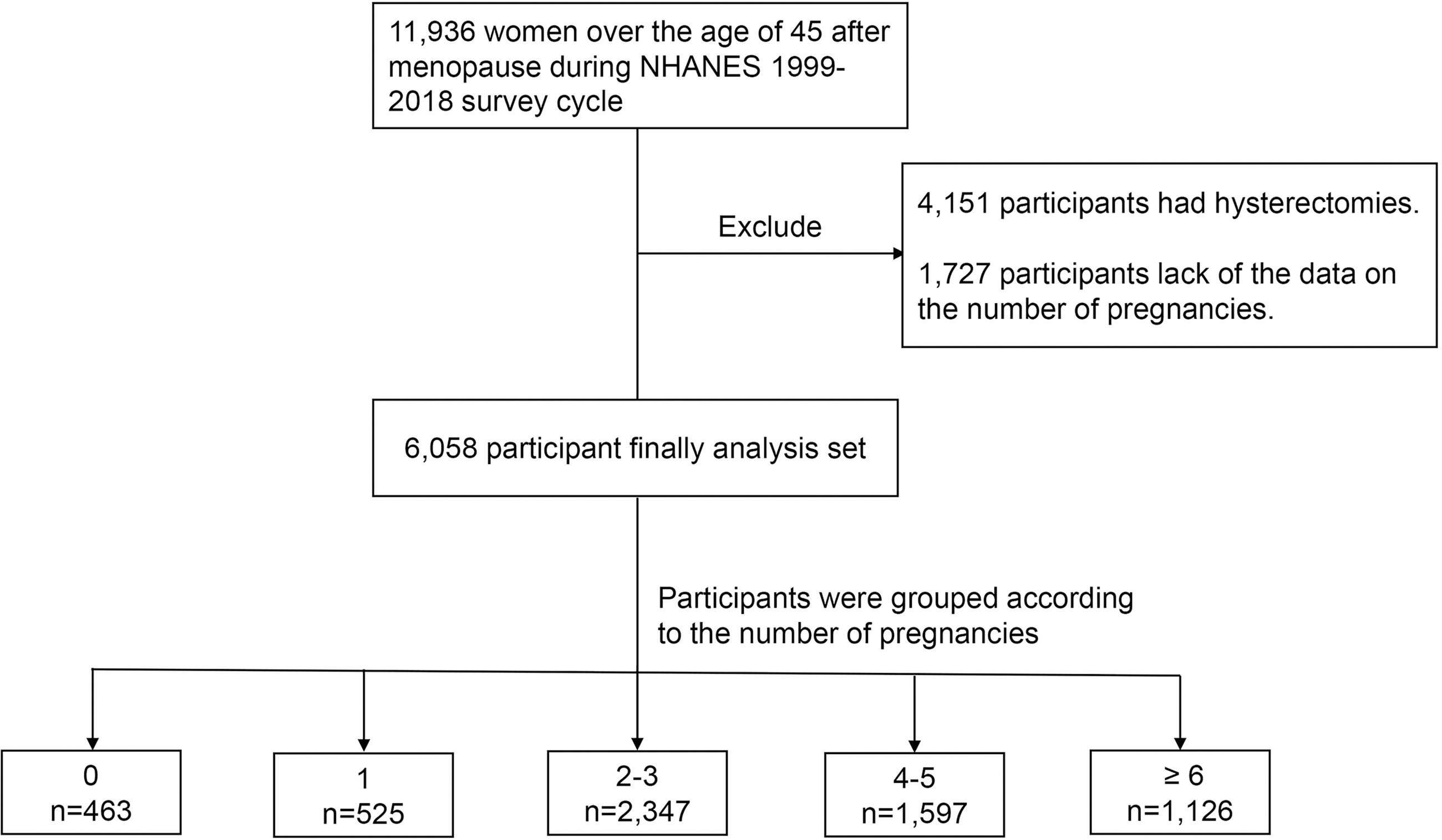
Flowchart of the participants included. NHANES, National Health and Nutrition Examination Survey.
Exposure variables: Number of pregnancies
The number of pregnancies was assessed via self-report using a standardized questionnaire completed at the baseline examination. For the purposes of the presentation, the number of pregnancies was divided into 0 (reference), 1, 2–3, 4–5, or ≥6, to create more stable estimates.
Assessment of ASCVD and 10-year ASCVD risk
“Has a doctor or other health professional ever told (you/survey participant) that (you/s/he) … had a coronary heart disease/angina, also called angina pectoris/heart attack (also called myocardial infarction)/stroke?” was a question on the medical conditions section of the household questionnaires via home interview, and those who answered “yes” were deemed to have a history of ASCVD. Ten-year ASCVD risk scores were calculated according to previously published guidelines. 19 Predicted ASCVD risk higher than 7.5% was defined as a high 10-year ASCVD risk.
Definitions of covariates of interest
We used covariates assessed from the baseline examination. Participants answered questionnaires that provided information on age, race, education level, poverty ratio, marital status, smoking status, alcohol use, age at menarche, age at menopause, oral contraceptive use, exogenous hormone, DM, and hypertension. The body mass index (BMI) (kg/m2) was obtained from the exam file. NHANES data collection and detailed data collection methods are available at the NHANES website (http://wwwn.cdc.gov/nchs/nhanes).
Statistical analyses
We used the NHANES recommended weights to account for the planned oversampling of specific groups. The continuous variables were expressed as the mean ± SE, and the categorical variables were presented as counts (percentages). Baseline characteristics between each group were compared using a t-test for continuous variables and an χ2 test for categorical variables.
This study used multiple logistic regression to examine the link between pregnancy and ASCVD across various models. Model 1 adjusted for age, Model 2 for social factors including age, race, education, poverty ratio, smoking, drinking, and marital status. Model 3 considered reproductive health factors such as oral contraceptive use, age at menarche, menopause, and hormone use (former). Model 4 incorporated cardiovascular risk factors, including BMI, hypertension, and diabetes, alongside the previously mentioned variables. The odds ratio (OR) and 95% confidence intervals (CI) were calculated for each model. The analysis differentiated between age groups (45–64 and ≥65 years) and assessed the association between pregnancy and individual components of ASCVD. Moreover, we performed sensitivity analyses, and multiple logistic regression was used to assess the association between pregnancy and 10-year ASCVD risk according to the baseline number of pregnancies categories.
All data analyses were performed using R software (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria). A two-sided p value < 0.05 indicated significance for all analyses.
Results
This study involved 6,058 women aged ≥ 45 years, including 463 women with 0 pregnancies, 525 with one pregnancy, 2,347 with—two to three pregnancies, 1,597 with—four to five pregnancies, and 1,126 with six or more pregnancies. There were differences in the average age of the groups (p < 0.001), women with six or more pregnancies had the highest mean age (68.8 years), and women with one pregnancy had the lowest mean age (63.8 years). The higher the number of pregnancies, the lower the percentage of women with higher education (p < 0.001) and the lower the percentage of non-Hispanic Whites (p < 0.001). No statistical differences were found between the group’s BMI and age at menopause, but differences were found in alcohol use (p < 0.001) and age at menarche (p = 0.018). In addition, there were significant differences in exogenous hormone use (former), oral contraceptive use (former), and the prevalence of hypertension and DM in each group (Table 1).
Baseline Characteristics of Participants According to the Number of Pregnancies, NHANES 1999–2018
BMI, body mass index; DM, diabetes mellitus; NHANES, National Health and Nutrition Examination Survey.
Participants were asked whether they were married, widowed, divorced, separated, never married, or living with a partner. Those reporting marriage or living with a partner were grouped together.
The incidence of postmenopausal ASCVD increased significantly with the number of pregnancies (Fig. 2). In this study, four logistic regression models were used to analyze the link between the number of pregnancies and the risk of ASCVD. Model 1 indicated that women with six or more pregnancies had a twofold increased risk of ASCVD (OR: 2.07, 95% CI: 1.31,3.25). Model 2 showed that women with—four to five pregnancies had a 1.69 times higher risk, and those with six or more pregnancies had a 1.90 (95% CI: 1.15,3.15) times higher risk of ASCVD compared with women with no pregnancies. Models 3 and 4 further confirmed these findings, demonstrating increased risks of ASCVD in women with—four to five and six or more pregnancies (Table 2). In the whole population, all adjusted models found an increasing trend in the OR of ASCVD risk as the number of pregnancies increased (p for trend < 0.001, = 0.010, < 0.001, = 0.010 in Models 1, 2, 3, and 4, respectively).

Association of the number of pregnancies with ASCVD. ASCVD, atherosclerotic cardiovascular disease; CHD, coronary heart disease.
Odds Ratios for the Association Between Pregnancy and ASCVD According to Baseline Number of Pregnancies
Reference refers to the baseline group of women who have not experienced any pregnancies (No. of pregnancies = 0).
Model 1: adjusted for age.
Model 2: adjusted for age, race, education level, poverty ratio, smoking use, drinking status, and marital status.
Model 3: adjusted for age, race, oral contraceptive use, age at menarche, age at menopause, and exogenous hormones (former use).
Model 4: adjusted for age, race, BMI, education level, smoking use, drinking status, exogenous hormones, hypertension, and DM.
BMI, body mass index; DM, diabetes mellitus.
In this study, the association between pregnancy count and ASCVD risk was analyzed, specifically focusing on age groups. Among women aged 45–64 years, the risk of ASCVD in those with six or more pregnancies was notably higher compared to women with no pregnancies, with an OR of 3.76 (95% CI: 1.62,8.71) in Model 1 and 2.81 (95% CI: 1.13, 7.00) in Model 3. This group showed a significant increase in ASCVD risk correlating with the number of pregnancies (p for trend < 0.001, = 0.040, = 0.004, = 0.020 in Models 1, 2, 3, and 4, respectively). However, in women aged 65 years and above, an increased number of pregnancies did not correspond to a higher risk of ASCVD (p for trend = 0.100, = 0.110, = 0.060, = 0.100 in Models 1, 2, 3, and 4, respectively).
In addition, we did a sensitivity analysis, women with six or more pregnancies had a significantly increased 10-year risk of ASCVD, with ORs of 2.30 (95% CI: 1.38, 3.85), 1.91 (95% CI: 1.09, 3.85), 2.29 (95% CI: 1.35, 3.87) and 1.80 (95% CI: 1.11, 2.94) in the four models, respectively. Moreover, there was an upward trend in the 10-year risk of ASCVD as the number of pregnancies increased (all p for trend < 0.001; Table 3).
Odds Ratio for the Association between Pregnancy and 10-Year ASCVD Risk a According to Baseline Number of Pregnancies
Reference refers to the baseline group of women who have not experienced any pregnancies (No. of pregnancies = 0).
Model 1: unadjusted.
Model 2: adjusted for education level, poverty ratio, smoking use, drinking status, and marital status.
Model 3: adjusted for oral contraceptive use, age at menarche, age at menopause, and exogenous hormones (former use).
Model 4: adjusted for BMI, education level, smoking use, drinking status, exogenous hormones, hypertension, and DM.
ASCVD, atherosclerotic cardiovascular disease; DM, diabetes mellitus.
2,049 participants (had the data on 10-year ASCVD risk) were included.
Our study conducted a detailed examination of ASCVD, dividing it into four subcategories: CHD, stroke, angina, and heart attack. This analysis showed a significant increasing trend in the risk of stroke, CHD, and heart attack correlating with a higher number of pregnancies. However, this trend was not consistently observed in the cases of angina (Fig. 3).

The forest plot of the number of pregnancies with specific disease subgroups. Model 1: adjusted for age. Model 2: adjusted for age, race, education level, poverty ratio, smoking use, drinking status, and marital status. Model 3: adjusted for age, race, oral contraceptive use, age at menarche, age at menopause, and exogenous hormones. Model 4: adjusted for age, race, BMI, education level, smoking use, drinking status, exogenous hormones, hypertension, and DM. BMI, body mass index; DM, diabetes mellitus.
Discussion
In this study, we found that, compared with women who had never been pregnant, those postmenopausal women with the higher number of pregnancies had an increased risk of ASCVD, which was more pronounced in women aged 45–64 years. Furthermore, we found that postmenopausal women with a higher number of pregnancies also had an increased (10 years) ASCVD risk. In our subgroup analysis, we found that the increased risk was from stroke, CHD, and heart attack.
ASCVD, including cerebrovascular disease and atherosclerotic heart disease, remains the most common cause of death in women. Pregnancy is an exposure unique to women that leads to significant changes in maternal cardiovascular function, metabolism, and lifestyle. Previously, adverse pregnancy outcomes (such as pre-eclampsia or preterm birth) and pregnancy conditions (such as gestational hypertension and DM) have been shown to correlate with a higher risk for future ASCVD. 13,20 However, studies on the relationship between the number of pregnancies and ASCVD are scarce and some have inconsistent results. The earliest study showed no association between the number of births and CHD among parous women. 21 Although two subsequent studies reported that the rates of CDH were higher among multigravida women than among women who had never been pregnant, the degree of this association was slight. 22 In contrast, other studies have shown evidence that the number of deliveries was associated with CVD/ASCVD in a J-shaped manner. 23,24 These discrepancies may be due to several factors, including sociocultural differences in the populations studied, inconsistent exclusion criteria, and the evaluation of different multiple cardiovascular outcomes. These previous studies also had limitations, which included a small sample size, or lack of detailed patient information. In addition, these studies only investigated the relationship between the number of live births and CVD, whereas miscarriages and stillbirths, which are also accompanied by physiological changes due to pregnancy, were not considered. 25 Therefore, it remains controversial on the role of parity in the development of ASCVD given the inconsistency of previous findings. To clarify the relation between the number of pregnancies and ASCVD, we conducted a national study that was based on a large sample of women and was fully adjusted for possible confounding factors (including race and education level) to further quantify the association between parity and the risk of ASCVD. Finally, we confirmed that postmenopausal women with a higher number of pregnancies had an increased risk of ASCVD compared to women who had never been pregnant.
The potential mechanisms underlying the association between the number of pregnancies and ASCVD are not known. During pregnancy, the cardiovascular system undergoes significant and lasting changes, and due to a total increase in blood volume of about 45% during pregnancy 26 –28 total peripheral vascular resistance gradually decreases in parallel, 25,29,30 cardiac output continues to increase, peaking at 30–40% higher than nonpregnant levels in singleton pregnancies, leading to reversible or irreversible changes in heart anatomy. 31 –33 In addition, weight gain, abdominal fat accumulation, elevated blood lipid levels, increased insulin resistance, additional stressors (such as endothelial dysfunction, and inflammation), and hemostatic processes often occur inevitably in pregnant women. 34 –37 The above-mentioned physiological and metabolic changes in the cardiovascular system not only increase the risk of cardiovascular disease during pregnancy, 38 but also increase the risks of CVD in women in the long term. 39 We can reasonably speculate that repeated exposure to these changes may have long-term and cumulative effects on cardiovascular health. In our study, higher postmenopausal triglycerides and the higher prevalence of hypertension and diabetes in women with more pregnancies seemed to validate this mechanism.
In the present study, we first found that the association between the number of pregnancies and ASCVD was more significant in postmenopausal women aged 45–64 years using an age-stratified analysis. In contrast, this relationship was not significant in women ≥65. The reasons for this are unknown and are probably complex. Women aged 45–64 years will go through menopause, and it has been reported that nulligravida women may be less likely to experience negative symptoms, meaning a better physiological/metabolic condition and less stress. 40 The possible psychological and physiologic mechanisms related to these findings are intriguing and deserve further study. However, certainly, the inclusion of the number of pregnancies for cardiovascular risk assessment is very necessary for women in this age group. Furthermore, we found a particularly significant positive association between the number of pregnancies and stroke. This is consistent with previous studies. For example, an analysis of women aged 45–74 years showed that women with six or more pregnancies had a 70% increased risk of stroke when compared with women who had never been pregnant. 41 A recent study found that higher numbers of pregnancies and births were associated with subclinical atherosclerosis of the brain and carotid arteries (white matter hyperintensity and carotid artery plaque), 42 which are strong predictors of stroke. At present, stroke remains a significant burden and is the leading cause of disability as well as the leading preventable cause of disability in women. 43 It is critically important to identify women at higher risk for stroke and our study provides evidence that early relevant secondary prevention measures for stroke should be implemented in women with a high number of pregnancies.
We acknowledge some limitations to our study. First, we used women with zero pregnancies as a baseline control, and these women may suffer from infertility or have more severe systemic diseases that contraindicate pregnancy, conditions that may have an impact on the occurrence of ASCVD and thus bias our findings. Second, the data for this study were obtained from the NHANES questionnaire and may be subject to recall bias. Third, we were unable to control for some common confounders such as diet, exercise, and sleep habits, and further research on this information is needed to support the results of this study.
Conclusion
In conclusion, we have found that a higher number of pregnancies was associated with a higher risk of ASCVD after menopause, especially among women aged 45–64 years. In subgroup analysis, we found this association to be particularly significant in the risk of stroke, CHD, and heart attack. These findings suggest that clinicians should consider the number of pregnancies when assessing ASCVD risk in women, and further quantify the ASCVD risk assessment scales of women with different numbers of pregnancies.
Footnotes
Acknowledgment
The authors thank the Natural Science Foundation of Fujian Province for its support and the participants and staff of the NHANES database for valuable contributions.
Authors’ Contributions
Q.H.C.: review and editing (equal). J.G.: Conceptualization (lead); writing—original draft (lead); formal analysis (lead); writing—review and editing (equal). L.L.Z.: Software (lead); writing—review and editing (equal). S.D.: Methodology (lead); writing—review and editing (equal). G.T.X.: Conceptualization (supporting); Writing—original draft (supporting); Writing—review and editing (equal). M.H.H.: Conceptualization (supporting); Writing—original draft (supporting); Writing—review and editing (equal). L.Z.: Conceptualization (supporting); Writing—original draft (supporting); Writing—review and editing (equal).
Author Disclosure Statement
All authors declare that there are no conflicts of interest.
Funding Information
This study was supported by a grant from the Natural Science Foundation of Fujian Province (plan no: 2022J011508; Fujian, China).