
Abstract
Background:
Preeclampsia history signals a higher risk for cardiovascular disease, but its value as a risk marker relies primarily on self-report. To identify the accuracy of maternal self-reports of recent preeclampsia, we conducted a validation study among women recruited to a web-based trial.
Methods:
Women with preeclampsia in the past 5 years were recruited to Heart Health 4 Moms. Preeclampsia was self-reported through an online recruitment questionnaire and affirmed via phone screen. Accuracy of maternal self-report was quantified using positive predictive value (PPV) versus medical record evidence of preeclampsia using three definitions: (1) documentation of clinician diagnosis, (2) American College of Obstetricians and Gynecologists (ACOG) 2002 diagnostic criteria (gestational hypertension and proteinuria), and (3) ACOG 2013 diagnostic criteria (gestational hypertension and proteinuria or systemic symptoms).
Results:
Complete medical records were received for 290 women who delivered from 2011 to 2016 and were predominantly non-Hispanic White (81.7%) with a mean age of 31.2 ± 4.8 years. Mean length of recall was 13.6 ± 14.7 months. The majority of women (92.1%) had medical record evidence of preeclampsia using ≥1 of the definitions. Maternal self-report of preeclampsia was validated for 88.3% based on clinician diagnosis, 59.0% with ACOG 2002, and 65.2% with ACOG 2013.
Conclusions:
In this validation study of U.S. women, the majority accurately self-reported their preeclampsia diagnosis based on medical record review. A higher proportion of self-reports validated by clinician diagnosis than ACOG criteria, suggesting women remember the diagnosis given by their provider and providers may not always follow or document criteria when making a diagnosis.
Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality among women in the United States. 1 Adverse pregnancy outcomes (APOs), including preeclampsia, are associated with future maternal CVD risk factors and events. 2 –5 The American Heart and Stroke Associations recognize these complications as female-specific risk factors for CVD and encourage clinicians to obtain a detailed pregnancy history to identify patients with these conditions who are at increased risk for CVD. 6 –8 Preeclampsia—defined by new-onset hypertension with proteinuria or systemic symptoms after 20 weeks’ gestation—is one of the most common APOs, occurring in approximately 5% of all pregnancies, and is the APO most strongly and consistently linked to CVD. 4,6,9 –11 Given its occurrence early in a woman’s adult life, a preeclampsia history can help direct targeted prevention and screening efforts before the development of established CVD risk factors. However, in medical systems where obstetric records are not linked with primary care records, the value of preeclampsia as a risk marker for CVD in women relies upon the accuracy of maternal self-report.
The accuracy of maternal recall is dependent on correct communication of the diagnosis to the patient, the manner in which maternal self-report is ascertained, the quality of the gold standard, and the criteria applied to the gold standard (i.e., preeclampsia definition). In six previous validation studies that utilized medical records as the gold standard, the positive predictive value of maternal self-report of preeclampsia ranged from 50% to 89% with mean/median length of recall ranging from during pregnancy and/or 2 months after the estimated delivery date to 27 years. 12 –17 However, few studies have examined the accuracy of maternal recall of preeclampsia using the current American College of Obstetrics and Gynecology (ACOG) criteria first released in 2013, which expanded the previous definition of preeclampsia to include new-onset hypertension with systemic symptoms in the absence of proteinuria, and no study, to our knowledge, has compared the accuracy of maternal recall of preeclampsia across ACOG diagnostic criteria. 11,18,19
Therefore, we sought to assess the accuracy of maternal recall among those with a self-reported history of preeclampsia within the past 5 years who were recruited to a nationwide, randomized controlled trial of a web-based lifestyle intervention. 20 We validated and compared maternal self-report of preeclampsia against medical record evidence of clinician diagnosis, ACOG 2002 criteria, and ACOG 2013 criteria. 11,18
Material and Methods
Heart Health 4 Moms (HH4M) was a nationwide, randomized controlled trial, testing a web-based education and lifestyle intervention among women with a recent history (≤5 years) of preeclampsia, conducted in collaboration between Brigham and Women’s Hospital and the Preeclampsia Foundation (Clinical Trials.gov Identifier: NCT02147626). 20 Participants were recruited from July 2015 to May 2016 through various channels, including online and social media postings from the Preeclampsia Foundation (Facebook, Twitter, website, electronic newsletter), March of Dimes (Facebook, Twitter, website), Craigslist (website postings in 41 cities across 26 states to target underrepresented racial/ethnic groups and Spanish-language speakers), and BabyCenter (website postings within eligible Birth Club Forums based on month and year of delivery); through a partnership with the National Association of County and City Health Officials; and fliers posted in Women, Infants, and Children offices in Massachusetts. Recruitment materials provided potential participants with a link to an online eligibility survey, available in both English and Spanish. Study data were collected and managed using REDCap electronic data capture tools hosted at Mass General Brigham. 21,22 HH4M was approved by the Institutional Review Board of Mass General Brigham.
The HH4M recruitment survey collected demographic information and confirmed eligibility criteria: self-reported history of a pregnancy complicated by preeclampsia within the past 5 years, current age (18–44 years), U.S. residence, and live-born infant from the index preeclamptic pregnancy still residing with the participant. Women who developed preeclampsia after delivery (postpartum preeclampsia) were not eligible to participate in HH4M. If the participant was pregnant at the time of the survey, they provided a self-report of preeclampsia in response to the following question: “Has a doctor, midwife, or nurse told you that you have preeclampsia?” If a respondent was not currently pregnant but had delivered a baby in the past 5 years, they provided a self-report of preeclampsia in response to the following question: “Did a doctor, nurse or midwife tell you that you had preeclampsia?” Eligible participants were further screened over the phone by a trained research assistant to confirm the next level of eligibility criteria: normotension before the index preeclamptic pregnancy, not currently on an antihypertensive medication, weight less than 350 pounds, body mass index (BMI) between 18.5 and 40 kg/m2, access to the internet, and able to communicate in English or Spanish at least at an eighth-grade level. Respondents were also asked to affirm their history of preeclampsia by answering either the question “Did you develop preeclampsia during this pregnancy?” (if currently pregnant) or “Have you had a pregnancy complicated by preeclampsia in the last 5 years?” (if not currently pregnant). If a woman was pregnant at the time of the phone screen but was expected to deliver before the end of recruitment, she was re-contacted after her due date to complete the phone screen. In the case of more than one pregnancy complicated by preeclampsia within the last 5 years, women were first asked about the most recent preeclamptic pregnancy. If such a woman was ineligible based on her answers, she was then asked about her next most recent preeclamptic pregnancy in the past 5 years. Individuals with diabetes; a history of CVD, kidney disease, gastric bypass, or bowel surgery resulting in malabsorption; a current medical condition affecting diet or blood pressure (e.g., eating disorders, substance use disorder); or taking medications affecting their weight were not eligible. Women who remained eligible following the phone screen were asked to sign a medical record release form to allow study staff to obtain medical records related to the index preeclamptic pregnancy identified during the phone screen.
Medical records were requested to confirm the diagnosis of preeclampsia and included prenatal records, labor and delivery records, operative notes (in the case of a caesarian section), discharge summary of the delivery, and postpartum notes. As needed, study research assistants made repeated attempts to contact medical offices and/or hospitals to obtain complete medical records to either confirm or reject a preeclampsia diagnosis for the index pregnancy. Two clinician investigators (G.S. and E.S.) independently reviewed the records to validate the self-report of preeclampsia against three different definitions: (1) documentation of clinician diagnosis (i.e., whether a clinician [nurse, nurse midwife, nurse practitioner, or physician] wrote or similarly indicated [e.g., checking a box] in the medical record that the patient had “preeclampsia”), (2) ACOG 2002 diagnostic criteria, and (3) ACOG 2013 diagnostic criteria. Of note, “preeclampsia” mentioned in the medical record in the context of evaluation for, ruling out, or suspicion of preeclampsia did not qualify as documentation of clinician diagnosis of preeclampsia. Parity at the time of the first prenatal visit and the date of birth for the index pregnancy were also abstracted from the medical records.
A diagnosis of preeclampsia was confirmed by ACOG 2002 criteria if there was medical record evidence of: (1) new-onset hypertension (systolic blood pressure [SBP] ≥140 mmHg and/or diastolic blood pressure [DBP] ≥90 mmHg measured twice after 20 weeks of pregnancy in a woman with previously normal blood pressure) and (2) proteinuria (≥300 mg in a 24-hour urine collection, protein/creatinine ratio ≥0.3, or, if these two measures were not available, at least 1+ on a urine dipstick). 18 A diagnosis of preeclampsia was confirmed by ACOG 2013 criteria if the medical record for the index pregnancy satisfied the above criteria or, in the absence of proteinuria, new-onset hypertension was accompanied by new onset of any of the following systemic symptoms: thrombocytopenia (platelet count <100,000/μL), impaired liver function (abnormally elevated blood concentrations of liver enzymes to twice normal level, severe and persistent right upper quadrant or epigastric pain not responsive to medication nor accounted for by other diagnoses or both), new-onset or progressive renal insufficiency (serum creatinine concentrations >1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal diseases), pulmonary edema, or new-onset cerebral or visual symptoms (e.g., severe headache) after 20 weeks of pregnancy. 11 New-onset hypertension in pregnancy for both ACOG 2002 and 2013 criteria required confirmation of normotension before 20 weeks’ gestation, which was obtained by medical record evidence of no more than one elevated blood pressure during the first 20 weeks’ gestation (or a note endorsing normotension), the absence of a clinician diagnosis of chronic hypertension, and no evidence of anti-hypertensive treatment. Elevated blood pressures used to satisfy ACOG criteria were required to be at least 4 hours apart, except when blood pressure levels reached systolic blood pressure of 160 mmHg or higher and/or diastolic blood pressure of 110 mmHg or higher. In such cases, blood pressure measurements needed to be only a few minutes apart, per ACOG 2013 guidelines (whereas it was 6 hours apart in the ACOG 2002 guidelines). ACOG 2013 guidelines did not specify a required interval between documentation of elevated blood pressures and proteinuria and/or systemic symptoms; therefore, we conducted a sensitivity analysis requiring elevated blood pressures within one week of the proteinuria and/or systemic symptoms to mirror physician behavior in clinical practice.
For validation of maternal self-report of preeclampsia against ACOG 2002 or 2013 criteria, women were classified as having preeclampsia if there was medical record evidence satisfying the respective criteria for preeclampsia with either new-onset hypertension in pregnancy (as defined above) or preeclampsia superimposed on chronic hypertension. Preeclampsia superimposed on chronic hypertension according to ACOG 2002 was defined by (1) clinician diagnosis of chronic hypertension or documented anti-hypertension medication use or high blood pressure (SBP ≥140 mmHg and/or DBP ≥90 mmHg measured twice) before 20 weeks’ gestation; and (2) proteinuria (as defined above). Preeclampsia superimposed on chronic hypertension according to ACOG 2013, was defined in line with ACOG 2002 but additionally included women with chronic hypertension and systemic symptoms (as defined above).
Statistical analysis
Baseline demographic characteristics were summarized using means and standard deviations (SD), or percentages. Medical records from the index pregnancy served as the gold standard for validation. We compared the accuracy of maternal recall against clinician diagnosis in the medical record, ACOG 2002, and ACOG 2013 diagnostic criteria. For each of the three criteria, we calculated the positive predictive value (PPV), representing the proportion of maternal self-reports of preeclampsia that were accurate, according to the respective medical record evidence (clinician diagnosis, ACOG 2002, or ACOG 2013 diagnostic criteria). Analyses were conducted using SAS 9.4 (SAS Institute, Inc., Cary, NC).
Results
Over the 11-month recruitment period, 1,493 women completed the online recruitment survey. Of these, 931 women (62.4%) remained eligible following the survey, and 635 of them were subsequently phone-screened; 296 women were not phone-screened before the end of enrollment due to non-response following three follow-up attempts or because the enrollment target was reached. Following the phone screen, 390 women remained eligible, and 310 submitted a signed medical release form. Medical records were received for 300 women. Ten women had incomplete medical records, lacking sufficient information to either confirm or reject a diagnosis of preeclampsia (despite multiple requests for additional information), and were excluded. Therefore, medical records for 290 women were used to validate maternal self-report of preeclampsia. Index pregnancies were delivered from 2011 to 2016, with the majority (80.3%; n = 233) delivered from 2014 to 2016 (after the release of the ACOG 2013 guidelines).
Demographic characteristics of the population
The 290 women included in the validation study were predominantly non-Hispanic White (81.7%) and in their early thirties (31.2 ± 4.8 years; range: 20–44 years) at the time of recruitment into HH4M (Table 1). On average, they self-reported their history of preeclampsia 13.6 ± 14.7 months after delivery of the index pregnancy (range: 0–59.7 months), with the majority (63.8%) providing recall within the first year postpartum. Among those with known parity (n = 259, 89.3%), the majority were nulliparous (n = 185, 71.4%). At the time of recruitment, participants were living in 47 states across the U.S., with a plurality living in the South (n = 99, 34.3%).
Baseline Demographic Characteristics of the Heart Health 4 Moms Preeclampsia Validation Study Population (n = 290)
Parity (number of pregnancies lasting >20 weeks) was missing for 31 women while state/region was missing for one woman. SD, standard deviation.
Overall validation of preeclampsia
The majority of women (92.1%, n = 267) who self-reported preeclampsia had medical record evidence of preeclampsia according to at least one of the three definitions used in validation: clinician diagnosis, ACOG 2002, or ACOG 2013 diagnostic criteria (Fig. 1). Stratifying by time since delivery, women self-reporting preeclampsia within 12 months since delivery had a slightly higher overall PPV (93.5%) compared to those reporting from 12 months up to 5 years since delivery (89.5%).
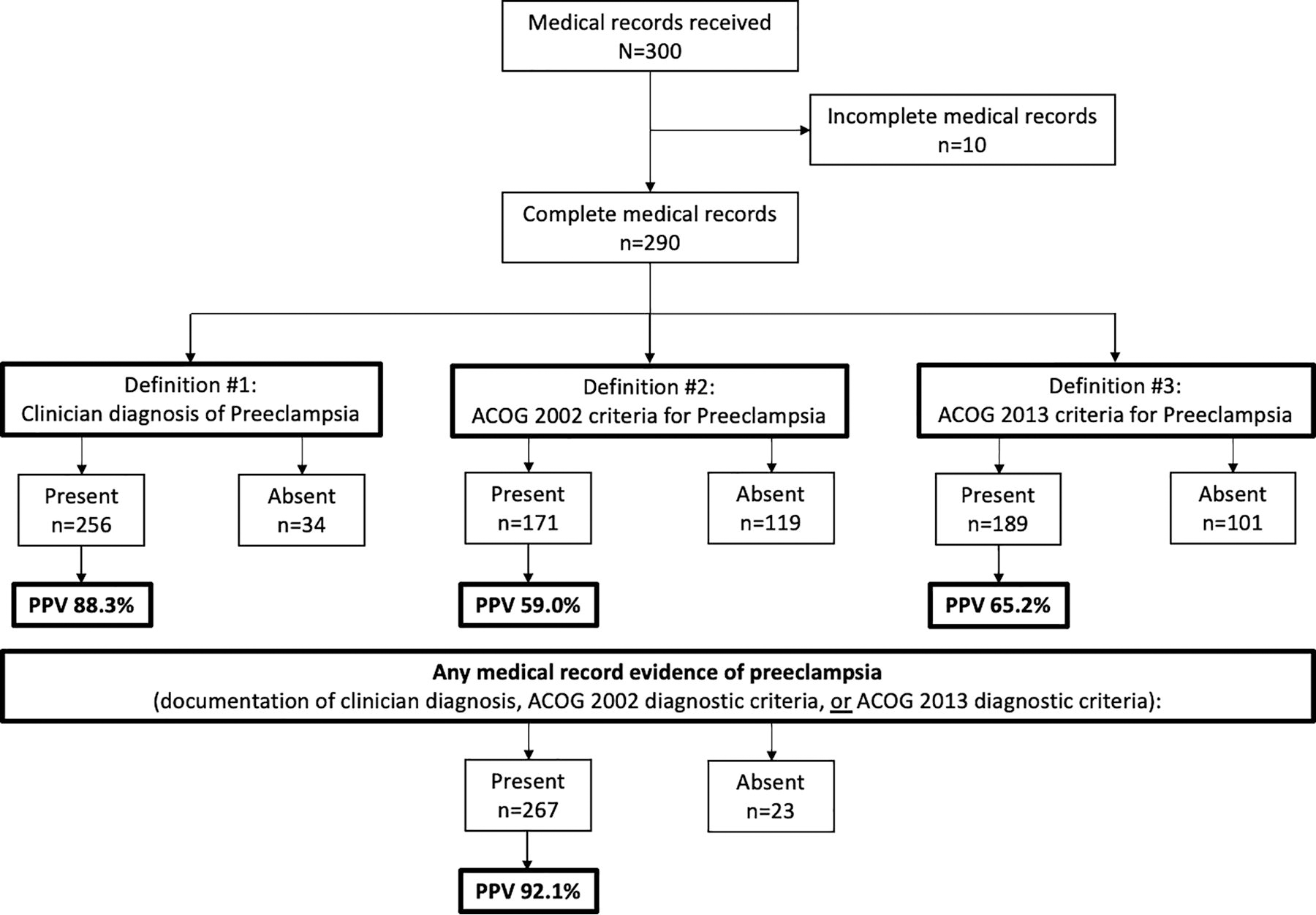
Flow diagram for the Heart Health 4 Moms (HH4M) medical record validation study of maternal self-report of preeclampsia. ACOG, American College of Obstetricians and Gynecologists; PPV, positive predictive value.
Validation of preeclampsia by clinician diagnosis
Out of the 290 medical records reviewed, a clinician diagnosis of preeclampsia was documented in medical records for 256 women, resulting in a PPV of 88.3% (Fig. 1).
For the 34 women who did not have a clinician diagnosis of preeclampsia in their medical records, 23 (67.6%) had the following related clinician diagnoses recorded: “pregnancy-induced hypertension” (PIH) or “gestational hypertension” (GHTN) (n = 14), Hemolysis Elevation of Liver enzyme and Low Platelets syndrome (HELLP) (n = 10; n = 5 women had both PIH/GHTN and HELLP), chronic hypertension (n = 3), and “hypertension during the third trimester of pregnancy” with “proteinuria during the third trimester of pregnancy” (n = 1). Among the remaining 11 women without clinician diagnosis of preeclampsia or a related diagnosis in the medical record, review of the record revealed a personal history of preeclampsia in a previous pregnancy (n = 5), two elevated blood pressures that were less than 4 hours apart (n = 1), only one elevated blood pressure (n = 2), documentation of “rule out preeclampsia” (n = 2), or no relevant signs or symptoms (n = 1).
Validation by ACOG 2002
The PPV of maternal self-report of preeclampsia was 59.0% (n = 171) when applying the ACOG 2002 diagnostic criteria to the 290 medical records (Fig. 1).
Women whose medical records did not validate against ACOG 2002 (n = 119) were slightly more likely to fail validation due to not meeting the hypertension criterion (n = 79) than the proteinuria criterion (n = 72; 32 did not meet either criterion). Among the 79 records that did not meet the hypertension criterion, 25 had no elevated blood pressures after 20 weeks’ gestation, 39 had only one elevated blood pressure after 20 weeks, and 15 had two elevated blood pressures after 20 weeks, but they were less than 4 hours apart.
Validation by ACOG 2013
When the ACOG 2013 diagnostic criteria were used, 189 women out of 290 had medical record evidence of preeclampsia for a PPV of 65.2% (Fig. 1). Among these women, 90.5% (n = 171) had hypertension with proteinuria, and 9.5% (n = 18) had hypertension with at least one systemic symptom in the absence of proteinuria (Fig. 2). Among the 18 participants meeting the ACOG 2013 criteria due to the presence of a systemic symptom, the most commonly occurring systemic symptom was impaired liver function (n = 10) followed by thrombocytopenia (n = 8), new-onset cerebral or visual disturbances (n = 6), and renal insufficiency (n = 3); none of the participants presented with pulmonary edema. Eight participants had more than one systemic symptom documented in their medical record (n = 7 had two symptoms and n = 1 had three). The most commonly co-occurring systemic symptoms were thrombocytopenia and impaired liver function, which presented in six of the eight participants with more than one systemic symptom.

Details of medical record confirmation of maternal self-report of preeclampsia by the ACOG 2013 diagnostic criteria. *The hypertension criterion for ACOG 2013 required new-onset hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg measured twice four hours apart) after 20 weeks of pregnancy in a woman with previously normal blood pressure. †Proteinuria was defined by ≥300 mg in a 24-hour urine collection, protein/creatinine ratio ≥0.3, or, if these two measures were not available, at least 1+ on a urine dipstick. ‡Systemic symptoms included thrombocytopenia (platelet count <100,000/μL), impaired liver function (abnormally elevated blood concentrations of liver enzymes to twice normal level, severe and persistent right upper quadrant or epigastric pain that is not responsive to medication nor accounted for by other diagnoses, or both), new-onset or progressive renal insufficiency (serum creatinine concentrations >1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal disease), pulmonary edema, or new-onset cerebral or visual symptoms (such as severe headache). § n = 8 participants had more than one systemic symptom documented in their medical record (n = 7 had two and n = 1 had three). # n = 12 participants who did not meet the ACOG 2013 criteria for preeclampsia were missing both qualifying elevated blood pressures and proteinuria/systemic symptoms. ACOG, American College of Obstetricians and Gynecologists.
The majority (n = 79) of the 101 women whose medical records were not validated by ACOG 2013 criteria did not meet the hypertension criterion. Of these, 39 had only one elevated blood pressure after 20 weeks, 16 did not have any elevated blood pressures after 20 weeks’ gestation, 15 had two elevated blood pressures after 20 weeks less than 4 hours apart, and 9 had elevated blood pressure(s) only during labor. A total of 34 participants did not have proteinuria or systemic symptoms; 12 participants did not meet either the hypertension criterion or the proteinuria or systemic symptoms criterion included in ACOG 2013.
Comparison of preeclampsia validation results across criteria
Among the 267 women with medical records confirmed preeclampsia, the majority validated according to all three criteria (Fig. 3). Specifically, 61% (n = 162) had a documented clinician diagnosis and evidence that satisfied both the ACOG 2002 and 2013 diagnostic criteria upon medical record review. Twenty-nine percent (n = 78) were validated according to clinician diagnosis but neither ACOG criteria. Nine women (3%) were validated by both ACOG 2002 and 2013 but lacked clinician diagnosis.
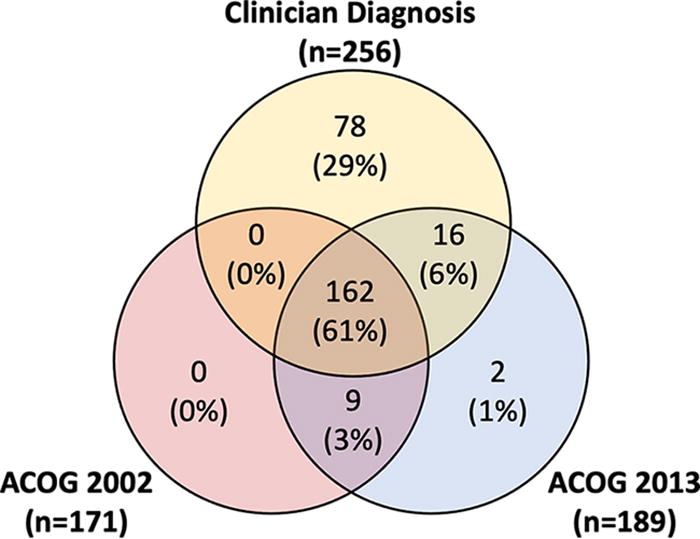
Validation results among the 267 women with medical record evidence of preeclampsia according to whether women were validated by clinician diagnosis, ACOG 2002, ACOG 2013, or a combination of the criteria. ACOG, American College of Obstetricians and Gynecologists.
Secondary analysis
In order to validate only preeclampsia with new-onset hypertension in pregnancy (rather than superimposed on chronic hypertension), a secondary analysis restricted to women with medical records confirmed normotension before 20 weeks’ gestation (n = 258; Supplementary Fig. S1). Among this subgroup, 91.5% (n = 236) had medical record evidence of preeclampsia.
Sensitivity analysis
To mirror clinician behavior in clinical practice, we conducted a sensitivity analysis requiring the elevated blood pressure criterion to be met within one week of the proteinuria/systemic symptoms criterion (Supplementary Fig. S2). The PPV of maternal self-report was 88.3% (n = 256) according to clinician diagnosis, 57.9% (n = 168) according to ACOG 2002, and 64.1% (n = 186) according to ACOG 2013.
Discussion
Over 90% of women self-reporting a recent history of preeclampsia had medical record evidence of preeclampsia satisfying one or more of the three definitions utilized in this validation study among 290 U.S. women recruited to a nationwide, randomized controlled trial of a web-based lifestyle intervention. The accuracy of maternal self-report of preeclampsia within the past 5 years was high against medical record evidence of clinician diagnosis and moderate against medical record evidence satisfying either the ACOG 2002 or ACOG 2013 diagnostic criteria. Accuracy of maternal self-report of preeclampsia was inversely related to the narrowness of the definition applied to the gold standard (medical records), with the highest PPV observed for clinician diagnosis (88.3%), followed by ACOG 2013 (65.2%) and ACOG 2002 (59.0%). To our knowledge, this is the first validation study comparing the PPV of maternal self-report of preeclampsia against the ACOG 2013 diagnostic criteria, which permitted the diagnosis of preeclampsia in the absence of proteinuria if other end organ symptoms were present, to that obtained with the ACOG 2002 criteria.
The PPV for ACOG 2013 diagnostic criteria exceeded that for ACOG 2002, as was expected given the wider range of qualifying signs and symptoms for preeclampsia diagnosis. Despite the fact that the majority of the included pregnancies were delivered after the release of the ACOG 2013 guidelines (i.e., 2014–2016), most preeclampsia cases met the diagnostic criteria with hypertension and proteinuria (90.5%) rather than with hypertension and at least one systemic symptom (9.5%). Given the anticipated lag between the release of new guidelines and subsequent uptake in clinical practice, the proportion of preeclampsia cases identified based on systemic symptoms, rather than proteinuria, may increase over time. Nonetheless, these findings suggest that the more expansive diagnostic criteria released by ACOG in 2013 permit the identification of an additional 1 in 10 preeclampsia cases.
The higher PPV observed for medical record evidence of clinician diagnosis of preeclampsia (88.3%), relative to either the ACOG 2002 or 2013 criteria, is likely reflective of (1) the complexity of the diagnostic criteria, requiring documented evidence across multiple time points in pregnancy, and (2) the severity of the condition. 23 In regard to the latter, the severity and quickly escalating nature of preeclampsia may mean that there may not always be time to measure and/or document the required vitals or labs when the life of the pregnant person and/or fetus are threatened, requiring emergent delivery. For these reasons, and since maternal recall is largely dependent on a provider informing the patient of their preeclampsia diagnosis, evaluating maternal self-report against medical record evidence of clinician diagnosis may best reflect the true accuracy of maternal self-report of preeclampsia.
The majority of extant medical record-based validation studies of maternal self-report of preeclampsia utilize the ACOG 2002 diagnostic criteria. The PPV of 59.0% obtained in the current study for ACOG 2002 is comparable to earlier studies in single centers (51.0% among 103 patients at Mayo Clinic in Rochester, MN with median recall of 27 years 14 ; 68.2% among 526 patients at Brigham and Women’s Hospital in Boston, MA with mean recall of 4.4 years 12 ) and population-based cohorts (57.0% among 4,300 Generation R Study participants in the Netherlands with a 2-month recall 13 ). Higher estimates have been obtained more recently from two population-based studies in Norway (sub-sample of participants in the fourth survey of the Tromsø Study) 17 and the Netherlands (PRIDE Study; prospective birth cohort), 16 which report PPVs of 80.0% and 88.0%, respectively. The higher PPV of 88.0% in the PRIDE Study may be due, at least in part, to the short length of recall (during pregnancy and/or 2 months after the estimated due date); 16 length of recall was not reported for the Tromsø Study (and was no longer available at the time of our request). One previous study has validated maternal recall of preeclampsia using ACOG 2013 diagnostic criteria and found a PPV of 97.7% (210/215; calculated based on data provided in Fig. 1). 19 Although higher than our PPV of 65.2%, this is likely the result of the selected nature of the previous study’s validation sample, which included participants in The Preeclampsia Registry and Biobank who self-reported a preeclamptic pregnancy within the past 7 years; did not have a pre-existing condition before pregnancy (chronic hypertension, diabetes, kidney or liver disease, idiopathic thrombocytopenia, or other hematologic disorders); provided a saliva sample; and for whom medical records were available.
When medical record evidence of preeclampsia according to one or more of the three definitions used in the current validation (clinician diagnosis, ACOG 2002, or ACOG 2013 diagnostic criteria) was accepted, the PPV was 92.1%; this can be most directly compared with a validation study conducted in the Nurses’ Health Study II prospective cohort. In that study, the PPV of nurse participants self-report of “preeclampsia/toxemia” on biennial questionnaires was 89% when accepting medical record evidence of either (1) provider report of preeclampsia or (2) documentation of gestational hypertension and proteinuria (ACOG 2002), either written/checkboxed or measured blood pressure and urine protein. 15
It is worth noting that, even when applying a more inclusive definition to the medical records, the quality of maternal recall is inherently limited by the accuracy of the information communicated at the time of diagnosis. Providing patients with an accurate, succinct, and understandable clinical summary following a maternal event (e.g., APO diagnosis) may both increase clarity in provider-patient communication and aid in maternal recall. This could take the form of a physical checklist handout that could be completed by the provider and given to the patient at the time of diagnosis and/or delivery of hospitalization discharge.
Strengths of this study include rigorous medical record review to confirm the presence or absence of preeclampsia according to three different definitions/diagnostic criteria and geographic representation of participants from 47 U.S. states. However, while the current study is comparable to past validation studies of maternal self-report of preeclampsia in regard to majority non-Hispanic White race and ethnicity, and nulliparity, the accuracy of maternal self-report may differ in more diverse patient samples. Selection bias may limit the interpretation of our findings, as those included in this validation had at least an eighth-grade reading level, were not on anti-hypertensive medication, and responded to outreach for a lifestyle intervention study; therefore, these individuals may have been more aware of their preeclampsia history and more likely to be engaged in health-seeking behaviors than the general population of preeclampsia patients. Furthermore, preeclampsia history was self-reported on the recruitment questionnaire and subsequently confirmed upon phone screen, which likely increased the accuracy of maternal self-report relative to a single self-report. Finally, postpartum preeclampsia was not systematically assessed in this medical record validation study; records were available through discharge for all participants but medical records up to six weeks postpartum were not uniformly collected. This may have resulted in an attenuation of the PPV, as individuals with true postpartum preeclampsia may have accurately self-reported having had preeclampsia, but the medical records necessary to validate the diagnosis were not available.
A self-reported history of preeclampsia identifies individuals at an increased risk for future CVD risk factors and events. 4,15 In the absence of medical record linkages bridging the gap between prenatal and obstetrical care to primary care, an individual’s ability to accurately report their preeclampsia diagnosis is critical to ensuring they receive appropriate care. This validation study demonstrated that over 90% of those self-reporting recent preeclampsia had medical record evidence of preeclampsia diagnosis or diagnostic criteria. Accurate identification of those with a history of preeclampsia has the potential to improve public health through continued investigation of the short- and long-term consequences of this adverse pregnancy outcome and to improve individual health through appropriate screening, referral, and prevention strategies to reduce cardiovascular risk.
Authorship Contributions
J.S.: conceptualization, methodology, software, formal analysis, investigation, data curation, writing—original draft. G.S.: conceptualization, investigation, project administration, writing—review and editing. A.R.: writing—review and editing. E.T.: writing—review & editing. J.R.-E.: funding acquisition, methodology, conceptualization, writing—review and editing. E.S.: supervision, funding acquisition, methodology, conceptualization, investigation, writing—review and editing. All authors contributed to and approved the final version of the article.
Footnotes
Author Disclosure Statement
J.J.S. is now a salaried employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, United States. No other competing financial interests exist.
Funding Information
Heart Health 4 Moms was funded by the Patient Centered Outcomes Research Institute Contract CER-1306–02603. J.J.S. was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number K01HL159281; the content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.