
Abstract
Background:
Minimally invasive hysterectomy is preferred to open hysterectomy due to lower morbidity, but recent data regarding the association of surgical approach with patient recovery and opioid consumption are lacking.
Objective:
To analyze how postoperative opioid use and return to baseline activity vary by surgical approach for hysterectomy.
Study design:
This was a retrospective cohort study including hysterectomy patients from the Michigan Surgical Quality Collaborative registry that was linked to the State of Michigan’s prescription drug monitoring program. We analyzed two primary outcomes with respect to surgical approach: opioid consumption in the 30 days following surgery, measured in morphine milligram equivalents (MMEs), and return to baseline activity >4 weeks after surgery. Adjusting for demographics, comorbidities, preoperative opioid use, surgical indication, clinical events at 30 days postoperatively, and surgical approach, we used multivariable linear regression and logistic regression models to identify factors associated with our primary outcomes.
Results:
Lower opioid consumption was reported with minimally invasive hysterectomy, with mean postoperative opioid consumption (95% CI) of 32.70 (27.15–38.26) MMEs for vaginal, 39.91 (37.17–42.65) MMEs for laparoscopic, and 54.97 (48.81–61.13) MMEs for open hysterectomy. Other covariates associated with lower opioid consumption included older age and year of surgery in 2019 versus 2018. Predicted probability of return to baseline activities >4 weeks after surgery was 51% (44–57%), 43% (40–45%), and 64% (60–69%) for vaginal, laparoscopic, and open hysterectomy, respectively.
Conclusion:
Minimally invasive approaches to hysterectomy are associated with lower postoperative opioid consumption and a more rapid recovery relative to open hysterectomy.
Introduction
In the United States, over 600,000 hysterectomies are performed annually. 1,2 Minimally invasive hysterectomy is preferred to open hysterectomy due to decreased morbidity, 3 –7 but data regarding the associations between surgical approach and patient recovery or opioid consumption are still needed. Examination of opioid prescribing and consumption is important in order to address morbidity and mortality related to opioid use. 8 –11 Between 2004 and 2014, postoperative opioid prescriptions increased by more than 50%. 12,13 One recent study revealed that the amount of postoperative opioid prescribed was nearly double the amount used. 8 With 80% of patients reporting that their opioid dependence developed in connection to healthcare and the association between opioid exposure in the perioperative period and persistent opioid use, 7,11,14,15 appropriate prescribing helps to minimize risk.
To this effect, the Opioid Prescribing Engagement Network (OPEN) at the
The analysis of clinical practices, such as choice of surgical approach and efficacy of practice guidelines, enables further refinement of protocols and mitigates patient risks. 7,8,11,18 Therefore, our objective was to leverage a novel dataset combining granular comorbidity data, risk-adjusted outcomes, and patient-reported outcomes from the MSQC with controlled substance data for patients who had hysterectomies in Michigan to analyze time to return to baseline activity and postoperative opioid use by surgical approach.
Materials and Methods
This was a retrospective study of adult women who had undergone a hysterectomy performed for gynecological indications between January 1, 2018 and October 31, 2019 at hospitals participating in the MSQC. MSQC is a collaboration of 70 hospitals that participate in pay-for-performance clinical quality improvement. Our cohort included data from 59 of these 70 hospitals. MSQC cases are selected with a stratified sampling method to capture hysterectomies and a representative distribution of general surgical cases. Surgical Clinical Quality Reviewers (SCQRs), who are employed by participating hospitals, review the medical record and enter demographics, medical history, clinical care processes, and clinical outcomes abstracted into an online registry.
We utilized several inclusion criteria in this analysis. First, patients needed to have valid discharge opioid data (either a prescription or specified as not getting a prescription) and be linked to the State of Michigan’s prescription drug monitoring program (PDMP). The PDMP data were obtained through data sharing agreements between University of Michigan (on behalf of the study team) and State of Michigan Licensing Board (owner of the PDMP data) and the PDMP data vendor (Bamboo Health [formerly Appriss Inc.]) as well as a separate Business Association Agreement with Bamboo Health. The process of obtaining PDMP data linked with patient data has been described in detail previously.
19
Patients were excluded if they matched with more than one patient in the PDMP data as it was not possible to uniquely identify these patients and obtain accurate prescription data. In addition, given that the data sharing agreement for the state PDMP data was limited to Michigan, we excluded patients with addresses outside Michigan. Second, patients had to have completed a questionnaire on patient-reported outcomes regarding their postoperative experience. The protocol for soliciting a questionnaire involved the MSQC hospital’s SCQR emailing or mailing the survey to all eligible patients three times and calling them three times to ask them to fill out the distributed surveys. Patients who did not return these communications or who indicated that they did not wish to participate were excluded from our analysis. Additional exclusion criteria included age <18, non-gynecological cancer as the primary surgical indication, death within 30 days of the procedure, or length of hospital stay >30 days after the procedure (Fig. 1). This study using linked and deidentified data from both MSQC and the PDMP was deemed not regulated by the
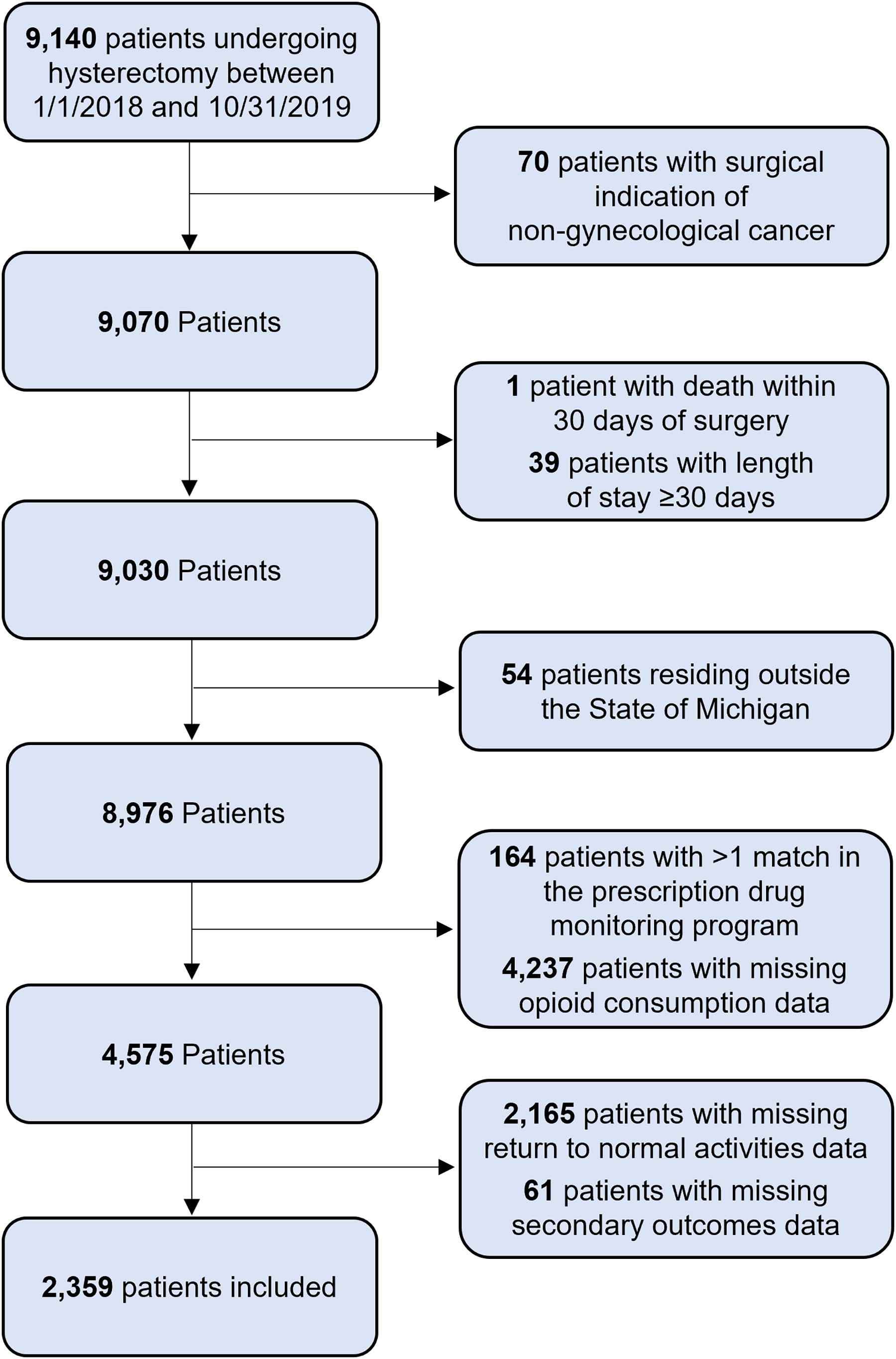
Cohort criteria. Application of predetermined inclusion and exclusion criteria was applied to our patient pool, narrowing the cohort from 9,140 to 2,359. All analyses were performed on this group of patients.
Clinical characteristics
The primary explanatory variable was a surgical approach for hysterectomy abstracted from the clinical record and categorized as vaginal, laparoscopic, or open. Laparoscopic hysterectomy included supracervical and total hysterectomy. Laparoscopic-assisted vaginal hysterectomy was classified in the laparoscopic group.
Additional explanatory variables included patient demographics, comorbidities, primary indication for the surgery, year of surgery, preoperative opioid use, and 30-day postoperative clinical events. Demographics abstracted into the MSQC Registry included age, race, ethnicity, and commercial versus public insurance (Medicare or Medicaid). Comorbidities included diabetes, tobacco use in the year before surgery, chronic obstructive pulmonary disease (COPD), sleep apnea, hypertension, history of cancer, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, and immunosuppression. Surgical indication was based on the primary ICD-10 codes for hospitalization. Categories included gynecological cancer; a menstrual disorder (e.g., abnormal uterine bleeding or pelvic pain due to fibroids or endometriosis); conditions considered premalignant (including cervical dysplasia or endometrial hyperplasia); conditions of uncertain malignant potential (e.g., adnexal or uterine masses); inflammatory diseases; pelvic organ prolapse; and other (Supplementary Appendix SA1). Preoperative opioid exposure was assessed using PDMP data and was defined as at least one opioid prescription fill period between 365 days and 1 day prior to admission for surgery. Postoperative clinical events included minor complications (e.g., urinary tract infection, superficial surgical site infection) and major complications (e.g., deep or organ space surgical site infection, cardiac complications, pneumonia, venous thromboembolism). Utilization of postoperative services included reoperation, emergency department (ED) visits, and readmission within 30 days of the primary procedure.
Outcomes
One primary outcome was patient-reported postdischarge opioid consumption, measured in MMEs, for 4 weeks following surgery. Data regarding mean prescribed MME (obtained from MSQC data) and mean filled MME (obtained from MAPS data) were collected and included as supplemental information for the primary outcome. The other outcome was patient recovery, measured in length of time until return to baseline function dichotomized into >4 weeks or <4 weeks. Within the patient questionnaire, “return to baseline function” was defined as return to the patient’s normal everyday social and work activities within the usual postoperative physician-guided restrictions. The patient-reported questionnaire included items regarding opioid use, pain in the first week following surgery, time to return to baseline daily activities, and patient satisfaction. Pain scores in the week following surgery and patient satisfaction were included as secondary outcomes. Questionnaire items and patient scoring scales are outlined in Supplementary Appendix SA2. The questionnaire items outlining opioid use (e.g., type, strength, and quantity of opioid prescribed) were verified by the data abstracted from the patient’s electronic medical record by the MSQC SCQR to ensure accurate prescription data.
Statistical analyses
Descriptive statistics were calculated for all covariates based on surgical approach. Univariate differences between groups were assessed using the Chi-square test. A multivariable linear regression model with robust standard errors was used to evaluate the association of surgical approach (vaginal versus laparoscopic versus open) and opioid consumption, adjusting for demographics, comorbidities, preoperative opioid use, surgical indication, year of surgery, and 30-day postoperative outcomes. A multivariable logistic regression model was used to assess the association of surgical approach and return to baseline activity >4 weeks after surgery, adjusting for the above-mentioned factors. The secondary outcomes of satisfaction and pain in the week after surgery were calculated based on surgical approach and were analyzed with descriptive statistics and the Chi-square test.
To examine if care complications influenced our primary outcomes, we performed a sensitivity analysis in which we excluded patients with ED visits, reoperation, or readmission within 30 days of the primary procedure to determine if there was a difference in predicted postoperative opioid consumption in MMEs and odds of returning to baseline activity >4 weeks after surgery.
To assess for selection bias, we compared the characteristics of patients included in our cohort with the patients who were excluded due to the lack of data for all outcomes using descriptive stats and Chi-square test.
All analyses were performed with Stata version 17.0 (StataCorp). The p values were two-tailed, and significance was set at p < 0.05.
Results
There were 9,140 hysterectomy patients who had valid discharge opioid data in the MSQC registry and 4,575 patients who had opioid consumption data from MSQC and PDMP data. After excluding patients with missing data for outcomes and various other reasons, our cohort had 2,359 patients (Fig. 1). The characteristics of the 2,359 patients included in the cohort and the 6,453 patients excluded due to the lack of complete data for all outcomes were similar (Supplementary Table S1).
Patients’ clinical characteristics were analyzed by surgical approach (Table 1). Surgical approach was vaginal for 321 patients (13.6%), laparoscopic for 1,613 patients (68.4%), and open for 425 patients (18.0%). There were significant differences in the distribution of age, race and ethnicity, insurance type, BMI, ASA class, surgical indication, history of non-gynecological cancer, preoperative opioid use, and rates of complications (Table 1). We did not find differences in the rates of diabetes mellitus, hypertension, smoking, COPD, immunosuppression, reoperation, ED visits, or readmissions.
Cohort Characteristics
Data presented as n (%).
DM, diabetes mellitus; COPD, chronic obstructive pulmonary disease; ASA, American Society of Anesthesiology; ED, emergency department; BMI, body mass index.
Opioid consumption was lowest after vaginal hysterectomy
Postoperative opioid consumption differed significantly by surgical approach in unadjusted and adjusted analyses. Unadjusted consumption was the highest for open hysterectomy (mean MME = 57.6, SD = 66.9), followed by laparoscopic hysterectomy (mean MME = 40.0, SD = 58.9) and vaginal hysterectomy (mean MME = 28.7, SD = 45.0). In a multivariate analysis, compared to laparoscopic hysterectomy, open hysterectomy was associated with higher opioid consumption and vaginal hysterectomy was associated with lower opioid consumption. Using this model, we calculated the predicted mean postoperative opioid consumption having adjusted for other factors including demographics, comorbidities, preoperative opioid use, surgical indication, year of surgery, and 30-day postoperative outcomes. In the adjusted analysis, mean postoperative opioid consumption was lowest among those who underwent vaginal hysterectomy (32.70 MME, 95% CI: 27.15–38.26), intermediate with laparoscopic hysterectomy (39.91 MME, 95% CI: 37.17–42.65), and highest with open hysterectomy (54.97 MME, 95% CI: 48.81–61.13) (Table 2). In reference, this is equivalent to mean oxycodone consumption of 4.36, 5.32, and 7.33 5 mg tablets of oxycodone in vaginal, laparoscopic, and open hysterectomy, respectively. Descriptive statistics of mean prescribed MME and mean filled MME stratified by surgical approach can be found in Supplementary Table S2.
Linear Regression Model for Postoperative Opioid Consumption a
Only statistically significant data included.
Additional demographic and clinical factors associated with opioid consumption from the multivariable linear regression model are shown in Table 2. When analyzed by age ranges, younger women consistently had higher adjusted opioid consumption compared to women aged ≥65 (Fig. 2A). Those who smoked, had Medicare or Medicaid (versus private insurance), or with preoperative opioid use also had higher postoperative consumption. Specifically, patients who filled an opioid prescription in the year prior to surgery demonstrated a higher mean opioid consumption, regardless of surgical approach (Fig. 2B). Lower consumption was identified among those who had surgery in 2019 versus 2018. There was no significant association with other preoperative comorbidities, demographics, or postoperative complications.

Adjusted mean opioid consumption by surgical approach and preoperative opioid use, and by age.
In a sensitivity analysis to examine the effect of readmission, reoperation, or ED visits on opioid consumption, we excluded 220 patients who had such an event within 30 days of surgery and reproduced the linear regression model. After adjustment for the aforementioned covariates, the adjusted mean opioid consumption for vaginal, laparoscopic, and open hysterectomy was 29.67 MME (95% CI: 24.46–34.88), 39.13 MME (95% CI: 36.21–42.05), and 52.38 MME (95% CI: 45.90–58.86), respectively.
Time to return to baseline activities varied by surgical approach
Return to baseline activities >4 weeks after surgery differed by surgical approach in unadjusted and adjusted analyses. In the unadjusted analysis, return to baseline activities >4 weeks after surgery was 52.6%, 42.3%, 64.7% for vaginal, laparoscopic, and open hysterectomy, respectively. In the adjusted analysis, the predicted probability of return to baseline activities >4 weeks after surgery was 51%, (95% CI: 44–57%), 43% (95% CI: 40–45%), and 64% (95% CI: 60–69%) for vaginal, laparoscopic, and open hysterectomy, respectively (Fig. 3).
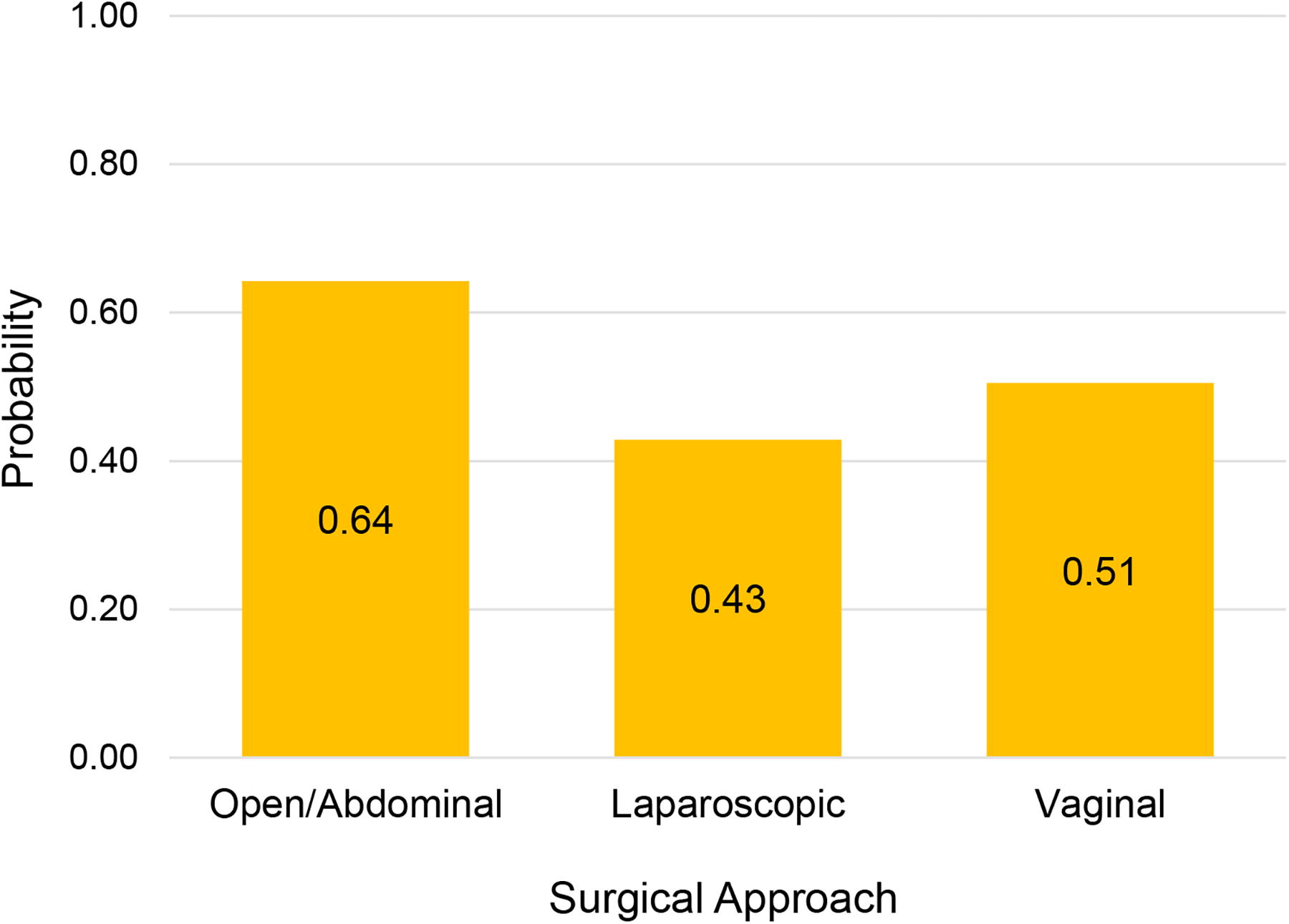
Average predicted probability of return to baseline daily activities in >4 weeks. Predicted probability of return to baseline daily activities was analyzed using a multivariable logistic regression model. Return to baseline activities in >4 weeks differed by surgical approach. The predicted probability of a return to baseline activities >4 weeks after surgery was highest in the open cohort (0.64), intermediate in the vaginal cohort (0.51), and lowest in the laparoscopic cohort (0.43).
Adjusted odds of a delayed return to baseline activity were calculated for demographic and other clinical characteristics in a multivariable model, with significant factors listed in Table 3. Women with a diagnosis of diabetes and a hemoglobin A1c > 6.5% and those with a history of non-gynecological cancer had improved recovery, with lower predicted probability of returning to baseline activities >4 weeks of surgery. Women readmitted within 30 days had higher odds of returning to baseline activities >4 weeks after surgery. ED visits and reoperation were not associated with return to baseline activities >4 weeks after surgery, nor were age, BMI, other comorbidities, or gynecological cancer. In the sensitivity analysis where we excluded patients who had readmission, reoperation, or an ED visit within 30 days of surgery, predicted probabilities of return to baseline activities >4 weeks after surgery were 49% (95% CI 43–56%), 42% (95% CI 40–45%), and 64% (95% CI 59–69%) for vaginal, laparoscopic, and open hysterectomy, respectively.
Logistic Regression Model for Return to Baseline Daily Activities >4 Weeks after Surgery a
Only statistically significant data included.
DM, diabetes mellitus.
Secondary outcomes
Secondary outcomes included patient satisfaction and pain scores in the week following surgery. Significant differences were found in the postoperative pain scores by surgical approach (p < 0.001). In the unadjusted results, severe pain was reported by 9.0% and 9.6% of patients in the vaginal and laparoscopic cohorts, respectively, compared to 17.2% of patients in the open hysterectomy cohort. Little-to-no pain in the first week after surgery was reported by 61.1% of patients who underwent vaginal hysterectomy and 53.5% of patients who had laparoscopic hysterectomy. No significant differences were found in levels of unadjusted patient satisfaction: 94.4% of patients with vaginal hysterectomy, 96.3% with laparoscopic hysterectomy, and 93.6% with open hysterectomy were “satisfied” with their procedure.
Discussion
When compared to open hysterectomy, vaginal and laparoscopic hysterectomy were associated with lower postoperative opioid consumption and more rapid recovery. Our data also revealed that a vaginal hysterectomy approach is associated with the lowest opioid consumption. Consistent with the recommendations from the American College of Obstetrics and Gynecology, 3 these findings support the relationship between minimally invasive techniques and improvements in postoperative recovery in both our vaginal and laparoscopic hysterectomy cohorts and highlight the safety outcomes associated with appropriate use of the vaginal approach for hysterectomy.
With almost 50,000 people dying of opioid overdose nationally in 2019, and the overwhelming majority initiating opioid use in connection with healthcare, 14 our results are evidence of progress in reducing postoperative opioid use. Our data demonstrated a decrease in average opioid consumption between 2018 and 2019. While this trend was overall consistent with other recent studies, 8,20 the average reported median consumption for minimally invasive hysterectomy in our data was much lower (42 MME, approximately 28 mg of Oxycodone) than in another recent publication 20 (75–80 MME, approximately 50 mg of Oxycodone). This difference likely reflects the statewide efforts of OPEN to reduce opioid prescriptions and highlights the importance of developing protocolized prescribing practices. 10,18,21,22
Our study additionally examined several factors previously thought to be associated with postoperative opioid use. Although we did not identify an association between a surgical indication and increased opioid consumption, previous studies have reported this type of connection. 20,23 We suspect that this is a limitation of our available data. While we analyzed a larger cohort of patients from numerous hospitals, we had only the primary indication for hospitalization available. In contrast, the other studies analyzed fewer patients from a smaller number of institutions, which may have afforded an opportunity to consider multiple indications for surgery.
In regard to our data on postoperative recovery, we examined data on a larger scale than previous analyses, providing further evidence regarding the benefits of a minimally invasive approach to hysterectomy. We found that 57% of 1,613 patients with laparoscopic hysterectomy and 49% of 321 patients with vaginal hysterectomy returned to baseline activities within 4 weeks. This is consistent with a recent Cochrane review of 200 patients who returned to baseline activity in 23–25 days and 25–33 days with laparoscopic and vaginal approaches, respectively. 5 This analysis provides a patient-reported outcome regarding return to baseline function among a relatively large number of patients compared to the previous literature.
Our data reflect the impact of developing standard opioid-prescribing practices in an effort to reduce consumption and demonstrate the benefits of a statewide surgical collaborative directing appropriate prescribing. Even lower consumption of opioids may be possible with continued consistent messaging and further protocol development for nonopioid pain management. 11,18,21,22,24 Within our model, we were able to effectively isolate subsets of data to identify several factors associated with opioid use. We found that younger patients consistently had significantly higher opioid consumption compared to older patients, and that those with preoperative opioid use had significantly higher consumption than those without. These factors are important to consider when developing guidelines for patient counseling and when implementing protocols for pain management. Additionally, our data surrounding recovery and opioid consumption by surgical technique can have important implications surrounding perioperative counseling. In instances where a particular technique is necessary for patient factors (e.g., large fibroids necessitating an open approach), our findings highlighting recovery times and opioid use may aid in setting expectations for return to work and other normal activities.
Future research regarding factors related to postoperative outcomes and opioid consumption could provide additional advancements in patient safety and clinical outcomes. While we do have more granular data represented in this analysis than in other previous studies, we still have limited information about mental health conditions, utilization of nonopioid pain relief methods, and roles of social determinants of health. Analysis of these, as well as other potentially contributory factors, could be used to stratify patients’ risk for increased opioid consumption in the postoperative period. On a broader scope, with the development of programs such as OPEN, expanding research efforts to consider the most effective way to produce and disseminate prescribing protocols would assist in addressing the opioid crisis on a systems level.
A strength of our study is its multicenter design with patient outcomes from 59 hospitals in Michigan. Most state policies preclude the use of PDMP data for research; however, the OPEN team obtained a data sharing agreement with the state licensing board to allow for a novel linkage of the MSQC registry and the state’s PDMP. 19 This allowed us to identify the importance of preoperative opioid use on postoperative consumption. It is also important to consider limitations. The generalizability of this retrospective analysis of Michigan patients may be limited by a population that is predominantly White. This is offset to some extent by its inclusion of patients from urban and rural areas, in academic and community hospitals, and with some socioeconomic and geographic diversity. Another limitation is our use of data from a hospital collaboration with an emphasis on clinical quality improvement. However, we recognize that many of these collaborative efforts create frameworks for systems level changes that are widely accessible, which to some extent preserves the generalizability of our findings. There is also the issue of loss of sample size. Patients could not be included in the analysis when MSQC patients did not have patient-reported outcome data or when they could not be linked to the PDMP. There is also the potential for missing opioid prescription data if the patient filled the prescription in another state. It is also important to consider patient opioid use during postoperative hospitalization, which is not included in our analysis and is likely higher for patients in our open hysterectomy cohort. Because of this, the true difference in opioid consumption is likely more than what was noted in our analysis. Another limitation of our data was our inability for our model to capture factors such as chronic pain or opioid use disorder, as these conditions were not included in MSQC data. This may limit our interpretation of the effects of preoperative opioid exposure on postoperative opioid use. Finally, there may be other contributory factors to opioid consumption and recovery that we could not analyze due to our available data.
Conclusions
Our study supports the importance of minimally invasive hysterectomy to improve patient safety and outcomes compared with an open approach, and highlights a trend of decreased opioid consumption during a time of newly disseminated opioid prescribing protocols. We found that vaginal and laparoscopic hysterectomy are associated with lower postoperative opioid consumption and a more rapid return to baseline activities within 4 weeks, with vaginal hysterectomy being associated with the lowest opioid consumption. Further, we identified factors that are important for patient counseling and prescribing practices, such as patient age and preoperative use of opioids.
Footnotes
Acknowledgment
The author would like to acknowledge Sarah Block (Michigan Medicine, Department of Obstetrics and Gynecology), a research editor. Her contributions include visualization, writing, reviewing, and editing.
Authors’ Contributions
J.J.D.: Conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; visualization; writing—original draft; writing—review and editing. C.M.B.: Conceptualization; data curation; funding acquisition; methodology; resources; supervision; writing—review and editing. V.G.: Data curation; formal analysis; resources; writing—review and editing. S.A.-S.: Methodology; resources; supervision; writing—review and editing. D.M.M.: Conceptualization; data curation; formal analysis; investigation; methodology; resources; visualization; writing—original draft; writing—review and editing.
Author Disclosure Statement
C.M.B. is a consultant for Heron Therapeutics, Vertex Pharmaceutical, Benter Foundation, and Alosa Health, and he provides expert testimony for medical malpractice. S.A.-S. is a consultant to Myovant Sciences/Pfizer, Bayer, Organon, Eximis, and she receives Author Royalties from UpToDate. D.M.M. receives UpToDate Royalties. The remaining authors report no conflicts of interest.
Funding Information
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Appendix SA1
Supplementary Appendix SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.