
Abstract
Introduction:
Endocrine therapy (ET) is the cornerstone of systemic treatment for patients with estrogen receptor positive breast cancer, but its uptake and adherence need further improvement. This observational study assessed ET initiation and 1-year adherence and its survival benefit among female Medicare beneficiaries with early-stage breast cancer.
Materials and Methods:
This retrospective cohort study analyzed the linked 2011–2019 Surveillance, Epidemiology, and End Results-Medicare data. Female beneficiaries newly diagnosed with hormone receptor positive, stage I-III breast cancer were included. Beneficiaries who initiated tamoxifen, anastrozole, letrozole, or exemestane within 3 months after cancer diagnosis were defined as initiators (n = 24,289), and those who never initiated these treatments were noninitiators (n = 8,899). Adherence was measured using proportion of days covered (PDC) in the continuous 12 months follow-up period. Multivariable logistic regression models were used to assess factors associated with ET initiation and adherence (PDC ≥ 80%), controlling for covariates. Weighted Cox proportional hazard models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) of all-cause and breast cancer related mortality between initiators and noninitiators and by adherence status.
Results:
Among eligible female beneficiaries (n = 55,893), 43% initiated ET within 3 months of cancer diagnosis. Among initiators, 77% had PDC ≥ 80% during the first year. Patient’s demographics (e.g., older age, race/ethnicity) and baseline health services utilization (e.g., mammography) were associated with ET initiation and adherence. ET initiation and adherence was associated with reduced risk of all-cause (adjusted HR = 0.62, 0.59–0.66; HR = 0.55, 0.53–0.59; respectively) and breast cancer related (adjusted HR = 0.57, 0.50–0.64; HR = 0.41, 0.36–0.47; respectively) mortality compared with noninitiators.
Conclusion:
Women with early-stage breast cancer who initiate ET and are adherent to treatment may achieve survival benefits compared with noninitiators.
Introduction
Breast cancer is the most common cancer in American women, except for skin cancers. 1 In 2023 alone, there are 300,590 estimated new cases of patients with breast cancer and about 43,700 deaths from breast cancer in the United States. 1 About 1 woman in 8 will be diagnosed with breast cancer during her lifetime. 1 The risk of getting breast cancer increases as a woman gets older, and the median age of diagnosis is 62. 1,2 Due to the ability of earlier detection and availability of innovative treatments, the 5-year relative survival rate of American women with breast cancer has improved to 91% in 2018. 1
About 3 out of 4 patients have breast cancers that are hormone receptor positive, and this percentage is higher in older women than in younger women. 3 For patients with hormone receptor positive breast cancer, endocrine therapy (ET) is routinely recommended to use for 5–10 years after the initial treatment of breast cancer to prevent cancer recurrence or death. 4 Tamoxifen has been the gold standard for ET among premenopausal and postmenopausal women with hormone receptor positive early-stage breast cancer for many years, but third generation aromatase inhibitors (AIs) have emerged as an alternative to tamoxifen in postmenopausal women due to benefits with better side effect profiles. 5,6 In 2019, the American Society of Clinical Oncology clinical practice guideline made the recommendations on extended adjuvant AI therapy based on benefits that include prevention of distant recurrence and prevention of second breast cancers. 4
Despite the survival and preventive benefits of ET, the uptake of and adherence to ET could be further improved across US women at different settings. 7,8 One large observational study found that 88% of commercially insured females with HR-positive breast cancer initiated ET and had 1-year adherence rate of 84%. 8 Another observational study reported that 23% of female Medicare beneficiaries with hormone receptor positive, stage I-III breast cancer did not initiate ET within 1 year, and 26% of those who initiated the treatment were not adherent. 7 Partridge et al. evaluated women with early-stage breast cancer in large commercial health programs and found that the mean adherence to adjuvant aromatase inhibitors decreased each year, ranging from 78% to 86% in Year 1 to 62% to 79% in Year 3. 9 Another analysis found that the overall adherence to adjuvant tamoxifen therapy in women with primary breast cancer could decrease to 50% by Year 4 of therapy. 10 The main reason of suboptimal uptake of and adherence to ET is due to their side effects (i.e., hot flashes, sexual dysfunction, weight gain, musculoskeletal symptoms, and fatigue). 11,12 One systematic review synthesized evidence from 26 studies and found that older and younger age, being single, having depression, having higher comorbidity index, and adverse effects were associated with poor 5-year ET adherence, whereas using AI instead of tamoxifen, receiving chemotherapy, and having prior medication were associated with increased adherence. 13 Since ET adherence is related to various and complex factors such as patient condition, therapy, health care system, and socioeconomic condition, understanding treatment initiation and adherence patterns and how these patterns may impact patient survival will optimize treatment decision-making. This observational retrospective study examined factors associated with early ET initiation, adherence, and survival among women with early-stage breast cancer.
Materials and Methods
Data source and sample
This retrospective new user cohort study analyzed the 2011–2019 Surveillance, Epidemiology, and End Results (SEER)-Medicare data (cancer site: breast cancer). The SEER-Medicare is a joint effort between the National Cancer Institute, SEER, and the Centers for Medicare & Medicaid Services. The SEER is a population-based cancer registry, which collects clinical data (i.e., tumor site, stage, grade), demographics (i.e., age, gender, race), and cause of death information for American cancer patients. 14 The Medicare administrative claims data include health care services for fee-for-service beneficiaries from the time of a person’s Medicare eligibility (aged 65 and older and younger individuals with permanent disabilities) until death, including hospital, skilled nursing home and hospice claims (Part A), physician office claims, outpatient claims, and home health utilization claims (Part B), as well as prescription drug claims (Part D).
We included female SEER-Medicare beneficiaries with newly diagnosed hormone receptor positive, stage I to III breast cancer (ICD-O-3 site code C50.0-C50.9) in 2012–2017 (SEER cancer registry data were available till 2017). To ensure continuous enrollment with Medicare, beneficiaries were limited to those who had full coverage in Medicare Parts A, B, and D for at least 12 months (washout period) prior to their breast cancer diagnosis. Beneficiaries who had Medicare Advantage (Medicare Part C) coverage were excluded because their medical claims/utilization are not fully captured. Beneficiaries who had any tamoxifen or AIs (i.e., anastrozole, exemestane, or letrozole) use or had contraindications (e.g., venous thromboembolism, oral anticoagulant use, and so on) with tamoxifen or AIs during washout period were excluded. Finally, a total of 55,893 female beneficiaries were eligible for this study (Fig. 1). Auburn University Institutional Review Board granted exempt approval for this study.
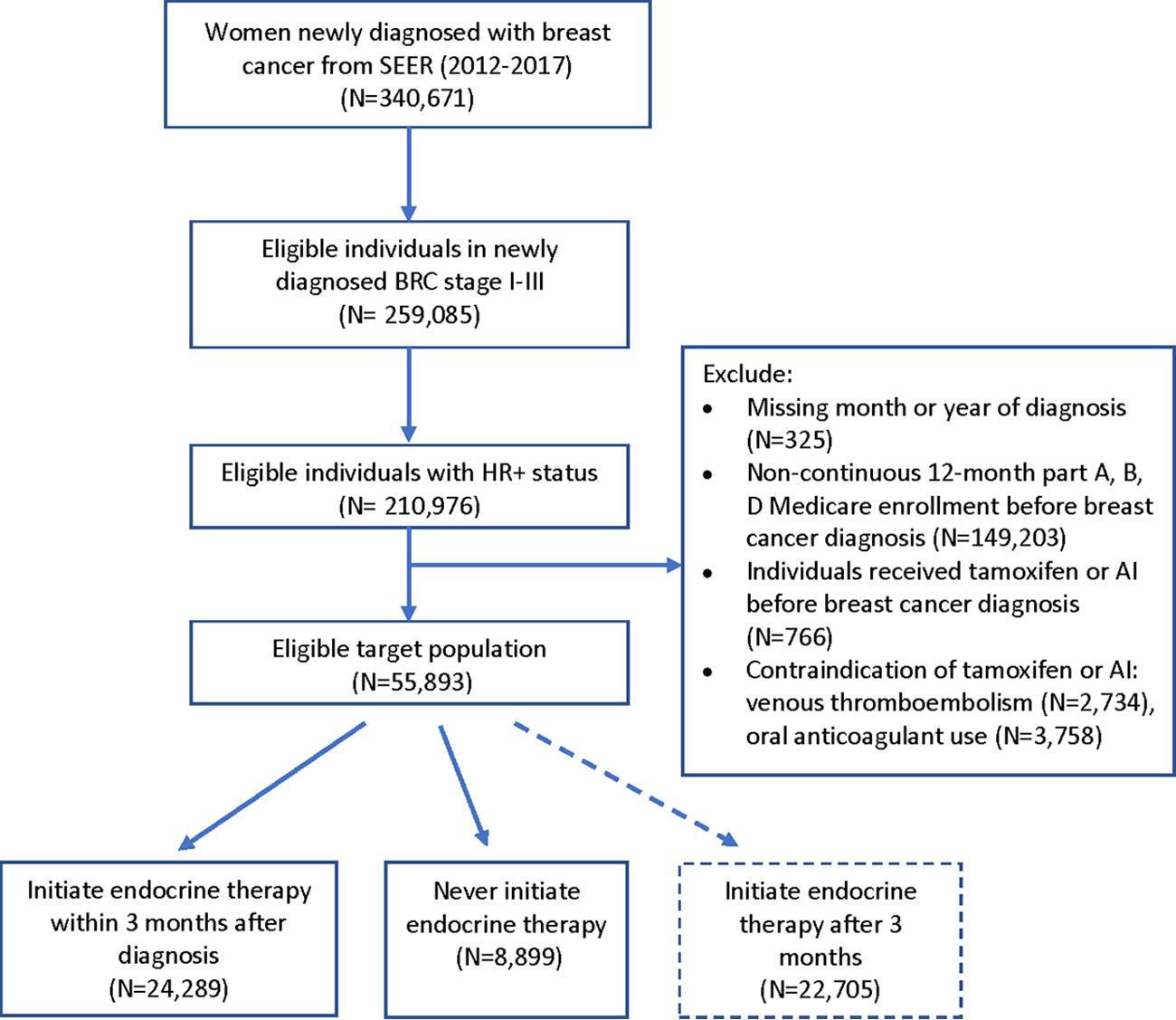
Sample selection flow chart.
Measurements
ET initiation
Beneficiaries who initiated a prescription of any of the four oral ET medications (tamoxifen, anastrozole, exemestane, and letrozole) within 3 months after their breast cancer diagnosis were categorized as initiators (n = 24,289), and those who never initiated these treatments during the entire study period were noninitiators (n = 8,899). ET prescriptions were identified in the Medicare Part D prescription claims data using corresponding National Drug Codes (NDC).
ET adherence
Treatment adherence to ET was measured using proportion of days covered (PDC) among beneficiaries with ≥2 ET prescriptions during the continuous 12-month follow-up period (continuously enrolled), in the form of dichotomous measurements (PDC ≥ 80% as adherent and <80% as nonadherent). PDC was calculated as total days’ supply of studied drugs (any of the 4 drugs as overall adherence) divided by the total number of days of study participation (i.e., 365 days for 12 months), and it was capped at 1.0 or 100%. 15
Mortality
All-cause and breast cancer related mortality were examined using the SEER’s records in date and cause of death (i.e., cancer or noncancer causes) after ET initiation (versus noninitiators). The follow-up started when patients initiated the treatment within a grace period of 3 months and ended at the occurrence of a mortality event, administrative censoring (12 months after ET initiation), or December 31, 2019 (December 31, 2018 for breast cancer related mortality), whichever occurred first.
Covariates
Baseline covariates that included patient characteristics [age, race/ethnicity, geographic region, marital status, comorbidity, emergency room visit], cancer characteristics [tumor grade, cancer stage, receptor status (i.e., estrogen receptors (ER) positive, progesterone receptors (PR) positive, and HER2 positive)], and breast cancer screening services (mammography, CT scan/ultrasound) were measured during the 12-month washout period or at the time of cancer diagnosis (i.e., cancer characteristics) between ET initiators and noninitiators. Patient’s demographic information and marital status were available in the Medicare enrollment records. Comorbidity, using the Charlson Comorbidity Index (CCI), 16 was identified using diagnosis codes with corresponding conditions (i.e., diabetes, congestive heart failure, and so on) in the Medicare medical claims data files during the 12-month baseline period. Emergency room visit (Yes/No) and breast cancer screening services (binary variables) were identified with corresponding revenue center codes and Healthcare Common Procedure Coding System (HCPCS) codes, respectively, from Medicare claims data files during baseline. Cancer/tumor characteristics variables were available from the SEER registry. Cancer stage was based on the SEER combined summary stage variable as follows: “Localized was identified as an invasive neoplasm confined entirely to the organ of origin. Regional was identified as neoplasm that has extended beyond the limits of the organ of origin directly into surrounding organs or tissues, into regional lymph nodes by way of the lymphatic system, or by a combination of extension and regional lymph nodes.” 17
Statistical analysis
Descriptive statistics with frequency count and percentage for categorical covariates and means and standard deviation (SD) for continuous/count variable were used to describe the study sample and compare the distributions between ET initiators and noninitiators. Multivariable logistic regression models were used to assess factors associated with ET initiation and adherence (PDC ≥80%), controlling for covariates (including patient’s age, race/ethnicity, geographic region, marital status, breast cancer stage, tumor grade, receptor status, CCI, any emergency room visit, and use of breast cancer screening services). Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were reported. Inverse-probability weighting (truncated the weights at the 5th and 95th percentiles) was used to balance baseline covariates between initiators and noninitiators, and weighted Cox proportional hazard models were used to estimate hazard ratios (HRs) and 95% CIs of all-cause and breast cancer related mortality between initiators and noninitiators. A series of sensitivity analyses were conducted to further reduce the impact of extreme weights on the variance (#1, to truncate the weights at the 1st and 99th percentiles), 18 to adjust for time-varying ET exposure on mortality [#2, to censor observations with ET treatment discontinuation (defined as a gap of ET prescription fill > 30 days)], to reduce biases on mortality from other cancer treatments (#3–5, to limit to ET initiators and noninitiators who had surgery/radiation/chemotherapy within 3 months after breast cancer diagnosis, respectively), to expand the grace period of ET initiation (#6, to expand to patients who initiated ET within 6 months after their breast cancer diagnosis), and to assess the association between ET adherence and mortality (#7, to compare patients who were adherent to ET treatment versus noninitiators, and patients who were nonadherent to ET treatment versus noninitiators). NDC, diagnosis codes, and HCPCS codes used to identify surgery/radiation/chemotherapy from Medicare medical and prescription claims data could be found in Supplementary Data S1. 19 All analyses were conducted using SAS version 9.4 (SAS Institute, Inc., Cary, NC) at significance level of p < 0.05.
Results
Study sample
This study included a total of 55,893 eligible female Medicare beneficiaries who were newly diagnosed with HR-positive, stage I to III breast cancer. Among them, 24,289 (43%) initiated ET treatment in 3 months after cancer diagnosis, 22,705 (41%) initiated ET treatment after 3 months, and 8,899 (16%) never initiated ET treatment (Fig. 1). Majority of the sample were 65 years and older (94.1%), non-Hispanic White (83.4%), residing in Northeast (40.4%) and West (32.4%), having tumor grade II (50.2%), and local cancer stage (83.4%) (Table 1).
Baseline Characteristics of ET Initiators and Noninitiators Among Patients Newly Diagnosed with Breast Cancer in SEER-Medicare (2011–2019) and Factors Associated with ET Initiation
Chi-square test for categorical variables and paired t-test for continuous/count variables.
Multivariable logistic regression model.
OR, odds ratio; CI, confidence interval; ER, estrogen receptors; PR, progesterone receptors.
Bold data indicated statistically significance at p < 0.05.
ET initiation
Among a total of 55,893 beneficiaries, 24,289 (43%) initiated ET treatment in 3 months (Table 1). Compared with ET noninitiators (n = 8,899), initiators were more likely to be older, non-Hispanic White (versus Black), residing in the Northeast and South regions, married, have higher tumor grade (II versus I) and regional cancer stage, cancer receptors positive, have less comorbidity and emergecy room visit, and use cancer preventative services, including mammography and CT scan/ultrasound (all p < 0.05). Multivariable results showed that factors associated with a significantly higher likelihood of early ET initiation included older age (adjusted OR = 2.26, 95%CI = 2.03–2.50 for 65–74; adjusted OR = 1.71, 95%CI = 1.54–1.89 for 75–84; adjusted OR = 1.20, 95%CI = 1.07–1.34 for ≥85) (versus <65), being Hispanic (adjusted OR = 1.13, 95%CI = 1.25–1.27) or Asian (adjusted OR = 1.33, 95%CI = 1.17–1.51) (versus White), having higher tumor grade (adjusted OR = 1.23, 95%CI = 1.16–1.30 for II (versus I) and regional cancer stage (adjusted OR = 1.46, 95%CI = 1.36–1.56) (versus local), being ER (adjusted OR = 10.25, 95%CI = 7.38–14.24) or PR (adjusted OR = 1.65, 95%CI = 1.52–1.79) positive, and having mammography at baseline (adjusted OR = 1.07, 95%CI = 1.03–1.15). Being Non-Hispanic Black (adjusted OR = 0.89, 95%CI = 0.81–0.99) (versus White), residing in Midwest (adjusted OR = 0.76, 95%CI = 0.69–0.85) and West (adjusted OR = 0.53, 95%CI = 0.49–0.57) (versus Northeast), not married (adjusted OR = 0.88, 95%CI = 0.83–0.94), having higher tumor grade (adjusted OR = 0.83, 95%CI = 0.77–0.91 for III (versus I), and having emergency room visit (adjusted OR = 0.86, 95%CI = 0.81–0.91) were associated with lower likelihood of early ET initiation (Table 1).
ET adherence
Among the 24,289 ET initiators, a total of 22,961 (95%) beneficiaries filled at least two ET prescriptions (n = 22,961) during the 12-month follow-up period. Among them, a total of 17,783 (77%) were adherent (PDC ≥80%) to their therapy in 12 months. Adherence to treatment (PDC ≥ 80%) was more likely to achieve among women who were in older age (65+ versus <65, adjusted OR = 1.30, 95%CI = 1.12–1.50 for 65–74; adjusted OR = 1.19, 95%CI = 1.03–1.37 for 75–84; adjusted OR = 1.17, 95%CI = 1.01–1.38 for ≥85), non-Hispanic Asian (versus White, adjusted OR = 1.48, 95%CI = 1.25–1.75), and had mammography (versus those who did not have mammography, adjusted OR = 1.22, 95%CI = 1.13–1.30). However, women who were residing in the West (versus Northeast, adjusted OR = 0.72, 95%CI = 0.65–0.79), not married (versus married, adjusted OR = 0.91, 95%CI = 0.84–0.98), and had at least one emergency room visit (versus those did not have any visit, adjusted OR = 0.82, 95%CI = 0.76–0.88) were less likely to adhere to ET treatment (Table 2).
Predictors of Adherence to ET (Proportion of Days Covered (PDC) ≥80%) Among Patients with Breast Cancer in SEER-Medicare (2011–2019) (n = 22,961)
Multivariable logistic regression model.
OR, odds ratio; CI, confidence interval; ER, estrogen receptors; PR, progesterone receptors.
Bold data indicated statistically significance at p < 0.05.
All-cause and breast cancer related mortality
The incidence rates of all-cause and breast cancer related mortality were 43.11/1,000 person-years and 7.76/1,000 person-years among ET initiators compared with 78.56/1,000 person-years and 17.5/1,000 person-years among noninitiators, respectively (Table 3). Unadjusted results showed that ET initiators had lower risk in both all-cause (HR = 0.55, 95%CI = 0.52–0.57) and breast cancer related mortality (HR = 0.46, 95%CI = 0.41–0.52) than noninitiators. After weighting, ET initiation was also associated with reduced risk of all-cause (adjusted HR = 0.62, 95%CI = 0.59–0.66) and breast cancer related mortality (adjusted HR = 0.57, 95%CI = 0.50–0.64). Among initiators, those who were adherent to ET treatment were associated with reduced risk of all-cause (adjusted HR = 0.55, 95%CI = 0.53–0.59) and breast cancer related mortality (adjusted HR = 0.41, 95%CI = 0.36–0.47) compared with noninitiators. Those who were nonadherent to ET treatment were also associated with reduced risk of all-cause (adjusted HR = 0.85, 95%CI = 0.80–0.91) and breast cancer related mortality (adjusted HR = 0.72, 95%CI = 0.63–0.84) compared with noninitiators. All results from sensitivity analyses were consistent with main findings (Table 3).
Effect of Initiation of ET on Survival Outcomes Among Patients Diagnosed with Breast Cancer in SEER-Medicare (2011–2019)
Other causes of death were treated as a competing event in the Fine and Gray model.
Cases per 1,000 person-years.
End of follow-up: death or end of administrative data (December 31, 2018, for breast cancer-related mortality or December 31, 2019, for all-cause mortality), whichever occurred first. Weighted Cox proportional hazard models were used to estimate HRs and 95% CIs, adjusted for baseline covariates and censoring due to loss to follow-up.
End of follow-up: Medicare Part A, B, D disenrollment, a gap of prescription fill >30 days, death, or end of administrative data (December 31, 2018, for breast cancer-related mortality or December 31, 2019, for all-cause mortality), whichever occurred first.
Within 3 months of breast cancer diagnosis: Had surgery (n = 20,863 among ET initiators and n = 7,275 among noninitiators); had radiation (n = 9,741 among ET initiators and n = 2,365 among noninitiators); and had chemotherapy (n = 1,183 among ET initiators and n = 941 among noninitiators). NDC, ICD, HCPCS codes for identifying these cancer treatments can be found in Supplementary Data S1.
After expanding to patients who initiated ET within 6 months, n = 37,632 for initiators versus n = 8,899 for noninitiators.
After limiting to patients who had ≥2 ET prescriptions during the continuous 12-month follow-up period, n = 17,783 for those who were adherent to ET treatment (PDC ≥80%) versus n = 8,899 for noninitiators, and n = 5,178 for those who were nonadherent to ET treatment (PDC <80%) versus n = 8,899 for noninitiators.
ET, endocrine therapy; HR, hazard ratio; CI, confidence interval.
Discussion
Our findings indicate that less than half (43%) of female Medicare beneficiaries newly diagnosed with early-stage breast cancer initiated ET within 3 months of cancer diagnosis. Among these early initiators, less than 80% of them were adherent to ET during the first 12 months. Certain patient’s demographics, cancer characteristics, and mammography use are associated with ET treatment initiation among women with early-stage breast cancer. Mammography use was also associated with better adherence. Importantly, our findings demonstrated that female beneficiaries with early-stage breast cancer may achieve survival benefits when they initiate ET in 3 months after cancer diagnosis.
Despite the benefits of ET, the uptake of and adherence to ET as recommended by guidelines could be further improved across U.S. women at different settings. 7,8 One large observational study found that 72% of adult female early-stage breast cancer patients with private health insurance initiated ET, and their 1-year adherence rate was 84% and the 5-year rate was 65%. 8 Another observational study analyzed the 2007–2011 SEER-Medicare data and reported that 23% of female Medicare beneficiaries with hormone receptor positive, stage I-III breast cancer did not initiate ET within 1 year, and 26% of those who initiated the treatment were not adherent. 7 Our finding in proportion of ET adherence among female Medicare beneficiaries with newly diagnosed early-stage breast cancer is consistent with these earlier studies. The lower proportion of ET initiation observed in this study is likely because we focused on the initiation during the first 3 months (early adopters) after cancer diagnosis. The main reason of suboptimal uptake of and adherence to ET is due to their side effects (i.e., hot flashes, sexual dysfunction, weight gain, musculoskeletal symptoms, fatigue, and insomnia). 11,12,20 –23 Therefore, improved management of side effects is needed for maintaining patients on treatment.
A few studies have identified factors associated with ET initiation and adherence among women with breast cancer. Bowles et al. found that women with older age, earlier-stage tumor, and being Black in race were less likely to initiate ET than their counterparts, 24 which is mostly consistent with our finding. In addition, we found that patient’s geographic location (i.e., residing in the Northeast), marital status (i.e., married), and use of mammography were also associated with higher likelihood of ET initiation. Wu et al. reported that women with breast cancer who were living in high-poverty areas and receiving treatment at non-Commission on Cancer hospitals were less likely to receive guideline recommended hormonal therapy. 25 Indeed, providers’ prescribing preference and patients’ socioeconomic characteristics and access to preventive services such as mammography might vary by geographic region, which should be considered and targeted in the development of effective intervention in improving ET initiation among women with breast cancer.
In contrast, one systematic review synthesized evidence from 26 studies and found that older and younger age, being single, depression, higher comorbidity index, and adverse effects were associated with poor 5-year ET adherence, whereas using AI instead of tamoxifen, having received chemotherapy, and prior medications were associated with increased adherence. 13 We also found that older age and being married were significant factors associated with higher ET adherence in our Medicare sample. As factors associated with ET initiation, we also found that patient’s geographic location (i.e., residing in the Northeast) and use of mammography were associated with higher ET adherence. Zhao et al. analyzed commercial claims data of adult breast cancer patients and also found that those who lived in the Northeast were associated with better ET adherence. 8 Kimmick et al. explored the use of adjuvant hormonal therapy in an insured, low-income women sample and found poor adherence (60%). 26 Our earlier work also indicated that older women who used mammography had better ET adherence as preventive treatment for breast cancer. 27 Since ET adherence is related to various and complex factors such as patient characteristics, 8,22,27,28 disease condition and therapy, 8,28 health care system, 28,29 access to care, 27 and out-of-pocket cost, 8,22,29,30 understanding initiation and adherence patterns and how these patterns vary by key factors will provide evidence in optimizing treatment decision-making and improving treatment uptake and adherence. Physicians should actively monitor ET adherence over time and evaluate treatment options with minimal side effect profiles and out-of-pocket cost to better support adherence for patients with breast cancer.
In addition, our findings demonstrated that female Medicare beneficiaries with early-stage breast cancer may achieve all-cause and breast-cancer related survival benefits when they initiate ET early on. Our finding is consistent with current understanding and evidence in the significant benefit of ET on survival among patients with early-stage, hormone receptor positive breast cancer. 31,32 Lee et al. investigated the impact of delayed ET initiation (after 12 months of diagnosis) on survival among a large, diverse (in age and health insurance coverage) sample of women with stage II and III HR-positive, HER2-negative, invasive breast cancer. They found that delayed ET had no statistically significant effect on the hazard of death (adjusted HR = 1.01; 95%CI = 0.96–1.06) compared with initiation within 12 months of diagnosis, so they suggested that clinicians should not be discouraged from initiating ET more than 12 months after diagnosis. 33 Compared with our Medicare sample, Lee et al. included a much younger, commercial insurance dominated group of patients. Based on the results from their sensitivity analysis, women who initiated ET within 12 months of cancer diagnosis had significant survival benefit compared with those who never initiated ET, 33 which is consistent with our findings. All results from our sensitivity analyses were consistent with main findings, including propensity score weighting trimming, adjusting for ET treatment discontinuation and other cancer treatments, expanding to patients who initiated ET treatments in 6 months, and examining the associations between ET treatment adherence and mortality. Indeed, cancer treatments such as chemotherapy, surgery, and radiation treatment are of great importance to treat breast cancer. Patients in whom adjuvant chemotherapy is recommended are at higher risk for breast cancer recurrence and mortality, 34 and our results suggested that survival benefit of early ET initiation among this high-risk group of patients is still significant compared with noninitiators. Our finding also confirms the benefit of adherence to ET treatment with respect to survival. Although all patients who were adherent and nonadherent had lower risk of all-cause and breast cancer related mortality compared with noninitiators, the magnitude of HRs for patients who were adherent and nonadherent was different (HR = 0.55 versus 0.85 for all-cause mortality and HR = 0.41 versus 0.72 for breast cancer related mortality, respectively), and the corresponding 95% CIs were not overlapping. Our study highlights the importance of ET treatment adherence in breast cancer survivorship and calls for interventions for improving adherence, such as improved follow-up targeting adherence and persistence, in clinical practice.
There were some limitations to our study. Although our findings are based on a large sample of female Medicare beneficiaries with early-stage breast cancer across the United States and many clinically significant confounders such as age, cancer stage and tumor grade, comorbidities, and ET persistence were controlled in the analysis, unmeasured confounding remains an issue for observational studies. Our analysis did not limit to patients with the completion of chemotherapy or surgery since most (>90%) of older women with early-stage breast cancer receive surgery prior to ET in the United States. 35 In addition, we assessed the first year ET adherence, which is likely higher compared with subsequent years. 8 The next step is to measure ET adherence over a longer duration (e.g., 5–10 years) and adopt a dynamic adherence measure such as the adherence trajectory. 36 Finally, our findings may not be generalizable to non-Medicare populations or delayed ET adopters since our sample focused on Medicare beneficiaries who initiated ET during the first 3 months after cancer diagnosis. Medicare beneficiaries who received coverage due to permanent disability (e.g., those who enrolled before age 65 years) are not typically considered to be representative of the younger than 65-year-old general or disabled populations. Although our sample included Medicare beneficiaries younger than 65 years old with early-stage breast cancer (4.85% ET initiators and 8.93% noninitiators), findings from this SEER-Medicare analysis may not be generalizable to younger populations who are not enrolled in Medicare. 37
Conclusions
In conclusion, this study highlighted the survival benefits of initiation of ET in 3 months after diagnosis compared with noninitiators among women with early-stage breast cancer. Our findings are strengthened by the large sample and multiple sensitivity analyses. Interventions to further improve ET initiation and adherence in breast cancer survivors should be developed and evaluated.
Footnotes
Acknowledgments
The authors acknowledge the efforts of the National Cancer Institute; the Centers for Medicare & Medicaid Services, Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database.
Disclaimer
This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by B.T. and J.Q. The first draft of the article was written by J.Q., and all authors commented on previous versions of the article. All authors read and approved the final article.
Data Availability
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board of Auburn University (#21–597).
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.