
Abstract
Objectives:
We aimed to describe obstetrics and gynecology (OBGYN) trainees’ anticipation of how the Dobbs v. Jackson Women’s Health Organization (Dobbs) U.S. Supreme Court decision may affect their training.
Methods:
A REDCap survey of OBGYN residents and fellows in the United States from September 19, 2022, to December 1, 2022, queried trainees’ anticipated achievement of relevant Accreditation Council for Graduate Medical Education (ACGME) training milestones, their concerns about the ability to provide care and concern about legal repercussions during training, and the importance of OBGYN competence in managing certain clinical situations for residency graduates. The primary outcome was an ACGME program trainee feeling uncertain or unable to obtain the highest level queried for a relevant ACGME milestone, including experiencing 20 abortion procedures in residency.
Results:
We received 469 eligible responses; the primary outcome was endorsed by 157 respondents (33.5%). After correction for confounders, significant predictors of the primary outcome were state environment (aOR = 3.94 for pending abortion restrictions; aOR = 2.71 for current abortion restrictions), trainee type (aOR = 0.21 for fellow vs. resident), and a present or past Ryan Training Program in residency (aOR = 0.55). Although the vast majority of trainees believed managing relevant clinical situations are key to OBGYN competence, 10%–30% of trainees believed they would have to stop providing the standard of care in clinical situations during training.
Conclusions:
This survey of OBGYN trainees indicates higher uncertainty about achieving ACGME milestones and procedural competency in clinical situations potentially affected by the Dobbs decision in states with legal restrictions on abortion.
Introduction
On June 24, 2022, the US Supreme Court released their opinion in Dobbs v. Jackson Women’s Health Organization (Dobbs) that overturned federal protection of access to abortion from Roe v. Wade. 1 States and organizations attempted to navigate the existing laws and regulations that could impact reproductive care. 2 Obstetrics and gynecology (OBGYN) professionals faced uncertainty, not only about providing clinical care to women but also the impact on the training and competency of OBGYN physicians. 3 The American College of Obstetricians and Gynecologists (ACOG) 4 and the Society of Gynecologic Surgeons (SGS) 5 have expressed concern about the emerging future of OBGYN after the Dobbs decision, given that 44% of residency programs are located in states where access to abortion may be restricted. 6
The Accreditation Council for Graduate Medical Education (ACGME) establishes educational milestones for all accredited residency programs. These milestones are used for resident and fellow outcomes-based assessments and include six general competencies. 7,8 Both the ACGME and ACOG state that adequate training of OBGYN residents requires appropriate education in family planning and abortion to ensure women’s safe access to termination of pregnancy. 8,9 Prior studies have shown that residents with routine abortion care training feel more satisfied with their training, are more competent, and are more likely to provide all aspects of miscarriage care, a foundational skillset for all OBGYNs, even those in states that ban nearly all abortion. 10,11 This indicates that the perception of anticipated OBGYN training may be altered after the Dobbs decision, but there are limited data from the trainee perspective.
Our objective was to survey OBGYN residents and fellows about the possible effect of the Dobbs decision on their OBGYN training in the post-Dobbs legislative environment. We hypothesized that trainees would anticipate more training gaps in states where laws restricting abortion care were already in place or pending.
Materials and Methods
We conducted a cross-sectional survey of OBGYN trainees from all residency and most fellowship programs in the United States between September 19, 2022, and December 1, 2022. The University of New Mexico Human Research Review Committee deemed the study exempt.
We designed this survey using the ACGME milestones as applicable to abortion care. 8 The survey was piloted by the study group (n = 20) and invited participants (n = 10) across the country prior to dissemination. The final survey instrument contained a mixture of multiple-choice or binary responses as well as free-answer questions (Supplementary Data S2). We then emailed all OBGYN residency and fellowship program directors and program coordinators in the United States, asking them to forward the REDCap survey link to their trainees. 12,13 We also contacted the Ryan Residency Training Program and fellowship society listservs for dissemination of the survey link. Finally, advertisements with REDCap survey links were posted on social media and through personal contacts at various institutions.
Our primary outcome was resident or fellow uncertainty about obtaining the highest chosen ACGME milestone level queried (Level 3 or 4) in all sub-competencies potentially affected by the Dobbs decision. Additionally, we sought to determine how many residents would meet the minimum 20 abortion procedures required by the OBGYN Residency Review Committee prior to graduation. Sub-competences potentially affected by Dobbs included any in which the ACGME referenced medical or procedural management involving embryos or fetuses, whether or not the specific milestone was explicitly related to abortion care.(Supplementary Data S1) Most questions had response options of “I’m not sure” or “Uncertain.” Responses were often followed by software logic–generated, multiple-choice questions to elucidate the respondents’ rationale.
We collected trainee information including postgraduate year (PGY), presence of a Ryan Residency Training Program at their current or former residency, and, for fellows, their fellowship subspecialty. We queried participant beliefs about whether they could continue to provide the standard of care and/or would be concerned about facing legal charges for managing clinical situations potentially affected by Dobbs during training and in future practice, for example, early pregnancy loss, pregnancy of unknown location, ectopic pregnancy, molar pregnancy, assisted reproductive technologies involving stored embryos, or medication and procedural induced abortion in the first or second trimesters for differing indications. We queried if trainees planned to access abortion-related training outside their own training program. Finally, we asked their beliefs about whether the ability to manage these clinical scenarios is vital in competency after graduation from an OBGYN residency and if they planned to manage these situations after training. The full survey instrument is available as a supplementary document (Supplementary Data S2).
We performed univariate analyses to establish respondent characteristics associated with the primary outcome. We then performed logistic regression analysis, adjusting for confounders identified in the univariate analyses using JMP 9.0.0 (SAS Institute Inc, Cary NC). For univariate and logistic regression, we considered the training location by state to be in the categories of unrestricted (minimal to no restrictions on abortion care), pending restrictions (laws in place to restrict that had yet to be voted upon or approved), and restricted (laws already in place in that state) according to the New York Times tracker for restrictions on the date of analysis (December 18, 2022). 14
Descriptive statistical analyses using Excel software were performed regarding respondents’ beliefs about the clinical scenarios related to the Dobbs decision, and descriptive statistical analyses were also performed on respondents’ plans for seeking training outside their home program.
Results
Of the 594 survey responses, 469 were active trainees in OBGYN programs (330 residents and 139 fellows) and eligible for analysis (Fig. 1). We received 469 eligible responses; the response rate could not be calculated as we purposefully did not query how many contacted programs sent it to which trainees in order to protect respondent anonymity. Of respondents, 197 (42%) of them were in states with pending restrictions (41 residents and 12 fellows in 6 states) or with current restrictions (96 residents and 48 fellows in 15 states) at the time of the survey. PGY levels were well distributed among resident respondents: 60/328 (18.3%) PGY 1, 83/328 (25.3%) PGY 2, 95/328 (29.0%) PGY3, and 90/328 (27.4%) PGY4. Fellow respondents included 37 (26.6%) in Maternal–Fetal Medicine (MFM), 36 (25.9%) in Gynecologic Oncology (Gyn Onc), 20 (14.4%) in Female Pelvic Medicine and Reconstructive Surgery (FPMRS), 16 (11.5%) in Reproductive Endocrinology and Infertility (REI), 14 (10.1%) in Complex Family Planning (CFP), 10 (7.2%) in Minimally Invasive Gynecologic Surgery (MIGS), 1 (0.7%) in Pediatric and Adolescent Gynecology (PAG), and 5 (3.6%) in other fellowships (including Global Health, Women’s Health Research, Women’s Reproductive Health, and Global Health Equity). Respondents varied in geography, with the most participants training in Pennsylvania, New York, and California (Fig. 1).

Recruitment of respondents into the study and respondent characteristics and locations.
Of resident respondents, 238/328 (72.6%) were affiliated with a Ryan Training Program, and 103/139 (74.1%) fellows had a Ryan Training Program at their former residency. Residency training at a program with a Ryan Training Program was not associated with plans to fully or partially participate in family planning training (OR 1.325, 95% CI 0.858–2.047).
The primary outcome, uncertainty of obtaining the highest queried milestone levels or the prerequisite 20 abortion procedures, was reported in 33.5% (157/469; 95% CI 29.4%–37.9%) of respondents (138 residents and 19 fellows). Occurrence of the primary outcome was well distributed by residency year (28 PGY1, 37 PGY2, 41 PGY3, 31 PGY4, 1 no response to PGY query). Among fellows, the primary outcome was seen across all ACGME fellowship subspecialties (12 MFM, 4 CFP, 2 REI, 1 FPMRS). On univariate analyses, factors significantly associated with the primary outcome included trainee type (13.7% fellows vs. 41.8% residents, p < 0.01), state environment (42.4% restrictions vs. 58.5% pending restrictions vs. 23.8% unrestricted, p < 0.01), PGY level (p < 0.01), and Ryan Training exposure (29.3% with Ryan Training vs. 44.8% without, p < 0.01). Participation in family planning training (no/partial participation vs. full participation) was not significantly associated with the primary outcome (p = 0.12). When adjusting for trainee type (resident vs. fellow), PGY level was no longer significantly associated with the outcome, so it was not included in the logistic regression model. State environment, trainee type (resident or fellow status), and Ryan exposure were included in the model. All three factors remained as significant predictors of the primary outcome after adjusting for the others. Restrictive state environments increased primary outcome incidence (aOR = 3.94 for pending restrictions vs. unrestricted, 95% CI 2.04–7.77, and aOR = 2.71 for restrictions vs. unrestricted, 95% CI 1.71–4.33), whereas having more senior trainee status (aOR = 0.21 for fellow vs. resident, 95% CI 0.12–0.35) and a present or past Ryan Training Program in residency (aOR = 0.55, 95% CI 0.34–0.88) were protective.
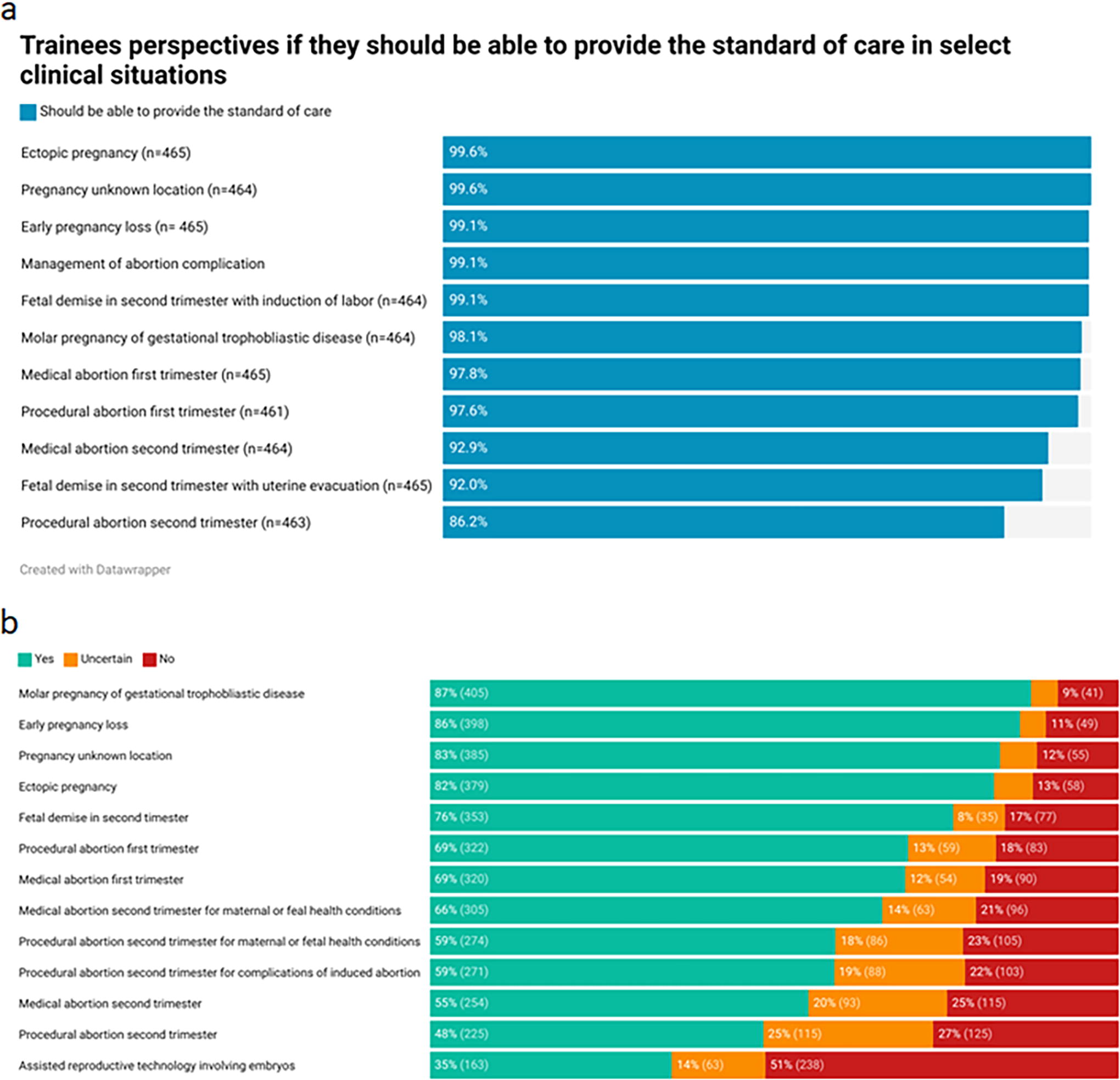
The majority of respondents replied that a competent OBGYN residency graduate should be able to offer the standard of care in most of the areas queried, including management of pregnancy loss, ectopic pregnancy, and termination of pregnancy for a variety of indications (Fig. 2a), and 86.2% believe second-trimester procedure abortion is key for competency in OBGYN (Fig. 2a). The majority of trainees also plan to manage clinical scenarios involving first-trimester pregnancy loss and nonviable pregnancy after graduation and to provide first-trimester services in induced abortion (Fig. 2b). Of trainee respondents, 48% (56% of residents and 34% of fellows) plan to offer second-trimester abortion procedures for any indication in their future practice.
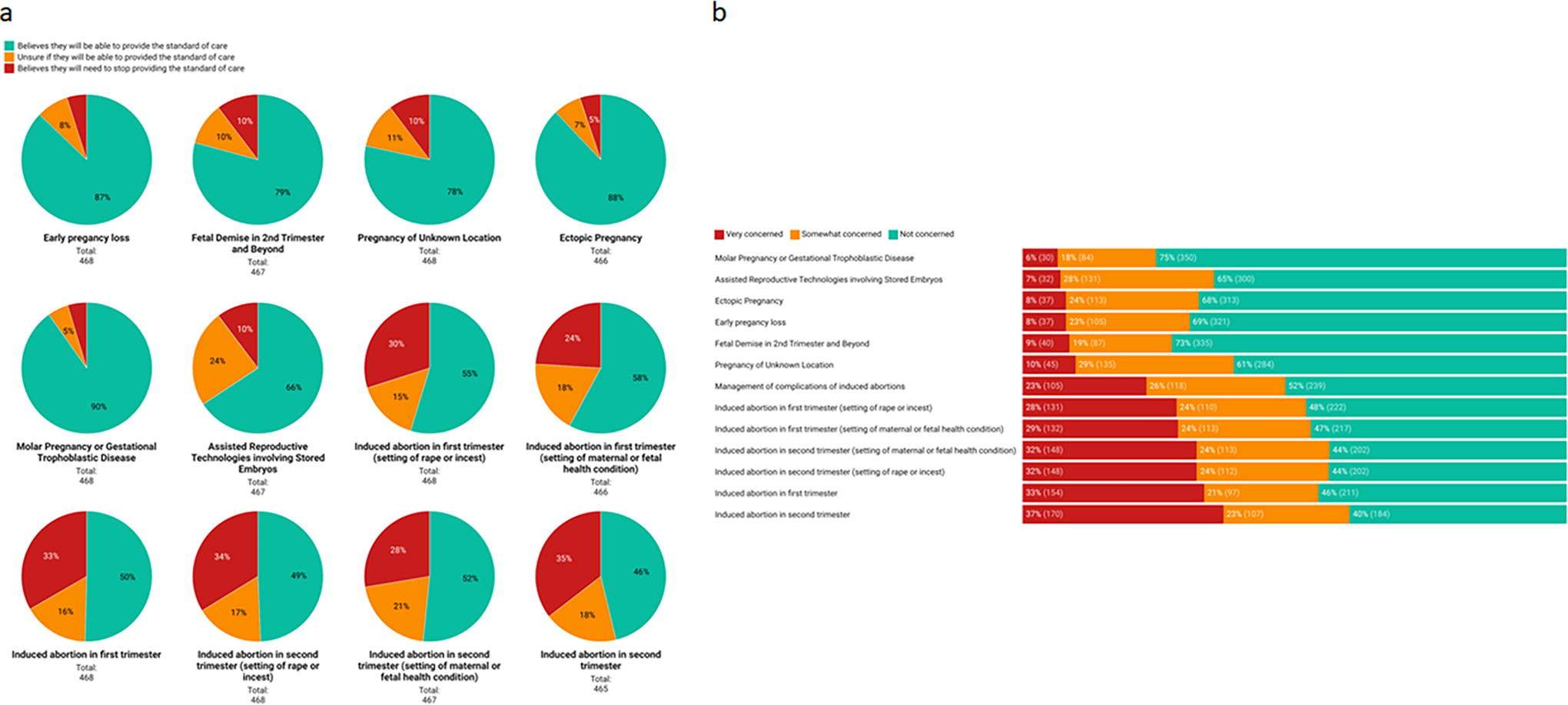
Ten percent of trainees believed they would have to stop providing the standard of care in cases of pregnancy of unknown location and assisted reproductive technologies, and 33% believed they would have to stop providing the standard of care for induced abortion (Fig. 3a). At least 24% of trainees were at least somewhat concerned about facing legal charges because of providing care during training, with the situation where this concern was the lowest being gestational trophoblastic disease and the highest in second-trimester abortion (Fig. 3b).
The majority of resident respondents felt they had already obtained Level 3 milestones in first-trimester bleeding (74.2%), family planning (72%), laparoscopic surgery (58.6%), and consultations (73.9%). However, of residents that had not obtained Level 3 milestones in these areas, up to a third (32.5%) did not think they would achieve this during residency (Fig. 4). Among the 75% of residents who had not achieved Level 4 in family planning, 33.6% were uncertain in their ability to obtain these skills, and 13.9% felt they would not obtain them prior to graduation (Fig. 4). Although 64.8% (197/304) of residents had already completed the 20 abortion procedures required by the ACGME, 26/107 (24.3%) who had not were uncertain or did not think they would prior to graduation (Fig. 4).

Resident reporting of obtainment of ACGME milestones and expected obtainment of these milestones if not already competent at this level. ACGME, Accreditation Council for Graduate Medical Education.
Fellow trainees from ACGME programs (CFP, MFM, REI, FPMRS, and Gyn Onc) expressed some uncertainty about whether they would obtain Level 3 or Level 4 subspecialty milestones relevant to their field (Supplementary Fig. S1). This was noted in the CFP fellows’ milestones of Level 3 management of complex abnormal pregnancy (20%), Level 3 serving as a consultant (33.3%), and Level 4 physician role in health care systems (50%). Many non-CFP fellows also expressed uncertainty in obtaining milestones such as Level 3 of genetic principles of the gamete/embryo for REI fellows (25%), Level 3 of sonographic and diagnostic procedures in MFM fellows (46.7%), and Level 3 of prenatal imaging and diagnosis in MFM fellows (11.1%).
Some respondents (9.3%) expressed they intended to seek experience outside of their program in family planning (Supplementary Fig. S2), 61% of which were willing to travel to an outside city or state to get this experience (Supplementary Fig. S3). Fortunately, the most common reasons expressed by trainees for not seeking outside training were already feeling competent in relevant milestones (75.2%) (Supplementary Fig. S4).
Conclusions
This survey of OBGYN residents and fellows indicates significant uncertainty regarding their ability to achieve ACGME milestones, reach procedural competency, and provide vital reproductive care to patients, because of the Dobbs U.S. Supreme Court decision. This uncertainty was increased with location in states with restricted or pending restrictions on abortion, resident status (vs. fellow status), and decreased with exposure to a present or past Ryan Training Family Planning program in residency or fellowship training.
Our study adds current postgraduate trainees’ perspectives to prior studies that documented decreased interest in postgraduate medical training in states with restrictive laws. Although past data have implied trainee concern about achieving competency in states with pending or current restrictions on reproductive health, these data add nuance by measuring, through objective ACGME milestones, which competencies trainees are concerned about lacking post-training. The AAMC reported greater decreases in the number of U.S. MD applicants in states with complete abortion bans across all specialties, not just OBGYN in 2023, compared with 2022. 15 Another survey that included US medical students and international medical graduates applying to US residency programs, residents, fellows, and practicing physicians across all specialties demonstrated that the majority (82%) preferred to work or train in states with preserved abortion access. 16 However, this is the first national study to examine current residents’ or fellows’ concerns nationally about reaching competencies deemed necessary for practice. Their concerns may exacerbate the decline in residency applications to states with restrictive laws; more importantly, they demonstrate lack of confidence in graduating as competent general or subspecialized OBGYNs.
There have been various published commentaries and opinion pieces focused on the broad anticipated impacts of abortion access and provision among medical providers and trainees. 17 –19 Authors have highlighted that lack of abortion training will also negatively impact achieving competency and developing skills in miscarriage management, pregnancy options counseling, and reproductive healthcare beyond abortion provision. 20 Our results document trainee-level data of these anticipated impacts. Stakeholders should consider that established training programs with high clinical volume and expertise (Ryan Programs) may positively affect trainees’ perceived competency in this area of OBGYN practice.
There are inherent limitations to survey studies that are reflected here. The findings reflect a respondent bias in that the survey was voluntary, and residents who have strong opinions about the Dobbs decision may be more likely to participate in the study. To mitigate this risk, the authors made specific efforts to eliminate any language in the survey wording that could suggest a bias for or against the Dobbs decision. Additionally, the authors made efforts to reach out to OBGYN organizations with both pro-life and pro-choice philosophies to broaden the reach of the survey distribution as much as possible. Despite these efforts, it is not possible to accurately quantify the total denominator of survey distribution or calculate an accurate response rate, as we did not query the program or the identity of respondents or those it reached to protect anonymity, and we were not permitted to distribute the survey directly to trainees. The response rate of only 330 out of over 1600 residents limits understanding the generalizability of the results. There is also no way to account for the possibility of social desirability bias that may be present in a survey study design.
Lastly, we must acknowledge some possible limitations of the survey and the outcomes themselves. There is no validated instrument available to measure trainee opinions specific to this situation, so we composed and piloted this instrument as quickly as possible to generate the data in a timely fashion, but key questions could have been unasked. For example, we purposefully did not query trainee characteristics such as age, gender identity, or racial identity in this survey because we wanted to keep focus on their training outlook and avoid actual or perceived politicization of their personal characteristics, and we wanted to avoid any perception that they could not remain completely anonymous. A lack of query in trainee characteristics resulted in our inability to describe or analyze these factors in these data. Also, certain fellowship subspecialties either do not have ACGME milestones (MIGS, PAG) or have limited milestones relevant to early pregnancy or abnormal pregnancy care (such as FPMRS or Gyn Onc), so this calls into question the contribution of these fellows to the survey. Our primary outcome and other questions only reflect trainee opinion, and it will be years before studies on this topic can determine if trainees predictions in this survey are proven or disproven in future objective measures of competency and preparedness in training graduates. However, we do not want to imply that uncertainty or fear among trainees is not itself concerning or damaging to the profession. Some reports have indicated drops in OBGYN applications to residencies in states with abortion bans, 21 indicating the possibility for trainee perceptions to alter the field.
We would support research on the same topic in 2–3 years’ time to observe any lasting impact on training. Such work would aid OBGYN training programs and national organizations in program design, program requirements, and workforce planning. This would also support the lawmakers that face complex decisions affecting medicine in our modern times, such as decisions about mifepristone prescribing, contraception coverage, and other issues related to this Supreme Court decision.
This study offers some of the first descriptive data after the Dobbs decision from a trainee viewpoint, demonstrating risk factors and protective factors for feeling uncertainty about future competency in training.
Footnotes
Acknowledgments
The authors would like to acknowledge the Collaborative Research in Pelvic Surgery Consortium (CoRPS) of the Society of Gynecologic Surgeons for providing administrative support for this study. The authors also want to thank the Ryan Program and Dr. Jodi Steinauer and Kristen Simonson for providing contacts and support for survey editing and distribution and the Society of Gynecologic Oncology for providing contacts and support for survey distribution.
Author Contribution
K.V.M.: Conceptualization, supervision, project administration, methodology, investigation, data curation, writing—original draft. S.K.-F.: Conceptualization, project administration, investigation, data curation, writing—original draft. T.A.: Conceptualization, investigation, data curation, writing—original draft. A.O.: Methodology, investigation, data curation, writing—original draft. L.E.D.: Methodology, investigation, data curation, writing—original draft. J.W.K.: Methodology, investigation, data curation, writing—original draft. W.D.W.: Methodology, visualization, data curation, writing—original draft. F.O.: Methodology, data curation, writing—original draft. D.M.: Methodology, data curation, writing—original draft. C.L.G.: Conceptualization, methodology, data curation, writing—original draft. A.J.B.: Methodology, data curation, writing—review and editing. K. P.: Methodology, data curation, writing—review and editing. M.E.F.-R.: Methodology, data curation, writing—review and editing. J.K.T.: Methodology, data curation, writing—review and editing. O.H.C.: Methodology, data curation, writing—review and editing. S.H.: Methodology, data curation, writing—review and editing. S.T.R.: Methodology, data curation, writing—review and editing. C.C.C.: Methodology, data curation, writing—review and editing. T.R.P.: Formal analyses, writing—review and editing. C.B.I.: Conceptualization, methodology, data analyses, writing—review and editing.
Author Disclosure Statement
K.V.M. is a board member-at-large for the Society of Gynecologic Surgeons, for which she receives travel support and holds a voting board position, and editor for Elsevier Publishing, for which she receives royalties, and a paid consultant for RBI Medical. A.O. is the President of the Association of Professors and Gynecology and Obstetrics. C.L.G. is the Research Chair for the Society of Gynecologic Surgeons, for which she receives travel support and holds a voting board position. S.H. is a Nexplanon trainer for Organon. C.B.I. is the 49th President of the Society of Gynecologic Surgeons, for which she receives travel support and has a voting board position. The other authors have no conflicting interests to disclose.