
Abstract
Background:
Research on the association between age at menarche and menopause, reproductive lifespan, and the risk of obesity in China is unclear and requires further clarification.
Materials and Methods:
Data were obtained from the China Hypertension Survey, a cross-sectional study using a stratified multistage random sampling method, conducted from October 2012 to December 2016, with a total of 187,162 women included in the analysis. Logistic regression models and restricted cubic spines were used to estimate the relationship between obesity and age at menarche, age at menopause, and reproductive lifespan.
Results:
The mean (standard deviation) age at menarche and menopause, and reproductive lifespan were 15.5 (1.8), 48.7 (3.5), and 33.2 (3.9) years, respectively. Age at menarche was negatively related to the risk of obesity (odds ratio [OR]: 0.968; 95% confidence interval [CI]: 0.961–0.975). There was a positive association between age at menopause and the risk of obesity in postmenopausal women (OR: 1.019; 95% CI: 1.014–1.023). Reproductive lifespan was positively related to obesity (OR: 1.020; 95% CI: 1.017–1.025). The restricted cubic spines showed the association between age at menarche, age at menopause, reproductive lifespan, and obesity was nonlinear when fully adjusted.
Conclusions:
Based on the large nationally representative sample, Chinese women with earlier age at menarche, later age at menopause, and longer reproductive lifespan have a higher risk of obesity.
Introduction
Obesity affected 603.7 million adults worldwide and accounted for 2.4 million deaths worldwide. 1 According to Chinese criteria, the prevalence of adults with obesity was 16.7% in 2020, making China to be the country with the highest number of people with overweight or obesity in the world. 2,3 In people with obesity, 41% of body mass index (BMI)-related deaths were due to cardiovascular disease (CVD). 1 Strong evidence from prospective cohort studies had linked overweight and obesity to increased risk of major noncommunicable diseases and premature mortality in Chinese populations. 2 Among adults, the prevalence of overweight and obesity used to be lower in men than in women, but the difference has narrowed or even reversed in recent years. Data from the first China Chronic Disease and Risk Factor Surveillance in 2013–2014 showed that the prevalence of obesity was 14.0% in men and 14.1% in women. 4 Female obesity has become an increasingly important public health issue in China.
The age of menarche and menopause, as well as reproductive lifespan, were associated with cardiovascular diseases and all-cause mortality, 5 but the relationship with obesity varies among studies and even is contradictory. Existing studies had found that age at menarche was negatively and completely linearly related to obesity, 6 –8 but there was other study reported that this linear relationship began at a certain age and that early age at menarche was not associated with obesity. 9 Yang et al. reported findings from China Kadoorie biobank study that age at menopause and total reproductive years were linearly and positively correlated with BMI and waist circumference. 8 However, the Framingham Heart Study found age at menopause was not associated with measures of body composition including BMI, waist circumference, visceral adipose tissue, and subcutaneous adipose tissue. 10
In addition, the dramatic fall in estrogen production after menopause may contribute to weight gain and changes in adipose tissue distribution. Women with obesity have been identified as high-risk subgroups for further progression to prediabetes, type 2 diabetes mellitus (T2DM), and potentially CVD. 11 The impact of obesity on cardiovascular events is greater with increasing age at menopause. There were significant interactions of menopausal age with BMI for heart failure incidence in women who experienced menopause at age ≥55 years. 12 Women who had obesity with a short reproductive lifespan (<35 years) at baseline showed a higher risk of T2DM and hypertension. 13
These influences have been studied in combination with obesity in relation to other diseases, but the relation with obesity alone is not well studied. Research should move forward from diseases such as cardiovascular events to the study of obesity risk factors, which means moving from prevention of disease to prevention of risk factors for disease. This is a large study to comprehensively investigate the relationship between age of menarche and menopause, reproductive lifespan, and risk of obesity in Chinese women, using a nationally representative sample and assessing multiple subgroups of individual characteristics and lifestyles.
Materials and Methods
Study design and participants
All participants in this study were from the China Hypertension Survey conducted in China from October 2012 to December 2016. 14 The stratified multistage random sampling method was used to sample the general population aged ≥18 years in 31 provinces of the Chinese Mainland. The specific sampling method has been described in detail in the previous articles. 14,15 A total of 451,755 participants from 262 urban resident cities and rural counties were enrolled, of which 218,133 were female subjects. After excluding women with missing or implausible information (n = 31,007), a total of 187,126 women were included in the final analysis including 100,393 women who were premenopause and 86,733 women who were postmenopause (Fig. 1).

Flowchart of inclusion and exclusion of study participants.
Written informed consent was obtained from each participant before data collection. This study (No. 2011BAI11B01) was approved by the ethics committee of Fuwai Hospital, Beijing, China. All procedures were in accordance with the 1964 Helsinki Declaration.
Data collection
All subjects were interviewed by trained staff using standard questionnaires developed by Fuwai Hospital, which covered social–demographic characteristics, lifestyle factors, and reproductive factors. Physical examinations were conducted by trained physicians and nurses. Fixed measuring belt and standard right-angle device (accurate to 0.1 cm) were used to measure the height without shoes. The OMRON body fat meter was used to measure the weight without wearing thick clothes.
Definitions
Age at menarche and menopause were self-reported by participants. Menopause status was defined based on the World Health Organization’s definition of menopause as the absence of menstruation for ≥12 months. The reproductive lifespan was defined as the interval between age at menarche and menopause.
BMI was calculated as weight divided by the square of height (kg/m2). Obesity was defined as BMI ≥28.0 kg/m2. Current alcohol drinking was defined as having consumed alcoholic beverages at least once a week in the past month. Current smokers were defined as people who smoked at least 20 packs of cigarettes lifetime and were still smoking. Vegetable–fruit dietary pattern was defined as eating fresh vegetables and fruits at least once a day. Physical exercise referred to doing strenuous or physical activities (e.g., football, biking, walking) that increased breathing and heartbeat rate at least three times a week. Parity means the number of children a woman has in her lifetime.
Statistical analysis
Baseline characteristics of participants were presented as means and standard deviations (SD) for normally distributed data and proportions for categorical data. The χ2 test and variance analysis were used to compare variables between the different groups. Logistic regression models were used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) between obesity and age at menarche (classified as ≤13, 14, 15, 16, and ≥17 years, with 15 as the reference), age at menopause (classified as ≤45, 46–48, 49–51, 52–54, and ≥55 years, with 49–51 years as the reference group), and reproductive lifespan (classified as ≤28, 29–31, 32–34, 35–37, and ≥38 years, with 32–34 years as the reference). The restricted cubic splines were performed to explore the nonlinearity, which were specified with three knots. And the comparison between excluded women and included in the analyses is shown in Supplementary Table S1.
In logistic model 1, we adjusted for age at recruitment (continuous), model 2 plus region (urban or rural), ethnicity (Han or other ethnicities), marital status (unmarried/widowed, married/cohabiting), education level (elementary or below, junior high school, high school or above), alcohol drinking (yes or no), smoking (yes or no), vegetable–fruit dietary pattern (yes or no), physical exercise (yes or no), and contraceptive use status(yes or no); model 3 plus contraceptive use status (yes or no) and breastfeeding experience (yes or no), parity (0–1, 2, ≥3). When analyzing the association between age at menarche and obesity in model 3, we further adjusted menopause status (yes or no). When analyzing the association between age at menopause and obesity in model 3, we further adjusted age at menarche.
p < 0.05 was considered to be statistically significant. And R 3.6.2 (http://www.r-project.org) was used to conduct our analyses.
Results
The characteristics of the study participants by age at menarche, menopause, and reproductive lifespan were listed in Tables 1, 2, and 3, respectively. The mean (SD) age at recruitment was 50.6 (16.4) years, and the mean (SD) age of menopause women was 64.6 (10.3).
Characteristics of Study Participants by Age at Menarche
Percentages were calculated based on women with complete information for that specific variable.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; SD, standard deviation.
Characteristics of Study Participants by Age at Menopause
Percentages were calculated based on women with complete information for that specific variable.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; SD, standard deviation.
Characteristics of Study Participants by Reproductive Lifespan
Percentages were calculated based on women with complete information for that specific variable.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; SD, standard deviation.
In the total population, the mean (SD) BMI and parity were 20.4 (3.7) kg/m2 and 2.9 (1.8), respectively. A minority of women were smokers (1.9%), alcohol drinkers (6.2%), and users of contraceptives (7.1%). Most women had breastfeeding experience (95.3%).
Restricted cubic splines suggested the relationship between age at menarche, age at menopause, reproductive lifespan, and obesity with restricted cubic splines (Fig. 2). The relationship between age at menarche and obesity was linear when adjusting for age at recruitment only (p for nonlinearity = 0.075), and became nonlinear when adjusting for more covariates when age at menarche exceeded 15 years; the rate of OR reduction decreased. The relationship between age at menopause and obesity was J-shaped with an inflection point of 50 years and significant nonlinear. And the relationship between reproductive lifespan and obesity was also nonlinear in all models, with the increase in OR becoming faster when reproductive life expectancy exceeded 34 years. The relationship between age at menarche and obesity was further analyzed in premenopausal and postmenopausal populations (Supplementary Fig. S1). In premenopausal women, the ORs fluctuated significantly across the range of age at menarche. The curves showed that both very early and very late ages at menarche were associated with higher odds of obesity compared to ages around 13 years, where the OR was closer to 1. In postmenopausal women, the ORs were more stable across the range of ages, suggesting a linear relationship between age at menarche and obesity.
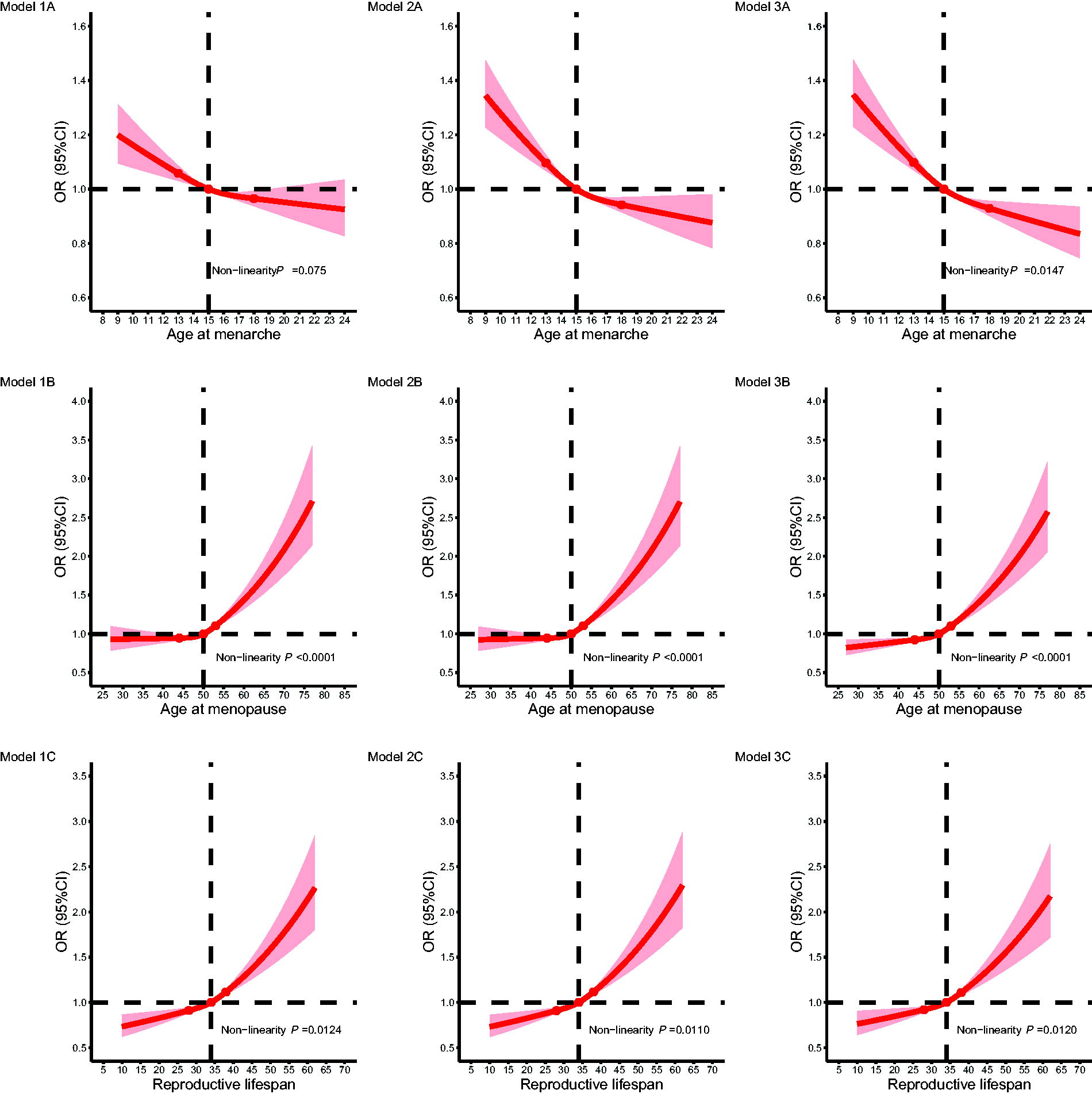
The dose–response relationship between age at menarche, age at menopause, reproductive lifespan, and obesity with restricted cubic splines. Models 1A, 1B, and 1C: adjusted for age at recruitment. Models 2A, 2B, and 2C: models 1A, 1B, and 1C plus region, ethnicity, marital status, education level, alcohol drinking, smoking, vegetable–fruit dietary pattern, physical exercise, and contraceptive use status. Models 3A, 3B, and 3C: models 2A, 2B, and 2C plus contraceptive use status, and breastfeeding experience, parity; model 3A more plus menopause status; models 3B and 3C more plus age at menarche.
Figure 3 shows the ORs for obesity events by age at menarche, age at menopause, and reproductive lifespan among women. In models 1, 2, and 3, the relation between age at menarche and menopause, reproductive lifespan, and obesity was significant. Model 3 showed that for those with age at menarche ≤13, 14, 15 (ref), 16 and ≥17 years, the ORs (95% CIs) were 1.16 (1.11–1.21), 1.04 (1.00–1.08) 1.00 (ref), 1.05 (1.00–1.10), and 0.97 (0.93–1.01), respectively, and for those with age at menopause ≤45, 46–48, 49–451 (ref), 52–54, and ≥55 years, the ORs (95% CIs) were 0.95 (0.90–1.00), 0.94 (0.90–0.99), 1.00 (ref), 1.20 (1.14–1.26), and 1.22 (1.14–1.31), respectively, for those with reproductive lifespan ≤28, 29–31, 32–34 (ref), 35–37, and ≥38, the ORs (95% CIs) were 0.91 (0.86–0.97), 0.94 (0.89–0.99), 1.00 (ref), 1.07 (1.02–1.12), 1.20 (1.13–1.27), respectively. Those with age at menarche ≥17 years, age at menopause 46–48 years, and reproductive lifespan ≤28 years had the lowest risk.
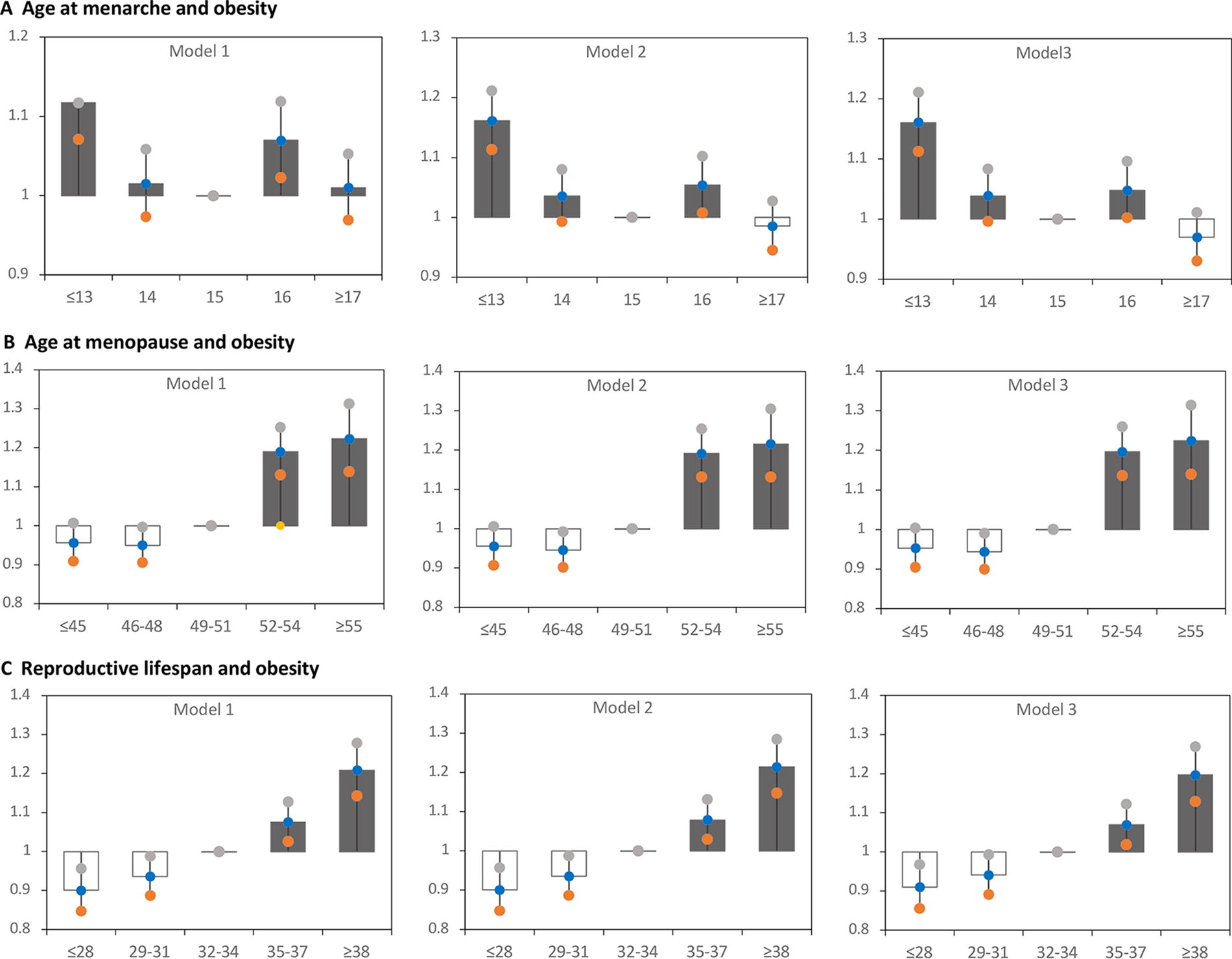
Adjusted odds ratios (ORs) (95% confidence intervals [CIs]) for obesity by age at menarche, menopause, and reproductive lifespan among Chinese women.
As shown in Figure 4, age at menarche was negatively related with the risk of obesity, with an adjusted OR (95% CI) of 0.968 (0.961–0.975) per year. For every 1-year increase in age at menarche, the risk of obesity decreased by 3.2%. The relation between age at menopause and risk of obesity was also significant, with an adjusted OR (95% CI) of 1.019 (1.014–1.023) per year. For every 1-year increase in age at menarche, the risk of obesity increased by 1.9%. Longer reproductive lifespan was related to obesity events, with an adjusted OR (95% CI) of 1.021 (1.017–1.025) per year. For every 1-year increase in reproductive lifespan, the risk of obesity was increased by 2.1%.

Adjusted odds ratios (ORs) (95% confidence intervals [CIs]) for obesity per year by age at menarche, age at menopause, and reproductive lifespan within various subgroups.
Subgroup analyses were also conducted according to region, age at recruitment, region, marital status, education level, ethnicity, breastfeeding experiences, current alcohol drinker, smoking, use of contraceptives, and parity. The results showed that the relation between age at menarche and obesity was more pronounced in women who were age at recruitment younger than 60 years, in the high education group, with no experience of breastfeeding, with a history of contraceptives, and with 0–1 parity. Whereas reproductive lifespan and age at menopause showed similar relations in subgroups, which was less stable in women who smoked and in those aged less than 60 years at recruitment.
Discussion
This was the first large study that comprehensively investigated the associations between age at menarche and menopause, reproductive lifespan, and risk of obesity in Chinese women, using a nationally representative sample and evaluating multiple subgroups. In this nationally representative study, 100,393 premenopause and 86,733 postmenopause women were included. We found age at menarche was significantly negatively related to the risk of obesity, and age at menopause and reproductive lifespan were significantly positively related to the risk of obesity.
Several studies found a correlation between age at menarche and adult obesity. 7,8 Liu et al. reported that the risk of obesity decreased with increasing age at menarche in southwestern Chinese women. 16 The risk of obesity was highest among women younger than 11 years of age at menarche, with an OR of 3.75, and lowest among women older than 18 years of age at menarche, with an OR of 0.74, which is consistent with the relation trend in Lenka’s study and our outcome in Supplementary Figure S1, especially in premenopause women. 16,17
Our study showed age at menarche was significantly and positively correlated with age at recruitment, with the mean age at recruitment reaching 59.7 years for women with age at menarche over 17 years and 44.3 years for women with age at menarche not over 13 years. This is related to the situation in China, where the People’s Republic of China was founded in 1949, and women born in the 1950s were more likely to suffer from poverty and malnutrition and to have their first menstruation later. Therefore, we are more concerned about the group of women who menstruate earlier; although the age is different, this is in fact related to the changes in the modern diet, and those who menstruate earlier may be at greater risk of obesity in middle age.
However, the mechanism of this relation is not well understood. One hypothesis is that an early age of menarche leads to higher concentrations of androgens in women, which in turn promotes obesity. 18 In addition, early onset of menarche has been linked to childhood obesity. 19 The rate of weight gain in childhood determines the age of puberty through the complex mechanism of leptin. 20 Excessive caloric intake and reduced physical activity in childhood may explain the early onset of menarche. 21 Moreover, obesity in childhood tends to track into adulthood and has a strong relation with metabolic syndrome in adulthood. 22
We found that age at menopause was related to obesity and that the risk increased significantly, especially after the age of 50, in line with the trend of the previous study. 8 Accelerated gains in fat mass and losses of lean mass are menopause transition-related phenomena. The rate of increase in the sum of fat mass and lean mass does not differ between premenopause and the menopause transition; thus, there is no discernable change in rate of weight gain at the start of the menopause transition. 23 During the menopause transition, there was a potential increase in insulin resistance, changes in serum lipid concentrations, and significant increases in BMI and percentage of total body fat. 24,25 The Copenhagen City Heart Study found that low plasma concentrations of endogenous estradiol had moderate adverse effects on cardiovascular risk factors, with the possibility that obesity was an intermediate factor. 26 For postmenopause women, the risk of all-cause mortality increases by 24% for every 5 kg/m2 increase in BMI, and this relation is reduced by appropriate physical activity. 27 Therefore, women with late menopause age can help prevent obesity through a low-caloric diet or Mediterranean diet and physical activity. 28
Reproductive lifespan is a composite indicator of age at menopause and age at menarche, and this study found that the risk of obesity increases as reproductive life increases. Xia C et al. reported that longer reproductive life was significantly related to a higher risk of central obesity and metabolic disease in Chinese women. 29 Longer reproductive lifespan can be considered as greater cumulative exposure to sex hormones and decreased High-Density Lipoprotein Cholesterol (HDL-C), which is associated with an increase in total and abdominal fat percentage and a decrease in HDL-C, to the detriment of CVD. 30
This study has some strengths. First, our study data were nationally representative using a multistage stratified sampling method, and our standardized measurement tools and strict quality control ensure credible and high-quality data. In addition, a number of factors (e.g., childhood obesity for which data were unavailable) that may influence obesity were adjusted to reduce the impact of potential confounding factors and reliably assess the relations. However, there are also some limitations. At first, this was a cross-sectional study, and therefore it was not possible to ascertain the causal association between age at menarche and menopause and obesity. Second, age at menarche and menopause were self-reported and subject to recall bias, leading to age group misclassifications possibly as well. Third, there are several reasons that women’s menses may cease, for example, hysterectomy, endocrine disorders, and cancer treatment, which may bring about a shift in the relationship between age at menopause and obesity as defined by BMI. And peri-menopausal stage has an effect on female body composition alone, which may partially influence the effect of age at menopause on obesity. Finally, menarche occurs at puberty, and obesity occurs in women after menopause, with a period of up to 30 years or more in between, making them susceptible to a variety of factors that can lead to a bias.
Conclusion
Based on the large nationally representative sample, Chinese women with earlier age at menarche, later age at menopause, and longer reproductive lifespan have higher risk of obesity. These associations also appeared to be similar among subgroups. Our results facilitate the early prevention of obesity in adolescence and alert and intervene in women whose menarche is earlier than 13 years and whose menopause is later than 51 years. Our findings have important public health implications for early detection and timely implementation of appropriate interventions in women at high risk of obesity.
Footnotes
Acknowledgments
The authors thank all the colleagues involved in the China Hypertension Survey.
Authors’ Contributions
L.C.: Conceptualization (supporting), writing—original draft (equal), formal analysis (lead), and writing—review and editing (equal). Y.H.: Writing—original draft (equal) and writing—review and editing (equal). X.W., C.Z., X.C., Z.H., J.C., L.Z., Y.T., and R.G.: Resources (equal). Z.W.: Conceptualization (lead) and writing—review and editing (equal).
Research Data (Data Sharing and Collaboration)
The dataset analyzed during the current study is available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
The study was supported by the Chinese Academy of Medical Science (CAMS) Innovation Fund for Medical Sciences (grant number 2017-I2M-1-004), the surveillance of cardiovascular disease and its risk factors in Chinese residents, and high-level hospital construction project (2022-GSP-GG-3).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.