
Abstract
Introduction:
Access to prenatal care offers the opportunity for providers to assess for substance use disorders (SUDs) and to offer important treatment options, but utilization of treatment during pregnancy has been difficult to measure. This study presents pre-COVID trends of a subset of SUD diagnosis at the time of delivery and related trends in treatment utilization during pregnancy.
Materials and Methods:
A retrospective cohort design was used for the analysis of West Virginia Medicaid claims data from 2016 to 2019. Diagnosis of SUDs at the time of delivery and treatment utilization for opioid use disorder (OUD) and non-OUD diagnosis during pregnancy across time were the principal outcomes of interest. This study examined data from n = 49,398 pregnant individuals.
Results:
Over the 4-year period, a total of 2,830 (5.7%) individuals had a SUD diagnosis at the time of delivery. The frequency of opioid-related diagnoses decreased by 29.3%; however, non-opioid SUD diagnoses increased by 55.8%, with the largest increase in the diagnosis of stimulant use disorder (30.9%). Treatment for OUD increased by 13%, but treatment for non-opioid SUD diagnoses during pregnancy declined by 41.1% during the same period.
Conclusions:
Interventions enacted within West Virginia have improved access and utilization of treatment for OUD in pregnancy. However, consistent with national trends in the general population, non-opioid SUD diagnoses, especially for stimulants, have rapidly increased, while treatment for this group decreased. Early identification and referral to treatment by OB-GYN providers are paramount to reducing pregnancy and postpartum complications for the mother and neonate.
Introduction
Owing to its precipitous increase, societal impact, and mortality rate, the opioid epidemic has garnered significant attention in the last decade. 1,2 Despite federal funding, media attention, and increases in access to treatment, the opioid epidemic persists, with the majority of overdose deaths now being attributed to illicitly manufactured fentanyl, often in combination with stimulants. 3
West Virginia has experienced the deleterious effects of the opioid epidemic, with the highest rate of opioid-related overdose deaths and one of the highest rates of maternal and neonatal exposure to illicit drugs in the United States. 4,5 Opioid use during pregnancy is associated with a 4.6-fold increased risk of maternal death during hospitalization. 6 Pregnant individuals with substance use disorders (SUDs) are more likely to experience maternal complications during pregnancy, including severe maternal morbidity. 2,6,7 Nationally, rates of substance use among pregnant individuals have continued to rise, although significant variation is seen across states. 8 Stimulants such as methamphetamine have shown the sharpest increase in recent years. 9
The impact of substance use on the fetus differs depending on the substances used and the gestational period in which use occurs. Exposure in the first 20 weeks of gestation generally impacts the formation and development of cells, whereas exposure in the second half of gestation impacts brain growth and cell differentiation. 10 Different substances impact birth outcomes differently, with the most common neonatal complications being fetal growth restriction, preterm birth, stillbirth, placental abruption, and neonatal abstinence syndrome (NAS). 11
Treatment of any type for SUD during pregnancy improves maternal and neonatal outcomes, increases long-term abstinence, and improves the odds of keeping families together, all of which are critical steps toward reducing the public health burden experienced by communities with high rates of SUD. 12 The recommended treatment for opioid use disorder (OUD) during pregnancy and postpartum includes methadone or buprenorphine medication for opioid use disorder (MOUD) in conjunction with counseling and other medical services. 13,14 The use of methadone or buprenorphine during pregnancy does not prevent neonatal exposure and the possibility of subsequent NAS in newborns; however, it can reduce the severity of NAS symptoms and improve neonatal outcomes. 15 At this time, there are no U.S. Food and Drug Administration (FDA)-approved medications for the treatment of stimulant use disorders. Pregnant individuals involved in programs that combine prenatal care and SUD treatment have higher compliance with prenatal care, are less likely to use substances during pregnancy, report higher levels of satisfaction with treatment, and have improved neonatal outcomes. 16
Motivating factors for entering treatment most commonly identified by pregnant individuals with SUD are not wanting to hurt the baby with continued substance use, avoiding the effects of maternal withdrawal on the fetus, and wanting to retain custody of the child. 17 This makes the integration of prenatal care and SUD treatment both logical and ideal. However, obstetricians often lack training and confidence in treating pregnant women with SUD and identify lack of access to treatment as a barrier to being able to help their patients with SUDs. 18
A significant number of disincentives face pregnant individuals in the decision to disclose substance use during the prenatal period. Individuals experiencing SUDs often report poor treatment by healthcare providers due to stigmatization, 19 –21 and the social stigma of having a SUD during pregnancy can be severe. Even if health care and social stigma are not perceived as issues, pregnant individuals are likely to fear the involvement of state child protection authorities and possible loss of custody of the newborn as well as other children in the home. 22 In addition, some states have enacted criminal penalties for the use of illegal substances during pregnancy; 23 23 states consider substance use during pregnancy to be child abuse under civil child welfare statutes and three states consider it grounds for civil commitment. 24 Although the use of illicit substances is not legally defined as “child endangerment” in West Virginia, the criminal penalties enacted in other states may have increased the fear factor for West Virginians.
In West Virginia and other rural states, nonmedical social determinants of health may also pose significant barriers to pregnant individuals in need of treatment for SUD. 25 For example, treatment barriers may be exacerbated by long travel times, lack of transportation services, and lower family incomes. 26 Moreover, addiction treatment services may not be well-coordinated with other prenatal care services, potentially worsening outcomes. 16
The United States Preventive Services Task Force 27 recommends universal screening for problematic substance use in adults 18 years or older, including pregnant and postpartum individuals. Screening refers to asking one or more questions about drug use or drug-related risks in face-to-face, print, or audiovisual format, but not testing biological specimens for the presence of drugs. 27 Prenatal care visits are an optimal time for screening to occur to facilitate early intervention. However, some concerns have been raised about the use of biological testing for SUD, including limited standardization of tests, mixed evidence concerning the accuracy of test results, and ethical issues over the use of test results (even preliminary test results) as the basis for legal actions against pregnant individuals, such as removal of children from the home. 28
Access to prenatal care can provide a window of opportunity for providers to assess substance use during pregnancy and offer important treatment options. Despite this, treatment utilization has remained relatively low. 29 –31 One national study reported that only 50% of women diagnosed with OUD were receiving medication to manage it. 32 Despite relatively high rates of access to prenatal care in West Virginia, 33 little is known about the proportion of women who need treatment for any SUD during pregnancy and are receiving it.
This study used West Virginia Medicaid claims data to examine the pre-COVID prevalence of SUD diagnosis at the time of delivery, and evidence of SUD treatment utilization for those individuals during the preceding nine months of pregnancy. During this time frame, at the national level, there has been clear evidence of significant increases in the use of methamphetamines in the general population as well as during pregnancy. 9,34 The definition of SUD included OUD, stimulant use disorders, and the use of other psychoactive substances. SUD diagnoses at the time of delivery are largely self-reported and are presumed to only represent a subset of SUD cases in both the total count and the type of substances being used by individuals. Assessing pre-COVID pandemic trends contributes to the future examination of post-COVID pandemic trends for pregnant individuals with SUD and is important to evaluate changing treatment needs.
Materials and Methods
West Virginia Medicaid claims data were made available for this study through a partnership between the West Virginia Department of Health and Human Resources and West Virginia University. A retrospective cohort design was used to examine the Medicaid data from calendar years 2016 to 2019. The primary outcome of SUD was identified at the time of delivery for inpatient hospital and birthing center settings based on principal diagnosis. Up to 15 secondary diagnoses fields were included for the identification of individuals with SUD diagnoses and behavioral health treatment during the prenatal period. The data included unique encrypted identifiers that allowed recognition of individuals over time using anonymous data. We included females aged 12– 52 years with delivery events in any setting (hospital or birthing centers). Claims from 2015 were included for deliveries occurring in the early part of 2016 to capture associated SUD treatment during pregnancy up to 270 days before delivery. Deliveries were identified using ICD-10-CM coding (see Supplementary Table S1). Medicaid claims data are created for billing purposes and include records of all billed services in all inpatient and outpatient settings.
The study presents findings on opioid diagnoses and non-opioid SUD diagnoses present at the time of delivery. It also includes information on specific categories of SUD (opioids, sedatives, stimulants, and other psychoactive substances) (Table 1). In Figure 2, these categories of SUD were collapsed into opioids, stimulants, and “other” use disorders to highlight the significant increase in stimulant use disorder in comparison to the other categories of substances. Other use disorders included sedatives, hallucinogens, inhalants, and other substances less commonly reported (see Supplementary Table S1). The category for inhalant diagnosis was excluded after initial analysis showed extremely small numbers. We did not include alcohol, cannabis, or tobacco-related diagnoses as primary outcomes; however, summary information on the incidence of these diagnoses by year is included in Table 1. Nationally, tobacco and cannabis are the most common substances used during pregnancy; 35 however, it is rare that pregnant individuals are diagnosed or referred to treatment for cannabis or tobacco use disorders. The incidence of documented alcohol use disorder in this cohort was extremely low.
Distribution of SUD Diagnosis at the Time of Delivery
MOUD, medication for opioid use disorder; SUD, substance use disorder; WV, West Virginia.
The secondary outcome of “treatment” was broadly defined as MOUD and/or counseling (see Supplementary Table S1). Diagnoses related to “in remission” or “history of” SUD were excluded. Across all 4 years, Methadone treatment was not captured in the Medicaid dataset; therefore, it was excluded from this study. The low numbers for Methadone treatment are partially due to West Virginia Medicaid not reimbursing for Methadone treatment until 2018.
The unit of analysis was delivery events identified in maternal Medicaid claims data, with each delivery defined as a single pregnancy episode. Not all pregnancy episodes result in a live birth, especially those affected by SUD. To ensure that all affected individuals with SUD in pregnancy were captured, delivery events involving stillbirths were included. Deliveries with associated coding for pregnancy termination procedures were excluded. The data did not include information about the length of pregnancy, and early termination may have decreased prenatal interaction with caregivers where assessment and referral for SUD treatment take place. Rates of opioid diagnosis per 1,000 deliveries over the study period (2016–2019) were examined within age groups in five-year increments between 20 and 40 years of age. (i.e., 12–19, 20–24, 25–29, 30–34, 35–40). The over-40 age group is not included in Figure 1 since reported SUD diagnoses were too small in number to include. Less than 350 individuals were Medicaid beneficiaries for less than 3 months before delivery (e.g., 75 individuals in 2017), and they were included in the study. The study was determined to be non-human subject research by the West Virginia University Institutional Review Board.
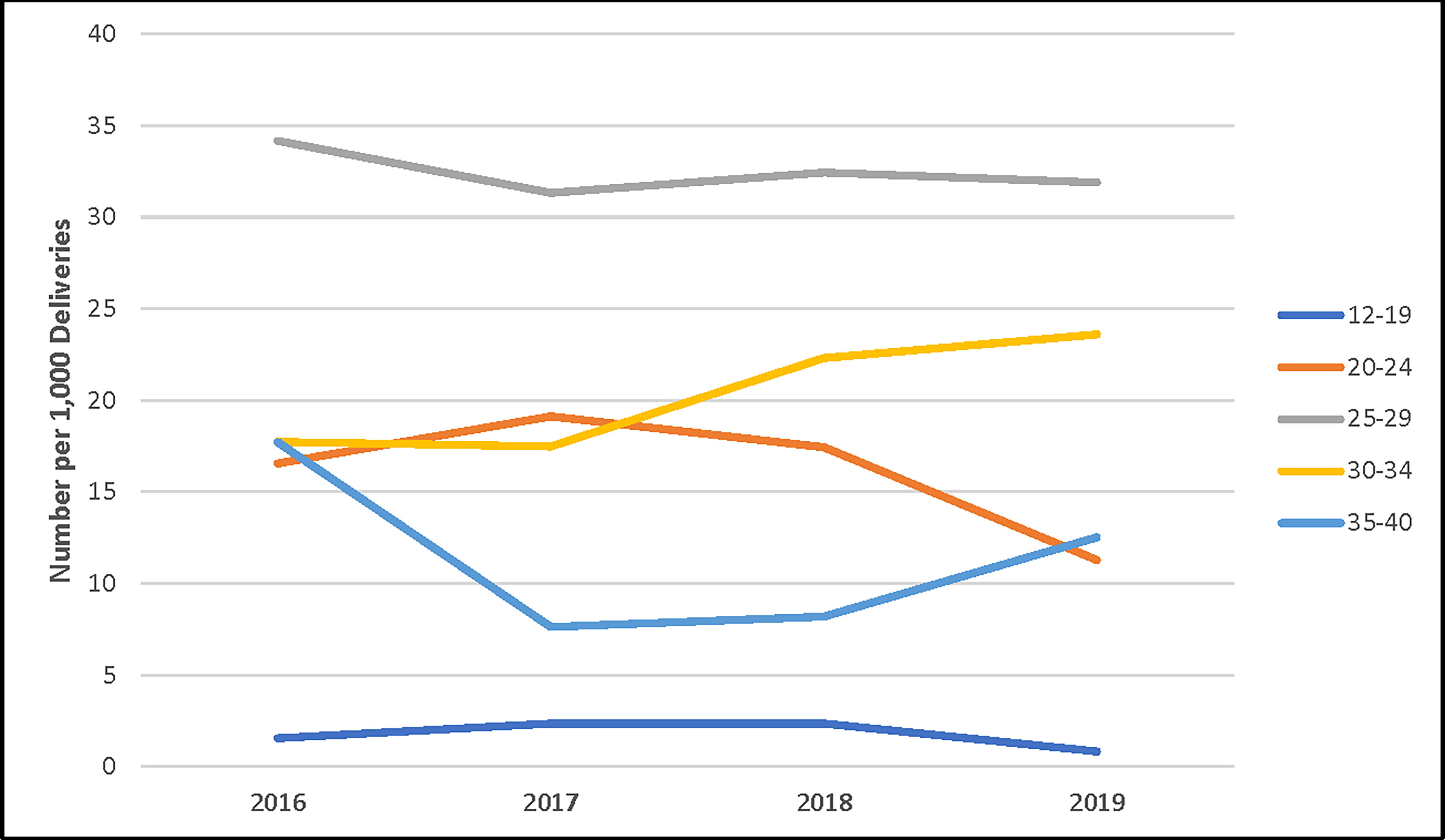
Rate of SUD diagnosis at the time of delivery by age group: West Virginia: 2016–2019. SUD, substance use disorder.
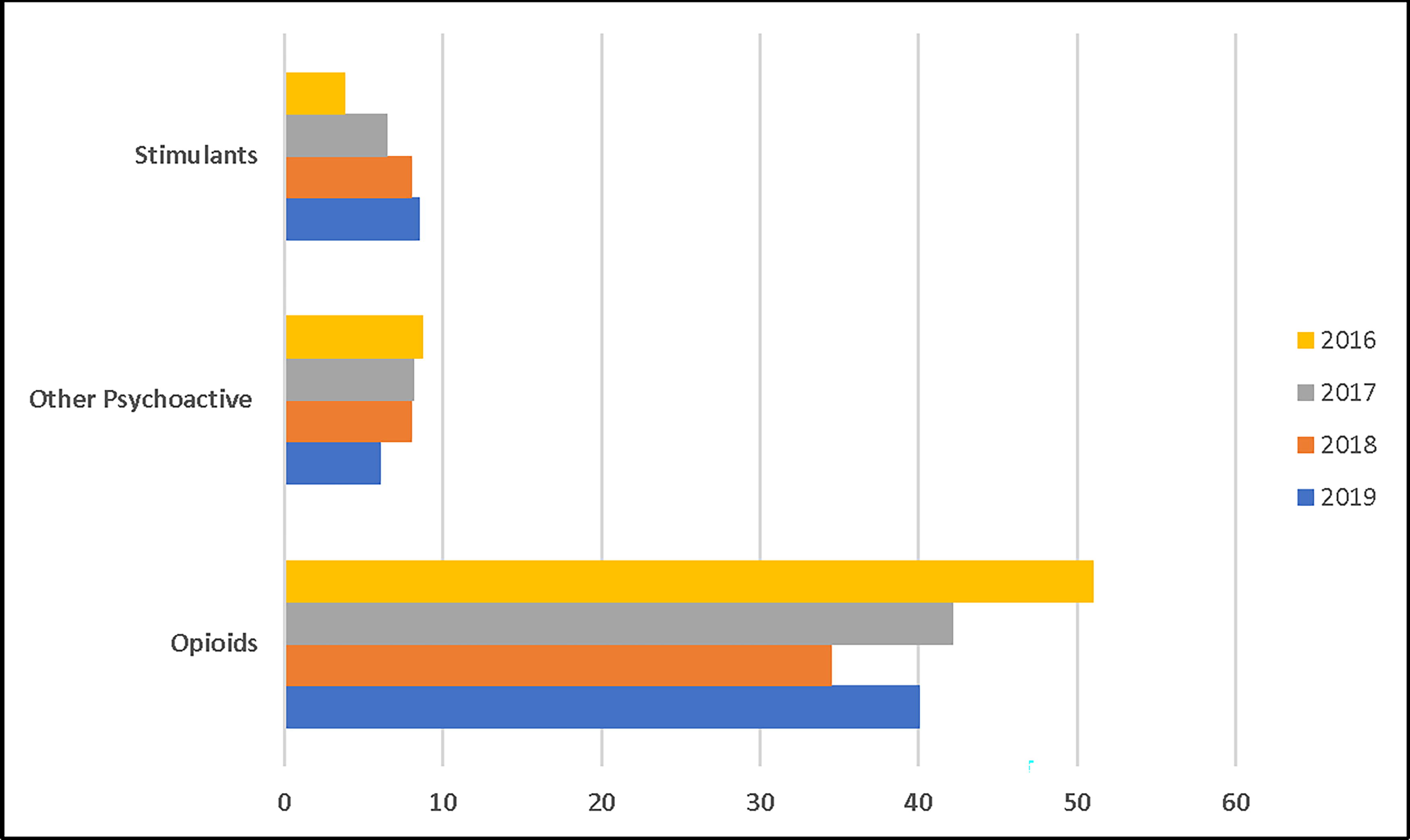
Most frequent categories of SUD diagnosis for West Virginia women at time of delivery: 2016–2019. SUD, substance use disorder.
Data analysis
The Medicaid data analysis used IBM’s Advantage Suite® software to create contingency tables denoting the differences across calendar years in categories of illicit drug use and types of SUD treatment documented during the nine-month period before deliveries. The data analysis was descriptive in nature. A category for methadone treatment was excluded after initial analysis showed extremely small numbers.
Results
Over the 4-year period, 2,830 pregnant individuals had a SUD diagnosis at the time of delivery, with an average annual increase of 8.2% out of a total of 49,398 delivery events (Table 1). OUD diagnosis at delivery declined 29.3% over the study period and accounted for 58% of all SUD deliveries in 2019. In contrast, nonopioid SUD diagnoses increased by 55.8% between 2016 and 2019. Among individuals with nonopioid SUD diagnoses, stimulants had a mean annual increase of 31.9% during the study period.
When examining age groups, the general rate of SUD diagnoses per 1,000 deliveries began to increase in 2018 for the older age groups over 25 years old (Fig. 1). Combining all age groups, pregnant individuals with opioid diagnoses declined from 51 per 1,000 deliveries in 2016 to 40 per 1,000 deliveries in 2019; whereas the rate of pregnant individuals diagnosed with stimulant use disorders increased (Fig. 2).
Among pregnant individuals with OUD diagnoses at the time of delivery, the percentage receiving any treatment (MOUD and/or counseling) before delivery showed a mean annual increase of 30.9% during the study period. In contrast, pregnant women with a non-opioid SUD diagnosis receiving any treatment (MOUD and/or counseling) before delivery showed an annual mean decrease of 41.1%. (Fig. 3).
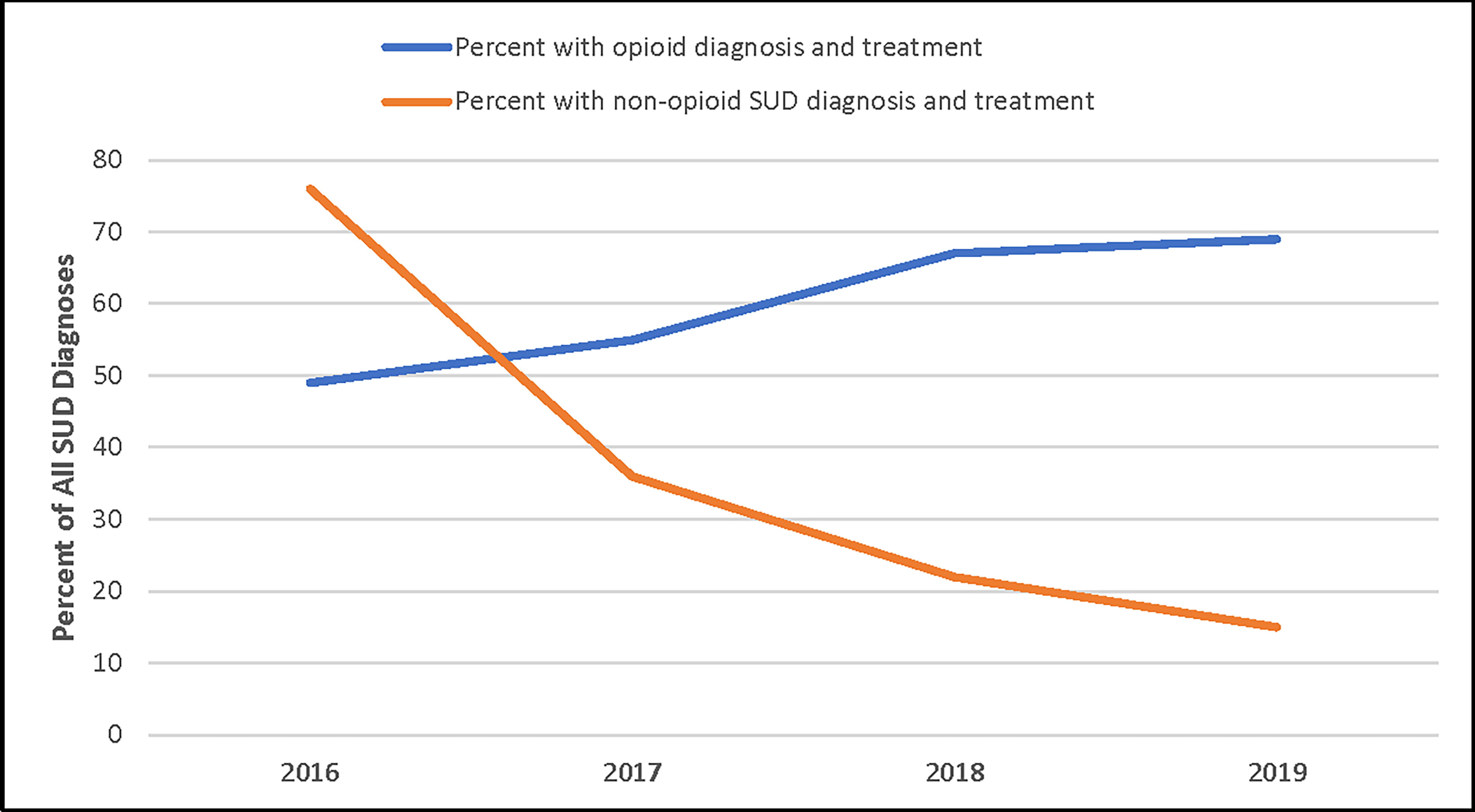
Comparison of prenatal treatment with opioid vs non-opioid diagnosis at time of delivery. SUD, substance use disorder.
Among all pregnant individuals with an OUD diagnosis, there was a mean annual increase of 12.9% in the number of women receiving treatment during pregnancy (Table 1). Conversely, in the SUD group (opioids excluded), the number of pregnant individuals with a SUD diagnosis receiving treatment declined on average by 41.1% annually. Pregnant individuals with a non-opioid SUD diagnosis receiving no treatment showed a mean annual increase of 50.2% over the study period (Table 1).
Owing to the low rates of diagnosis and treatment for cannabis and nicotine use disorder, they were not included as primary outcome measures. It is worth noting that the rate of cannabis use disorder diagnoses showed a mean annual increase of 8.2% from 2016 to 2019. Pregnant women diagnosed with nicotine use disorder remained steady, with less than a 1% annual decrease (Table 1). The general incidence of nicotine use in pregnancy in West Virginia is high, estimated at three times the national average. 36
Discussion
The purpose of the study was to identify substance use and treatment utilization trends among pregnant individuals in West Virginia. In our study, an estimated 8.2% of pregnant individuals in the Medicaid population were diagnosed with some type of SUD at the time of delivery, excluding alcohol use disorder, cannabis use disorder, and nicotine use disorder. Of those with a SUD diagnosis, an estimated 58% had opioid-related diagnoses in 2019.
OUD diagnoses declined over the study period, while the percentage of pregnant individuals receiving treatment increased by 28.9% from 2016 to 2019. The promising downward trend in the diagnosis of OUD among pregnant individuals at the time of delivery, paired against the increase in prenatal treatment, offers potential evidence that efforts initiated under West Virginia’s Opioid Response Plan (2018) have started to yield beneficial outcomes. Buprenorphine and methadone are evidence-based treatments recommended by the American College of Obstetricians and Gynecologists and the American Society of Addiction Medication for the treatment of OUD in pregnant individuals. 37 Federally allocated State Targeted Response and State Opioid Response grant monies helped in the expansion of MOUD services in West Virginia and other states during the period under surveillance. This investment may have had a positive impact on access to and uptake of services among pregnant women with OUD, as reflected in the 40% increase of women receiving this treatment.
Although uptake of treatment for OUD shows improvement, the bigger picture for all types of SUD diagnoses is not as encouraging. We found that individuals with SUD diagnoses involving other nonopioid substances increased by 55.8% over the study period, with the largest increases observed for stimulants (31%). Troublingly, these data suggest that pregnant individuals with nonopioid SUD diagnoses were also less likely to receive treatment. The percentage of individuals receiving treatment declined by an average of 41.1% annually over the study period. These results carry important implications for prenatal care practice, as methamphetamine use during pregnancy has been associated with maternal cardiovascular and placental complications, as well as cardiac arrhythmias, heart failure, pulmonary hypertension, and worsening preeclampsia. 38 Methamphetamine use during pregnancy has been shown to significantly increase the odds of maternal morbidity. 39
Currently, only 19 states have funded or created programs that target pregnant individuals with SUD, and 17 states give pregnant individuals priority access to treatment. 24 In West Virginia, there has been increasing support for services for pregnant individuals with SUD, beginning with the creation of the Drug Free Moms and Babies Project. 40 This program is a comprehensive and integrated medical and behavioral health program for pregnant and postpartum individuals, which supports healthy mother and baby outcomes by providing prevention, substance use screening, early intervention, and referral to treatment and recovery support services. Currently, there are 17 sites in West Virginia statewide that offer this program.
Implications for Practice
The decreased rate of OUD diagnoses and increase in the percentage of individuals receiving treatment for OUD during pregnancy, while very positive, should not be viewed as a sign that the opioid epidemic is waning. In fact, COVID-19 and the increased prevalence of fentanyl use, often in combination with methamphetamines has resulted in continued increases in overdose deaths in the general population from 2019 to 2020 at 29.4% nationally and 45% in West Virginia. 4 In this study, the 55.8% increase in nonopioid SUD diagnoses signals an ongoing problem because nonopioid treatment declined by a mean annual amount of 41.1% during the 2016–2019 time period. Increased use of stimulants and the use of other co-occurring psychoactive drugs are phenomenon that could have impacts on pregnant individuals and infants not yet fully understood. The observed trend in stimulant use among this population poses a treatment challenge since there are no FDA-approved medications presently available for stimulant use disorders, and only four evidence-based treatments to address stimulant use with contingency management. 14,41 One implication for practice includes the need for workforce training in evidence-based treatments for stimulant and co-occurring SUDs.
Nurses and providers working in obstetrics, gynecology, pediatric, and neonatal nursing are optimally positioned to provide compassionate support and care for individuals in any stage of SUD, from active use to remission. Maternal and neonatal outcomes are better among individuals with SUD if they are engaged in routine prenatal care. 12 The most crucial role of the care provider in the perinatal setting is to support an environment of care that is free from stigma. This can be attained by increasing access to continuing education regarding perinatal SUD. Understanding of the variety of MOUDs available, as well as the limitations of those medications in managing non-OUDs, is crucial. Those working in the fields of neonatology or pediatrics may not provide direct care to the peripartum individual with prior or current OUD or SUD, but they will interact with them as they provide care for children with intrauterine substance exposure. Nurses and providers caring for children with intrauterine substance exposure have a large influence on the healthcare experience. The overlap in care directs us to the need for dyad-focused (instead of individual-focused) health care. Strategies to reduce stigma toward pregnant individuals with SUD include using nonstigmatizing language in healthcare settings, sharing sympathetic narratives related to individuals with SUD, and messages focused on treatment effectiveness. 42 Stigma reduction can increase the willingness of policy makers to allocate resources, patients’ comfort with accessing treatment, and providers’ interest in working with individuals with SUDs. 43
Prenatal care appointments provide practitioners and nursing staff the opportunity to connect individuals to resources, screen them for dangerous illnesses or injuries, and assess for intimate partner violence. The policies of specific clinics and facilities surrounding urine drug testing, umbilical cord tissue testing, and meconium testing directly impact how much individuals access care. 12 Nurses and providers can advocate to establish policies for testing that balance appropriate screening and safety measures with the protection of privacy and promotion of recovery. Policies surrounding testing and mandatory reporting should be discussed with clients prenatally in a transparent manner. By maintaining open communication with the patient, care providers in the clinic and hospital setting can improve the patient experience by providing education on expectations and care. Initiating screening early and often are necessary steps to refer promptly to treatment. Initiating intervention during pregnancy contributes to improvement in the dyad outcome along the peri and postnatal journey. Based on the increased use of nonopioid substances noted in this study, it is crucial that screening include assessment for the use of all substances, not just opioids.
Limitations
Our study has several important limitations. The study design did not incorporate the identification of causal relationships for the decrease in OUD diagnosis and increase in treatment nor for the increase in stimulant use disorder diagnosis and lack of treatment uptake during pregnancy.
Longitudinal study designs determine temporal associations only. Also, the use of diagnostic categories “opioid vs. nonopioid” was created to be mutually exclusive for this study; however, co-occurring substance use is a widely reported problem and increasingly the norm among individuals with SUDs, including pregnant individuals. 9,34 Similarly, the definition of maternal prenatal “treatment” in our study was very broad, and in addition to MOUD, included any encounter for behavioral health counseling even if SUD treatment was not specified in the ICD-10 coding. The assumption was that any behavioral health encounter is likely to have a positive impact on outcomes for those with SUD and that in any behavioral health treatment, SUD-related issues are addressed. It is possible that individuals with Medicaid benefits received treatment not reflected in the claims data. Claims data are also likely to represent an undercount of SUD diagnoses, and these were limited to those covered by Medicaid only. Additionally, carve-outs for mental health and substance use services are common in many Medicaid programs, which could affect estimates from the analytical strategy we designed and implemented. However, the majority of behavioral health services are carved in by West Virginia Medicaid. 44
The estimates are not presumed to represent the entirety of pregnant people in West Virginia or in other states but constitute a sample with adequate numbers to be representative of trends before COVID-19. Rates of neonatal exposure are higher among Medicaid recipients in West Virginia, with 86% of infants diagnosed with NAS enrolled in Medicaid. 45 With regard to generalizability, as with all studies using an ecological design, there is a risk of ecological fallacy, i.e., assuming the associations that exist at the population level are also present at the individual level.
Conclusion
The study found that the rate of opioid diagnoses at the time of delivery decreased, while the prenatal treatment rates for OUD increased. This indicates progress made toward better outcomes for mothers and babies in West Virginia. However, the rate of nonopioid SUD diagnoses increased, while treatment for this group decreased during the same time period. Stimulants appear to be driving the increased prevalence of nonopioid SUD diagnosis. Strategies for early identification in the perinatal setting and referral to treatment are needed and should attempt to address the numerous disincentives pregnant people face that serve as barriers to seeking treatment.
Future research should explore whether trends observed in this study are observed in pregnant people in other states’ Medicaid populations. Further research needs to be conducted examining post-COVID treatment utilization with the proliferation of teletherapy increasing access for rural populations. 46
Footnotes
Acknowledgments
The authors would like to acknowledge Jordan Wilton, senior consultant at IBM Watson Health, for his expert assistance in the use of the West Virginia Medicaid data.
Authors’ Contribution
C.S.: Conceptualization, Methodology, Formal analysis, Resources, Writing—Original draft, Visualization, Funding acquisition. L.R.L.: Methodology, Writing—Original draft K.Z.: Methodology, Writing—Original draft S.D.: Methodology, Writing—Review & editing K.L.: Writing—Review & editing
Disclaimer
The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the Department of Health and Human Resources or West Virgnia University.
Ethics Approval and Consent to Participate
This project does not constitute research involving human subjects. The data utilized are from the West Virginia Medicaid claims (not Medicaid records). The data are permitted to be used only for authorized research and public health projects under the provisions spelled out in the Memorandums of agreement.
Author Disclosure Statement
The authors of this article declare that they have no personal or financial competing interests to disclose.
Funding Information
This publication was supported by the West Virginia Department of Health and Human Resources and the West Virginia University Office of Health Affairs.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.