
Abstract
Background:
Nearly half of all pregnancies in the United States are considered unintended (mistimed or unwanted), and this rate is even higher among younger and lower income women. The Affordable Care Act (ACA) dependent coverage provision may have influenced the frequency of unintended pregnancies by increasing accessibility to and affordability of family planning services among young adults. Furthermore, the impact of this provision may differ by young adult income level as those with lower income are less likely to be insured and thus more likely to benefit from this provision. Our objective was to estimate the association between the ACA dependent coverage provision and unintended pregnancy, overall, and by young adult income level.
Methods:
We applied a difference-in-differences approach to data from multiple cycles of the National Survey of Family Growth (n = 10,104) and compared trends in unintended pregnancy between those who were eligible to benefit (ages 18–25 years) and those who were ineligible to benefit (ages 26–33 years) from the provision, overall, and among income subgroups.
Results:
We found evidence that the dependent coverage provision was associated with a −7.4 percentage point reduction (95% CI: −13.5, −1.3) in the prevalence of unintended pregnancy among young adults with lower income (<100% of the federal poverty level). There was limited evidence, however, that the provision was associated with unintended pregnancy among young adults with higher income levels.
Conclusions:
These findings suggest the ACA dependent coverage provision may have reduced unintended pregnancy among a particularly high-risk group (i.e., young adults with lower income).
Introduction
Each year, roughly 5% of women aged 15–44 years experience a pregnancy that they consider to be either mistimed or unwanted, and this figure is nearly twice as high among women under the age of 30. 1 –3 These pregnancies are commonly referred to as “unintended.” 1 –4 Unintended pregnancy is an important public health issue because it is an indication that people are experiencing pregnancies—major health and life events—that they consider to be poorly timed or unwanted. Unintended pregnancy is influenced by numerous social, political, and economic factors, 1,5 –12 including public policy that shapes accessibility and affordability of family planning services.
The Patient Protection and Affordable Care Act (ACA) is one such policy that plausibly affected access to family planning. The dependent coverage provision of the ACA required private insurance plans to cover an insured’s dependents up to the age of 26 years. 13,14 This provision may have reduced insurance-related barriers to contraceptive products and services among young adults by increasing access to insurance coverage through parental coverage. In fact, there is evidence that the dependent coverage provision increased the number of young adults with health insurance coverage. 15,16 There is also evidence that this provision was associated with an increase in the use of highly effective hormonal contraceptives like the contraceptive shot and implant, 17 a reduction in the abortion rate, 17 and a reduction in childbearing. 17,18 Importantly, however, impacts on contraceptive use may be limited to certain sociodemographic subgroups. 16 Less research has assessed whether these changes in insurance coverage and contraceptive use translated into fewer unintended pregnancies. Moreover, despite the potential for impacts to differ by young adult and parental socioeconomic status due to differences in private health insurance coverage prior to the ACA, 19 –21 few studies have investigated whether the impact of the dependent coverage provision on reproductive health differed by young adult or parental socioeconomic status. 16 –18
Our objective was to determine whether the ACA dependent coverage provision was associated with a decrease in the prevalence of unintended pregnancy among young adult females. Further, we evaluated whether this potential association differed by one indicator of socioeconomic status (i.e., young adult income level). This work is relevant for both public health and public policy because it provides evidence of the impact of the dependent coverage provision on unintended pregnancy among young adult females overall as well as among socioeconomic subgroups, thereby improving our collective understanding of the impact of contemporary healthcare reform on reproductive health and health equity.
Materials and Methods
Design, data, and study population
We used a repeated cross-sectional study design, using data from multiple cycles of the National Survey of Family Growth (NSFG). 22 The NSFG is a cross-sectional survey of noninstitutionalized civilian males and females aged 15–44 years who are selected using a multistage probabilistic sampling methodology. Survey participants are asked about marriage, divorce, family life, fertility, and family planning. By applying NSFG-provided survey weights, nationally representative estimates can be produced. We used NSFG data from the 2006–2010, 2011–2013, and 2013–2015 survey cycles and included female respondents aged 18–33 who reported being sexually active (n = 10,929). We excluded respondents who turned 26 during the recall period in which the exposure and outcome were being measured (n = 822), and respondents who were missing covariate information (n = 3). These restrictions resulted in an analytic sample of n = 10,104 respondents (Fig. 1).
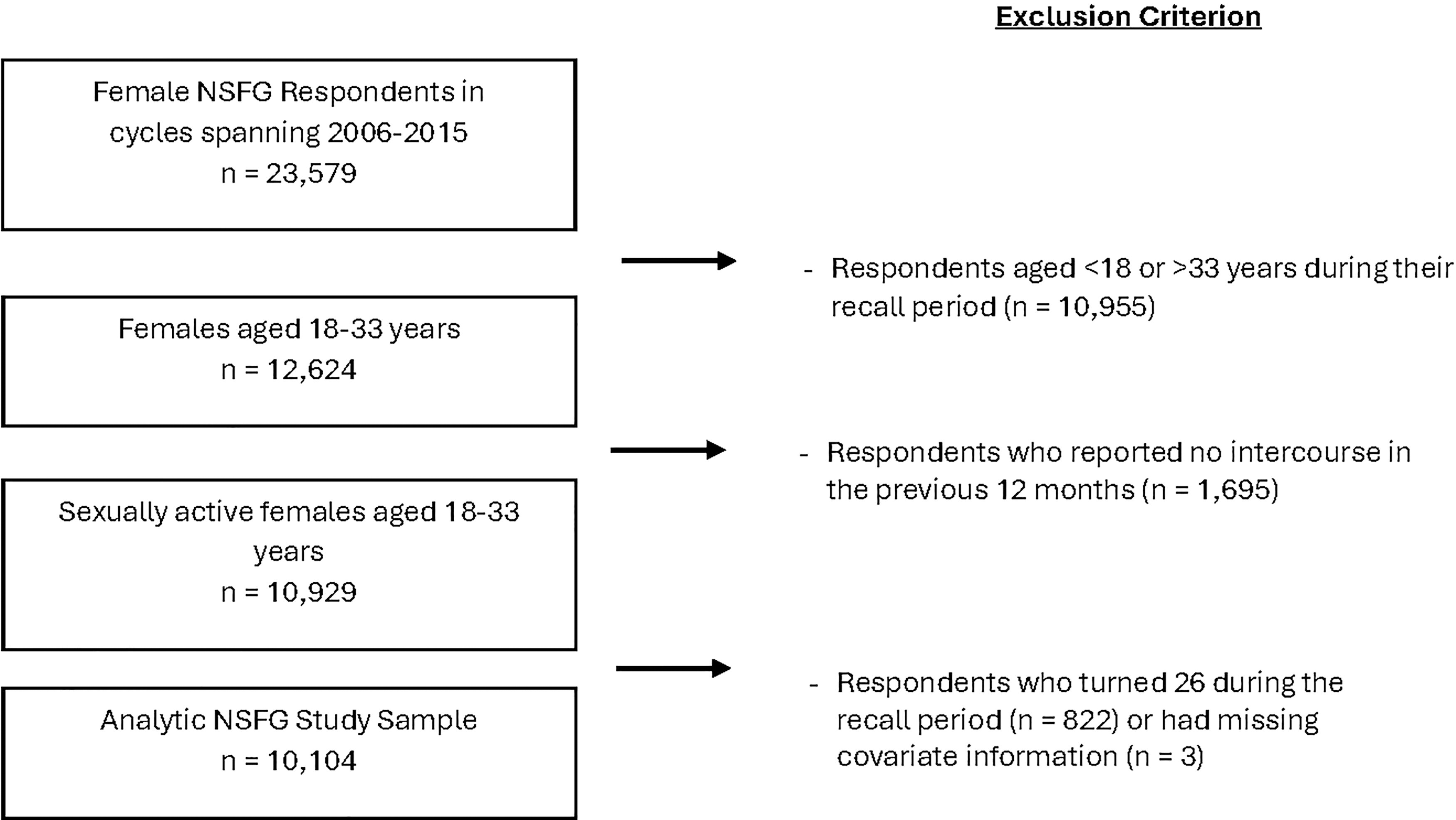
Flowchart for the unweighted analytic sample of sexually active female respondents ages 18–33 from the National Survey of Family Growth (NSFG).
Measurement of outcomes
We measured unintended pregnancy using a binary indicator of whether the respondent experienced at least one unintended pregnancy in the calendar year prior to being surveyed (e.g., if interviewed in 2013, we considered pregnancies that occurred in 2012). The NSFG attempts to collect a full pregnancy history for each respondent. As part of this history, the NSFG gathers information regarding both timing and wantedness of each pregnancy. This information, along with year of conception and respondent interview date, allowed us to identify unintended pregnancies that occurred in the prior calendar year.
Measurement of exposure
We also measured exposure to the dependent coverage provision in the calendar year prior to survey (hereafter, referred to as the recall period). The dependent coverage provision was implemented in September 2010 and required that private insurance plans cover dependents up to the age of 26 years. If an individual was eligible to benefit from the dependent coverage provision based on their age, we considered that individual to be “exposed” to the provision. Therefore, we considered an NSFG respondent to be exposed to the provision if they were aged 18–25 years for the entire recall period. Respondents aged 26–33 during the recall period were considered unexposed. We excluded respondents who turned 26 during the recall period (n = 822) because these individuals would have become ineligible to benefit from the dependent coverage provision during the recall period. That is, they would have been age eligible to benefit for part of the recall period, but not the entire recall period.
Measurement of covariates
We included several covariates that have been found to be correlated with unintended pregnancy: race/ethnicity [Hispanic, non-Hispanic (NH) Black, NH other or multiple races, NH White], household income level [<100% of the Federal Poverty Level (FPL), 100–249% of the FPL, 250–399% of the FPL, ≥400% of the FPL], education level (less than a bachelor’s degree and currently attending school, less than a bachelor’s degree and not currently attending school, bachelor’s degree or more), marital status (married, not married), parity (nulliparous, primiparous, multiparous), nativity (born in the United States and born outside of the United States), and metropolitan residence (yes, no). All covariates were collected primarily through self-report.
Statistical analyses
We summarized sample characteristics using frequencies and weighted percentages. Then, we described trends in unintended pregnancy graphically, depicting the trend overall and by exposure status. To evaluate the impact of the dependent coverage provision, we used a difference-in-differences (DD) approach. This approach identifies the impact of an intervention by comparing the trend in an outcome over time between an exposed group and an unexposed group. The validity of this approach requires that we assume the trend of the potential outcome from pre- to post-intervention would have been the same for both groups in the absence of the intervention. 23 –25 This is known as the parallel—or common—trends assumption. If the trend from pre- to post-intervention would have been the same for both groups in the absence of the intervention, then any difference in trends can be attributed to the intervention. Although this assumption cannot be verified, we can assess the plausibility of this assumption by looking at trends in the pre-intervention period. If pre-intervention trends do not differ between exposed and unexposed groups, the required assumption may be plausible. If pre-intervention trends do differ between groups, it suggests that the required assumption is likely not plausible.In this work, we assess the plausibility of the parallel trends assumption using visual assessment and hypothesis testing to evaluate whether pre-intervention trends differ between the exposed and unexposed groups.
We implemented the DD approach using a linear probability regression model. Both unadjusted and adjusted models were considered. Adjusted models included respondent household income level, race/ethnicity, education level, marital status, parity, and metropolitan residence. In our DD analysis, we defined a single post-policy period spanning 2010–2014, which combined data from two NSFG survey cycles. Then, we used an event study analysis to disaggregate this post period into two time points (2010–2012 and 2012–2014). The model specification that we employed can be found in Supplementary Appendix SA1. Through both DD and event study analyses, we estimated the change in prevalence of unintended pregnancy—i.e., the prevalence difference—that was associated with the dependent coverage provision.
In addition, we conducted subgroup analyses by the household income level (<100% of the FPL, 100–249% of the FPL, 250–399% of the FPL, and ≥400% of the FPL). To clarify whose income is captured by this measure, we restricted our subgroup analyses to respondents who reported not living with a parent. By incorporating this restriction, the operationalized household income measure reflects that of the young adult (rather than their parents). We conducted subgroup analyses to explore possible effect modification by income and to increase the plausibility of the common trend assumption by restricting the included sample based on one indicator of socioeconomic status (income level).
Sensitivity analyses
We also conducted sensitivity analyses to assess the robustness of our primary results with respect to the age range used to define exposure and to explore effect modification by age group. In these analyses, we restricted our definition of the unexposed group to include only those aged 26–29 during the recall period and considered two alternative definitions for the exposed group: 1) we considered respondents ages 18–21 during their recall period to be exposed and 2) we considered respondents ages 22–25 during their recall period to be exposed.
Statistical software
All analyses were conducted using Stata/SE 18.0. Svy commands were used along with the subpop statement to apply sampling weights and account for the multistage sampling methodology of the NSFG. Using these commands, we applied the Taylor linearization method to calculate standard errors.
IRB review
This study was reviewed and approved by the Michigan State University Institutional Review Board (STUDY0005077).
Results
Sample characteristics
Table 1 provides a summary of sample characteristics overall and stratified by exposure status and period. Most respondents identified as NH White (57.7%), reported a household income below 250% of the FPL (58.9%), had completed less than a bachelor’s degree (74.0%), were not married (59.4%), and lived in a metropolitan area (81.8%) (Table 1). Just under half (48.2%) of the study sample was age-eligible to benefit from (i.e., “exposed” to) the dependent coverage provision (Table 1). A greater proportion of the exposed group had lower income, less education, were not married, and were nulliparous (Table 1), which reflects their younger age. Overall, 6.1% of respondents reported experiencing at least one unintended pregnancy in the prior calendar year. This percentage decreased over the study period for both exposed and unexposed groups [9.2% to 7.5% among the exposed group and 4.3% to 3.8% among the unexposed group].
Sample Characteristics, Overall and Stratified by Period and Exposure Status, for the NSFG Analytic Sample of Sexually Active Female Respondents Aged 18–33 (n = 10,104)
NH, Non-Hispanic; FPL, Federal Poverty Level; Unweighted frequency and weighted percentages reported.
Primary analysis
To investigate the plausibility of the common trend assumption, we visually assessed whether the unadjusted pre-intervention trends appeared parallel, and we used statistical tests to formally evaluate whether unadjusted and adjusted pre-intervention trends differed by exposure status. The visual assessment revealed unadjusted pre-intervention trends that appeared roughly parallel for most income groups, although there was a notable exception among respondents with incomes between 100–249% of the FPL (Fig. 2). The statistical tests, however, suggested that the unadjusted and adjusted trends did not differ between exposed and unexposed groups prior to intervention (Supplementary Appendix SA2 Table B1, estimates for “2005–2007” from the event study analysis). Although these tests do not verify a common trend, they show no statistically detectable violation of this assumption in a period prior to the ACA. Given that the visual assessment and statistical test results were mixed regarding the 100–249% FPL income group, caution may be warranted when interpreting results among this income group.
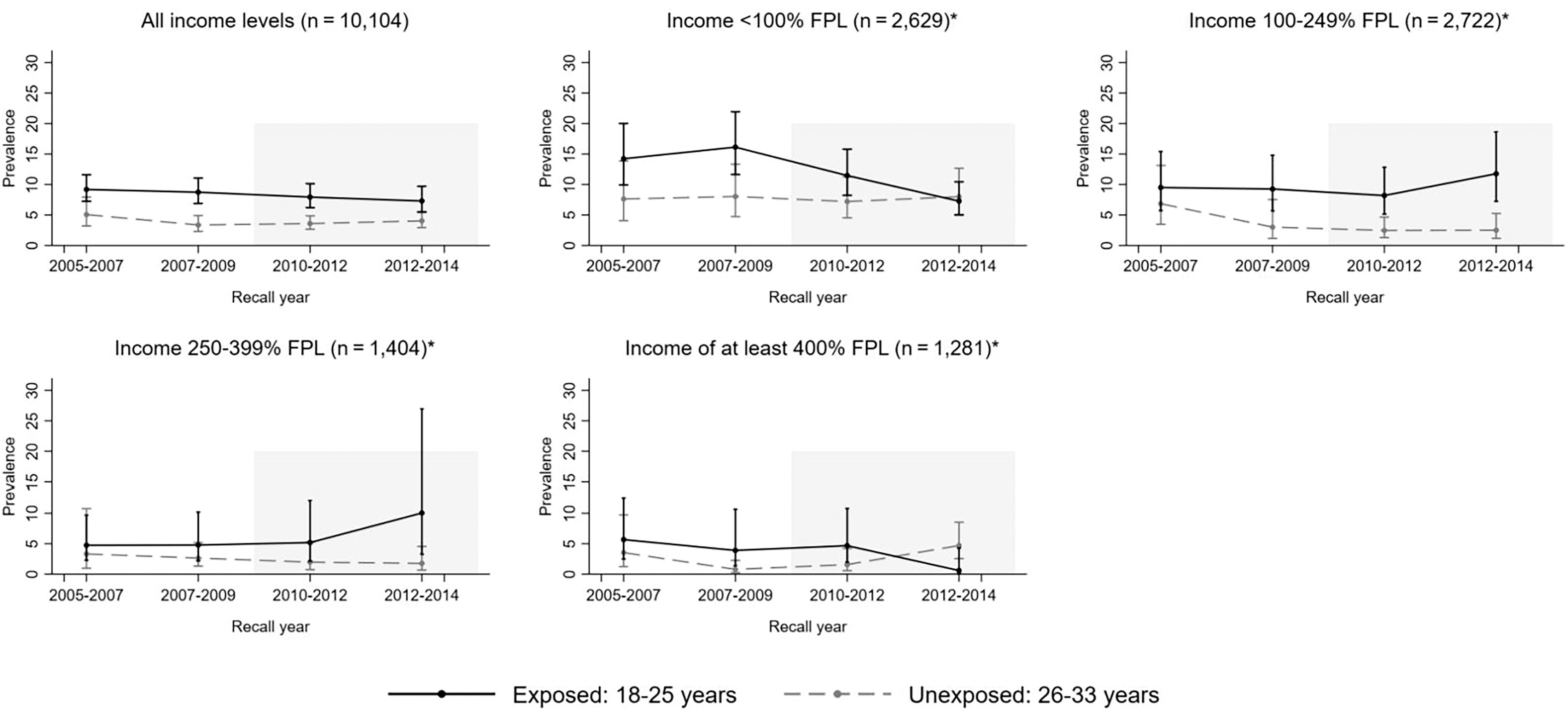
Trends in the unadjusted prevalence of unintended pregnancy over the study period, by exposure status and income level based on the NSFG analytic sample of sexually active female respondents aged 18–33 (n = 10,104). *To improve clarity of the income measure, we include only respondents who reported no parents in their household.
The unadjusted and adjusted DD and event study analyses provided no evidence that the dependent coverage provision was associated with prevalence of unintended pregnancy among 18–25-year-old females when all income levels were combined (Table 2, Supplementary Appendix SA2 Table B1). Among the lowest income group (<100% of the FPL), however, the adjusted estimate suggested that the dependent coverage provision was associated with a −7.4 ppt (95% CI: −13.5, −1.3) decrease in the prevalence of unintended pregnancy in 2010–2014 among young adult females (Table 2). Estimates from the event study analysis further suggested this association increased over the study period (Fig. 3, Supplementary Appendix SA2 Table B1). For example, in 2010–2012, the adjusted estimates suggested that the dependent coverage provision was associated with a statistically nonsignificant −5.0 ppt (95% CI: −13.6, 3.6) decrease in the prevalence of unintended pregnancy among young adult females with incomes <100% of the FPL, and this estimate increased to −9.0 ppt (95% CI: −17.0, −1.0) in 2012–2014. There was no evidence that the dependent coverage provision was associated with a reduction in unintended pregnancy among young adult females with incomes between 100 and 399% of the FPL (Table 2, Fig. 3, Supplementary Appendix SA2 Table B1), but there was some evidence from the event study analysis that the dependent coverage provision was associated with a −5.8 ppt (95% CI: −10.8, −0.7) decrease in the prevalence of unintended pregnancy among young adult females with incomes ≥400% of the FPL in 2012–2014 only (Supplementary Appendix SA2 Table B1).

Adjusted prevalence difference estimates for the association between the ACA dependent coverage provision and unintended pregnancy, as estimated by the event study analysis using the National Survey of Family Growth (NSFG) analytic sample of sexually active female respondents aged 18–33 (n = 10,104). ACA, Affordable Care Act; FPL, Federal poverty level. Estimates from the event study analysis, indicated by the point markers on the plot, provide an estimate of the prevalence difference in unintended pregnancy associated with the dependent coverage provision, given in percentage points. Bars extending from the point markers indicate 95% confidence intervals. The adjusted model includes respondent’s race/ethnicity, income level, education level, marital status, parity, nativity, and metropolitan residence. *To improve clarity of the income measure, we include only respondents who reported no parents in their household.
Prevalence Difference Estimates for the Association Between the ACA Dependent Coverage Provision and Unintended Pregnancy, as Estimated by the Difference-in-Differences Analysis Using the NSFG Analytic Sample of Sexually Active Female Respondents Aged 18–33 (n = 10,104)
Bold estimates indicate statistical significance at the 5% significance level.
To improve clarity of the income measure, we include only respondents who reported no parents in their household.
Includes respondent’s race/ethnicity, income level, education level, marital status, parity, nativity, and metropolitan residence.
ACA, Affordable Care Act; DD, Difference-in-differences; FPL, Federal Poverty Level; NSFG, National Survey of Family Growth; PD, Prevalence Difference; CI, Confidence interval.
Sensitivity analysis
When restricting the DD analyses to 22–29-year-olds (exposed: 22–25, unexposed: 26–29), the dependent coverage provision was associated with a decrease in unintended pregnancy among both the lowest income group and the highest income group, suggesting results among the highest income group are sensitive to the age range specification (Supplementary Appendix SA2 Table B2). Further, we found that associational estimates were generally larger among the older age group (ages 22–25) than the younger age group (ages 18–21) (Supplementary Appendix SA2 Tables B2–B3).
Discussion
Using a nationally representative sample of young adult females, we found evidence that the ACA dependent coverage provision was associated with a 7 ppt reduction in the prevalence of unintended pregnancy among women aged 18–25 with a household income <100% of the FPL. This result represents a 40% decrease from the pre-intervention prevalence among this group. We found limited evidence, however, that the dependent coverage provision was associated with prevalence of unintended pregnancy among women aged 18–25 with incomes at or above 100% of the FPL or when all income groups were combined. These findings suggest the dependent coverage provision may have reduced unintended pregnancy and that this impact may have differed across socioeconomic subgroups of young adults.
Importantly, the results of our event study analyses further suggested that the decrease in unintended pregnancy associated with the dependent coverage provision was largest in 2012–2014 and may have extended to the both the lowest (<100% of the FPL) and highest (≥400% of the FPL) income groups during this period. These results may suggest that the impact of the dependent coverage provision increased over the post period, reflecting a lag period between the implementation and impact of the dependent coverage provision for these income groups. Alternatively, the timing of these associations (2012–2014) aligns with the implementation of the ACA preventive care mandate which required that insurance plans cover preventive care, including FDA-approved female contraceptives. 14 This mandate applies to nongrandfathered, nonexempt insurance plans for individuals of all ages. If the impact of this mandate was equal across age groups, then our estimates for 2012–2014 should isolate the impact of the dependent coverage provision. However, if the impact of the mandate differed by age group, then our estimates for this period could be capturing a joint effect of the dependent coverage provision and the preventive care mandate, which could also explain the larger associations that we observed in 2012–2014 for the lowest and highest income groups. If so, these findings may suggest that both the dependent coverage provision and the preventive care mandate influenced unintended pregnancy among the lowest income group (consistent with the negative and growing point estimates we observed in 2010–2012 and 2012–2014), but that only the preventive care mandate influenced unintended pregnancy among the highest income group (consistent with the small, insignificant positive estimate we observed in 2010–2012 and the significant negative estimate we observed in 2012–2014). It is somewhat of a puzzle, however, that no statistically significant associations were observed among young adults with incomes between 100–399% of the FPL. Null results throughout the post period may suggest that neither the dependent coverage provision nor contraceptive mandate were able to effectively reach these middle-income groups, or were unable to influence sexual behaviors (e.g., contraception use or choice) among these groups. However, when stratified by income level, the event study analyses suffer from relatively small period- and group-specific sample sizes coupled with an outcome that becomes increasingly rare as income increases. As such, findings from the event study analyses could also be the result of sampling variation or relatively low statistical power, particularly among higher income groups. Additional work is needed to confirm these findings and investigate potential contributing mechanisms.
Our primary findings are consistent with previous descriptive work that found the unintended pregnancy rate declined between 2008 and 2011 among younger (18–24 years) and lower income (<100% of the FPL) women, 2 previous research that suggests fertility among young adults decreased following enactment of the dependent coverage provision, 17,18 and previous research that suggested abortions may have decreased among young adults following the dependent coverage provision. 17 These findings are also consistent with prior studies that found the use of highly effective contraceptives [long-acting reversible contraceptives (LARCs), contraceptive implant, contraceptive shot] increased in young adults after the dependent coverage provision was enacted. 17,26 Furthermore, the results of our subgroup analyses align with previous work that suggested impacts of the dependent coverage provision may differ across sociodemographic subgroups. 16,20 For example, the dependent coverage provision was associated with a roughly 10 ppt (43%) increase in dependent coverage (i.e., health insurance coverage through a parent’s plan), and these impacts were larger among young adults with indicators of lower socioeconomic status (i.e., unmarried, nonstudents). 20 Similarly, the dependent coverage provision was associated with a 13.5 ppt increase in the percent of Hispanic young adults who received a birth control method or prescription but was not associated with receiving a birth control method or prescription among NH Black or NH White young adults. 16 We are unaware, however, of prior research estimating the impact of the dependent coverage provision on unintended pregnancy or related outcomes (e.g., changes in insurance, contraception use) by young adult income level. Thus, it is difficult to assess with confidence whether the magnitude of our observed associations is plausible based on current literature.
This study has a few limitations. First, the analysis had relatively low statistical precision (or power), as indicated by the width of the confidence intervals reported. This suggests that caution should be exercised when drawing conclusions regarding the magnitude of the impact. Second, the estimates produced rely on the assumption that the exposed and unexposed groups would experience the same trend in unintended pregnancy in the absence of the intervention (i.e., the dependent coverage provision). Our empirical evaluation of this assumption in the pre-intervention period revealed no detectable violation, but it is important to emphasize that this assumption cannot be verified, and our empirical evaluation was limited to two pre-intervention time points. Furthermore, our hypothesis tests for differences in trends in the pre-intervention period may be underpowered. 27 To reduce the possibility for residual confounding, we incorporated restriction by age and income level (i.e., conducting sensitivity analyses further restricting the age range of the exposed and unexposed groups, conducting subgroup analyses stratified by income level) and regression adjustment. Third, the use of household income as a measure of socioeconomic status for young adults is limited by the fact that many young adults are still financially dependent on their parents and may be in the midst of educational or training pursuits that will eventually increase their earning potential. However, by restricting our subgroup analyses to young adults who reported not living with a parent, the operationalized income measure should reflect the household income of the young adult (not their parents), thereby indicating the young adult’s level of need for material support from external sources like parents. Fourth, this is an intention-to-treat analysis. That is, exposure was defined by respondent’s age without information on availability or use of parental health insurance coverage. We could not restrict our analyses to young adults who have parents with private insurance coverage because the NSFG does not collect data on parents’ insurance coverage. Thus, these analyses allowed us to evaluate the impact of the dependent coverage provision among the age group that was intended to benefit. It does not, however, differentiate between those who were eligible to benefit from those who did benefit.
We must also note the inherent complexity in conceptualizing and measuring pregnancy intention. First, we did not have adequate sample size to disaggregate unintended pregnancy and evaluate its two components separately (mistimed and unwanted pregnancy). Second, we used a retrospective measure of unintended pregnancy which may be susceptible to recall bias, although previous research is mixed regarding the extent of this potential bias. 28 –30 Moreover, because we are interested in estimating the difference in unintended pregnancy trends, we would only expect this measure to bias our associational estimates if its impact differed over time between the exposed and unexposed groups. Beyond its potential for recall bias, the construct validity of this measure has also been debated. In short, the construct validity has been questioned because a retrospective dichotomous measure of pregnancy intention cannot capture the complexity of an individual’s pregnancy desires nor can it capture the economic, social, political, or historical context of these desires or experiences. 5 –8,10,11 Acknowledging these issues, we believe that unintended pregnancy remains an important reproductive health outcome because it indicates that people are experiencing pregnancies that they themselves consider to be mistimed or unwanted, thereby suggesting that more can be done to support individual pregnancy and fertility desires.
Despite these limitations, this research also offers important contributions. This is the first study of which we are aware that estimates the impact of the ACA dependent coverage provision on unintended pregnancy, overall, and within income subgroups. These findings thus contribute to understanding both how the ACA influences health and for whom. Furthermore, this study used a nationally representative sample which increases external validity, and a DD approach which reduces the potential for confounding by incorporating a comparison (“unexposed”) group. Moreover, by incorporating multiple NSFG survey cycles in the post-intervention period, this approach provides information on the timing of the impact and allows the impact to change over the post-intervention period.
Future contributions can build upon this study in at least three ways. First, larger and more diverse datasets are needed to increase estimate precision and allow for additional subgroup analyses (e.g., analyses by race/ethnicity). Second, additional data are needed to understand the interaction between parental and young adult socioeconomic status, along with its implications for health equity. This need is reflected in both prior work that finds variation in parental insurance coverage (and subsequently, potential for dependents to benefit from the provision) by sociodemographic characteristics like income level, 31 as well as in the findings from our subgroup analyses that found the magnitude of the observed association between the dependent coverage provision and unintended pregnancy differed by the young adult income level. Third, additional studies are needed to confirm these findings and examine potential causal pathways within socioeconomic subgroups of young adults (e.g., changes in sexual behaviors, contraceptive choice, consistency of contraceptive use).
Conclusion
We found evidence that the ACA dependent coverage provision was associated with a substantial reduction in the prevalence of unintended pregnancy among young adult females with low income (i.e., females aged 18–25 who had a household income <100% of the FPL) in 2010–2014, but there was little evidence of an association among young adults with higher incomes. These findings suggest that the dependent coverage provision may have reduced unintended pregnancy, but that this impact may have been limited to certain socioeconomic subgroups. This work provides important information regarding one provision of the ACA, and how it has succeeded (or failed) to influence reproductive health among socioeconomic subgroups. More work is needed to understand how this provision, and the ACA more broadly, has influenced reproductive and sexual health, and health equity.
Footnotes
Authors' Contributions
C.L.M.-B.: conceptualization, methodology, analysis, writing—original draft, writing—review and editing, project administration, and funding acquisition; R.K., Z.L., C.H., and T.A.B.: methodology and writing—review and editing; C.E.M. (senior author): conceptualization, methodology, writing— review and editing, supervision, and funding acquisition.
Data Availability Statement
Author Disclosure Statement
The authors declare that they have no known or competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.