
Abstract
Introduction:
Understanding the incidence and predictors of postpartum depression (PPD) among active-duty service members is critical given the importance of this population and its unique stressors.
Methods:
We conducted a retrospective cohort study of all active-duty U.S. Army soldiers with a record of at least one live-birth delivery between January 2012 and December 2013. Multivariate logistic regression models were used to estimate associations between demographic, health-related, and military-specific variables and diagnoses of PPD in the total population (N = 4,178) as well as in a subpopulation without a record of depression before delivery (N = 3,615).
Results:
The overall incidence of PPD diagnoses was 15.9% (N = 664 cases) among the total population and 10.4% (N = 376 cases) among those without prior depression. Statistically significant predictors of PPD in the adjusted model included lower pay grade, a higher number of prior deployments, a higher number of child dependents, tobacco use, and a history of depression or anxiety before or during pregnancy. For soldiers without a history of depression, lower pay grade, and a history of anxiety before or during pregnancy were significantly associated with PPD.
Conclusions:
Knowing the predictors of overall and novel onset PPD diagnoses in this population could help establish clearer guidelines on PPD prevention, screening, management, and return to duty.
Introduction
Postpartum depression (PPD) is a debilitating and common condition, reported to affect 10–20% of women following birth. 1 –3 It is a mood disorder characterized by feelings of intense sadness, anxiety, or despair that interfere with daily life, and that can occur in women up to 1 year after birth. 4
PPD elevates the risk of poor health outcomes among mothers and their children. Mothers with PPD have increased risks of suicidality, 5 other mood disorders, and substance abuse. 6 –11 Children born to mothers with PPD are less likely to be breastfed, may have decreased mother–infant bonding and impaired cognitive and emotional development, and are at increased risk of developmental disorders and abuse. 6,12 –14
A wide range of risk factors have been identified for PPD, including a history of depression, substance use, domestic violence, stressful life events, a lack of social or marital support, poor physical health, and negative body image. 15,16 Low socioeconomic status has also been associated with PPD risk and there is evidence of different rates across race/ethnicity groups. 17 –19 Finally, there is some evidence that pregnancy-related complications are associated with increased PPD risk. 2,20
Less is known about PPD within vulnerable populations, including whether the risk factors identified thus far are generalizable to these groups. One population of particular interest is active-duty military servicemembers (SMs), a large proportion of whom are of child-bearing age and all of whom are exposed to a unique set of stressors relative to women in the general population.
One recent study evaluated PPD in military populations, examining clinical diagnoses of depression among both active-duty service women in the U.S. Armed Forces and dependent spouses from 2007–2012, using data from the Defense Medical Surveillance System. 5 In this study, 9.9% of active-duty service women and 8.2% of dependent spouses received PPD diagnoses by one year postpartum. Do and colleagues also reported that a history of mental disorder diagnoses was more common among service women and dependent spouses diagnosed with PPD, and that PPD was a predictor of future suicidality. A more recent population-based study reported increasing rates of PPD across time from 2001 to 2018 and examined differences across military branches. 21
Beyond these two studies, other work focusing on PPD among active-duty service women has typically been limited in size and/or have used self-reported symptom data, rather than clinical diagnoses, 22 –24 which may overestimate prevalence. 25 Large studies of incidence and risk factors of PPD in service women looking at key military, demographic, and health-related risk factors, especially during periods with a substantial deployment tempo, are essential to help create clearer guidelines on screening, management, and return to duty in this population.
In this study, we add to the prior literature in two important ways. First, we utilized longitudinal data that enabled us to observe women with at least a year of data before pregnancy and a year following delivery to explore both prepregnancy-related and pregnancy-related predictors of PPD, as well as to establish robust capture of PPD diagnoses. Second, we leveraged these longitudinal data to determine the incidence and predictors of what we term “novel onset PPD”—that is, PPD among women without a history of a depression diagnosis during pregnancy or during the year before pregnancy.
Materials and Methods
Study population
We conducted a retrospective cohort study using a longitudinal dataset with administrative and medical encounter information for active-duty U.S. Army soldiers recorded at the person–month level with data available between January 2011 and December 2014. Because we were limited to month-level data and were thus unable to determine with precision the pregnancy start date, we defined pregnancy length as 8 months for normal deliveries and 5 months for preterm labor.
We used the following criteria to define the study population (Fig. 1). First, we identified all soldiers with at least one delivery during the timeframe of our study (N = 18,493). For those soldiers with more than one delivery within the study period, only the first was included. To ensure sufficient capture of soldiers’ medical history before pregnancy, as well as their experience following delivery, only those soldiers with a minimum of 1 year of data both before pregnancy and following delivery were included (N = 4,229). We additionally excluded 51 soldiers with unknown education or body mass index (BMI) from the analysis, which resulted in N = 4,178 individuals in our primary analysis of PPD incidence. For the secondary analysis focused on novel onset PPD, by which we mean PPD occurring among women without a history of depression, we further excluded soldiers with diagnoses of depression before delivery, resulting in a study population of N = 3,615 soldiers.
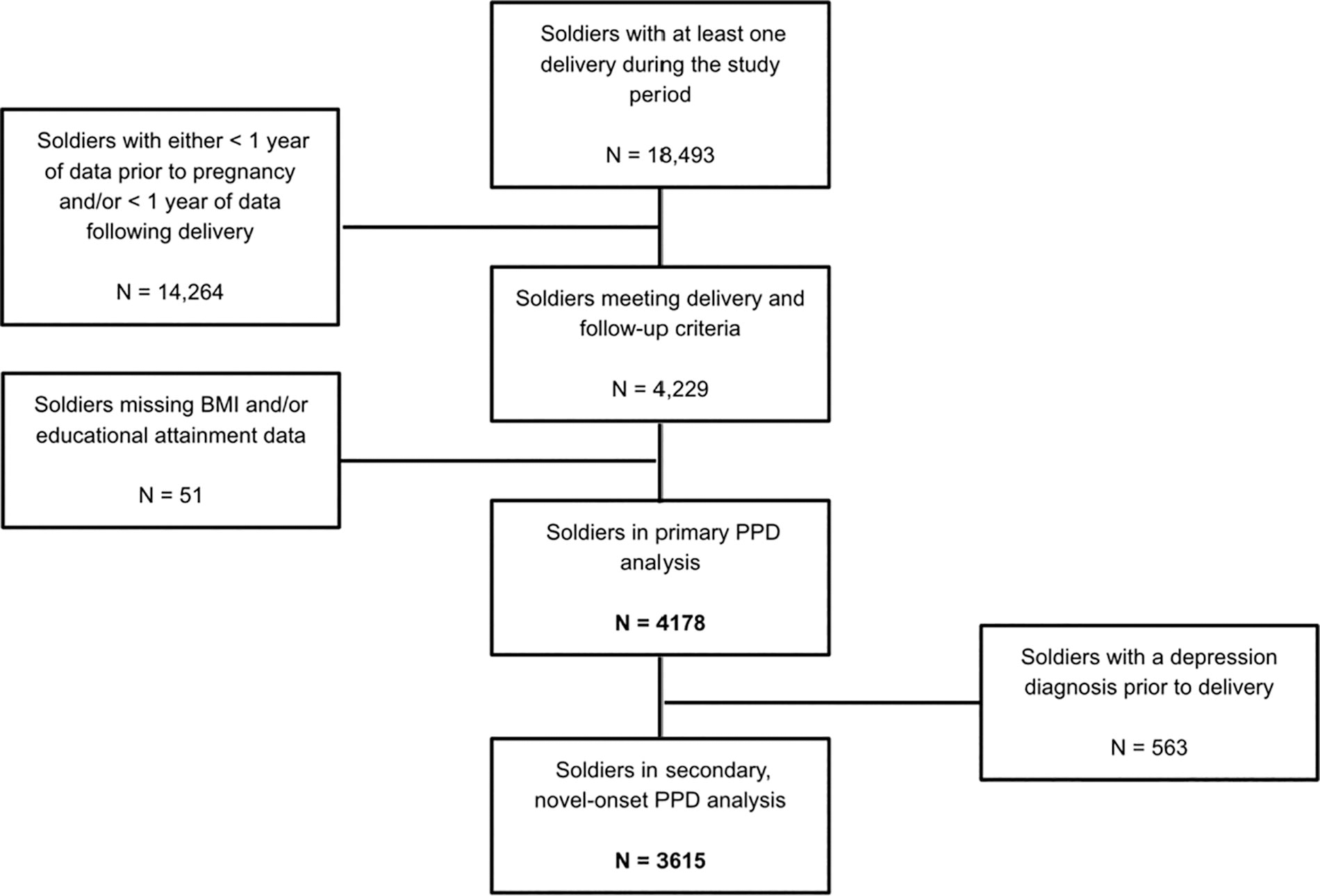
Flowchart describing construction of analytic samples for study of postpartum depression in the U.S. Army, 2011–2014.
Outcome variable
Our outcome of interest was PPD, identified by a diagnosis of depression occurring during the month of delivery or in the 11 months following the month of delivery. We defined our primary outcome by the presence of at least one of the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes: major depressive disorder single episode (296.20–296.26); major depressive disorder recurrent episode (296.30–296.36); depressive disorder, not classified elsewhere (311); and mental disorders of mother, postpartum conditions, or complications (648.44). Codes were extracted from health care encounter data as recorded in the Military Health System Data Repository (MDR), which includes both inpatient and outpatient care taking place both within and outside of military facilities. We also analyzed a subset of cases of PPD we have termed “novel onset PPD,” which includes only those women with a diagnosis of PPD, as defined by the codes listed above, for whom there were no diagnoses of depression either during pregnancy or in the year(s) before pregnancy.
Predictor variables
We used administrative data from the Department of Defense Manpower Data Center to identify each soldier’s period of active-duty service, which defined the observable time for the subjects. This data source also provided maternal age, self-reported race, ethnicity, education level, marital status, number of children in the household, military pay grade, and number of prior deployments. Military pay grade was categorized into junior enlisted soldiers (E1–E4), noncommissioned officers (E5–E9); and warrant officers and commissioned officers (W1–W5; O1–O10). All sociodemographic data were captured at the time of delivery.
We used data from both the MDR and the Digital Training Management System to obtain soldiers’ average weight and height to calculate the soldiers’ prepregnancy BMI. Given the sensitivity of BMI to pregnancy status, we used the last measured BMI for each soldier that was collected at least eight months before delivery to define BMI before or at the beginning of pregnancy. We utilized data from soldiers’ annual health exams, termed periodic health assessments, to identify soldiers with a history of high alcohol consumption. As with BMI, we utilized the most recent data collected on this before pregnancy.
All prior mental health disorder diagnoses made during the study time period were defined as either occurring before pregnancy, during pregnancy, or during both time periods, based on their month of occurrence relative to delivery.
We used the following ICD-9-CM diagnosis codes in the MDR encounter data to identify soldiers’ health conditions: anxiety states (300.0, 300.01, 300.02); post-traumatic stress disorder (PTSD) (309.81); preeclampsia (642.0, 642.1, 642.2, 642.3, 642.9, 642.74); gestational diabetes (648.8); preterm labor (644.2, 644.20); and multiple birth (651).
Statistical analysis
We first compared the populations of women with and without PPD descriptively using chi-square testing. We then used multivariable logistic regression models to test for associations between the demographic, military-specific, and health-related predictors described above and PPD. For the primary analysis, we examined the relationship between these predictors and all cases of PPD. For our secondary analysis, we examined the relationship between these predictors (excluding prior depression) and novel onset PPD. We used Stata MP, version 14.2 (StataCorp LP, College Station, Texas) for all analyses. All reported p-values are two-sided and we used p < 0.05 as a significance cutoff. This study was approved by the Institutional Review Board at Stanford University and also underwent secondary review by the human research protections office of the Defense Health Agency.
Results
In 2012–2013, a total of 4,178 deliveries were identified for the primary analysis (Fig. 1). Among soldiers who gave birth, we identified 664 PPD cases, for a cumulative incidence of PPD of 15.9%. Among soldiers without a recent history of depression (N = 3,615 deliveries), we observed 376 cases of PPD, for a cumulative incidence of novel onset PPD of 10.4%.
Tables 1 and 2 contrast the demographic, military-related, and health-related characteristics of soldiers with and without PPD. We observed significant distribution differences for many of the characteristics included and the differences were largely consistent when considering either all cases of PPD or those with novel onset PPD. Soldiers with PPD were significantly over-represented among those in the lowest educational attainment category and were more likely to be formerly married, to have a larger number of dependents, to be in a lower pay grade category, and to use tobacco. Much higher percentages of women with PPD—on the order of 3- to 5-fold differences—had a history of depression, anxiety, or PTSD, either before or during pregnancy (Table 1). A significantly higher proportion of women with PPD also experienced preterm labor, both among all PPD cases and those with novel onset PPD.
The total number of participants in the primary analysis was 4,178.
The total number of participants in the novel-onset depression analysis was 3,615.
p-values are based on chi-square test.
Army pay grade: E1–E4 junior enlisted, E5–E9 noncommissioned officer, W1–W5 & O1–O10 warrant officer and commissioned officer.
Health and Health-Related Behavior Characteristics of the Study Population, Comprising Soldiers on Active Duty in the U.S. Army, Giving Birth between January 2012 and December 2013 (N = 4,178 a /N = 3,615 b ). Values in the Table Represent the Percent of Soldiers within a Given Column with the Condition of Interest
The total number of participants in the primary analysis was 4,178.
The total number of participants in the novel-onset depression analysis was 3,615.
p-values are based on the chi-square test.
Health-related factors are coded as binary, only prevalence is presented.
Last known status reported by the patients, based on health encounter reports.
Table 3 shows the results of the adjusted logistic regression models predicting PPD and novel onset PPD. In the primary analysis focused on all PPD cases regardless of depression history, the adjusted odds of PPD were significantly higher among women with two or more children (odds ratio [OR] = 1.32, confidence interval [CI]: 1.01–1.72, p = 0.043). There was a significantly lower adjusted PPD odds among Asian and Pacific Islanders compared with White women (OR = 0.63, 95% CI: 0.41–0.97, p = 0.035).
The total number of participants in the primary analysis was 4,178.
The total number of participants in the novel-onset depression analysis was 3,615.
Depression before pregnancy is not applicable in the secondary analysis, because soldiers with preexisting depression were excluded.
Depression during pregnancy is not applicable in the secondary analysis, because soldiers with preexisting depression were excluded.
Multiple births is a binary variable indicator if the soldiers were pregnant with more than one baby in this pregnancy.
In terms of military characteristics, noncommissioned officers (OR = 0.64, CI: 0.49–0.84, p = 0.001) and warrant officers and commissioned officers (OR = 0.54, CI: 0.33–0.89, p = 0.016) had significantly lower odds of PPD compared with women in the lowest pay grades. The odds of PPD were also significantly higher among soldiers with a history of two or more deployments relative to those with none (OR = 1.33, CI: 1.00–1.78, p = 0.048).
In terms of medical characteristics, a history of depression before delivery was, perhaps not surprisingly, the strongest risk factor. The odds of PPD among those who had had depression before and during pregnancy were 2.75 and 7.91 times those, respectively, of soldiers with no depression history (p for both < 0.001). A history of anxiety was also a significant risk factor for PPD, whether it occurred before pregnancy (OR = 1.68, CI: 1.25–2.27, p = 0.001) or during pregnancy (OR = 2.04, CI: 1.44–2.90, p < 0.001). PPD risk was significantly higher among tobacco users (OR = 1.28, CI: 1.04–1.57; p = 0.018). There were also significantly higher odds of PPD among women with preterm labor (OR = 1.45, CI: 1.04–2.03; p = 0.028).
Among the 3,615 soldiers in the analysis that was focused on novel onset PPD, being in a higher pay grade was even slightly more protective than was observed in the primary PPD analysis. Noncommissioned officers (OR = 0.61, CI: 0.44–0.85, p = 0.003) and warrant officers and commissioned officers (OR = 0.41, CI: 0.22–0.78, p = 0.006) had significantly lower odds of novel onset PPD compared with women in the lowest pay grades. A history of anxiety showed a strong positive association with novel onset PPD, both before pregnancy (OR = 2.23 CI: 1.52–3.26, p < 0.001) and during pregnancy (OR = 2.27 CI:1.43–3.60, p = 0.001). Among those women without a history of depression, we did not see significant associations with the number of child dependents, deployments, tobacco use, or preterm labor, although it should be noted that the effect sizes were very similar to those found in the analysis of all PPD outcomes.
Discussion
In this study of active-duty U.S. Army soldiers, we found that 15.9% of mothers experienced PPD, as ascertained via a depression diagnosis code, during the year following delivery. The strongest risk factor that emerged was the presence of mental health disorder diagnoses before delivery, especially those during pregnancy. We also studied the subset of women with no prior history of depression to determine the incidence of and risk factors for what we term “novel onset PPD,” which afflicted 10.4% of women without a history of a recent diagnosis of depression. We found that anxiety, either before pregnancy or during pregnancy, was a significant predictor of novel onset PPD. Our findings may provide an opportunity for proactive care of these mothers during and after pregnancy.
According to previous studies, an estimated 10–20% of women develop PPD, indicating that our study population is in the middle of the risk scale for this condition. 1 –3,26 In the study most analogous to ours, Do et al. reported that 9.9% of active-duty SMs had developed PPD, although it should be noted that the strategy they employed to ascertain PPD was more restrictive than ours. 5
Our analysis identified several risk factors for PPD across multiple areas of interest. Important psychiatric risk factors included diagnoses of depression and anxiety, especially during pregnancy. Of the obstetric factors analyzed, only preterm labor was found to be associated with significant increase in the odds of PPD. In terms of military factors, a higher number of deployments and lower pay grade were found to be related to PPD risk. Lastly, while the findings for subjects with novel-onset PPD were broadly similar overall to those in the total group, the estimate for anxiety as a risk factor was slightly stronger.
As expected, our findings confirmed that the presence of a mental health disorder before delivery, and especially during pregnancy, is an important risk factor for PPD. Individuals with a history of depression before pregnancy had nearly threefold the risk of PPD compared with those with no history of depression, and those with depression during pregnancy had nearly eightfold the risk. Anxiety before and during pregnancy was also predictive of PPD risk, although to a lesser degree than depression. The effect estimates for both anxiety and depression were higher when occurring during pregnancy rather than before pregnancy, suggesting that mental health during pregnancy will be more informative of mental health postpartum than overall mental health history.
PTSD was notably not found to be a significant predictor of PPD, whether it presented before or during pregnancy in our overall analysis. This contrasts with literature that has found PTSD history to increase PPD risk. 27 While we observed a twofold increase in the adjusted odds of PPD in association with PTSD before pregnancy in the novel-onset PPD group, this elevation was only suggestive in terms of the hypothesis test results (p = 0.063). PTSD diagnoses were quite rare relative to diagnoses of depression or anxiety, so it is possible we lacked sufficient power to test this association. Another possibility is that because PTSD and combat deployment are linked, and we controlled for deployment, the PTSD-PPD association seen in others’ work was simply the product of unrealized confounding. A similar phenomenon was seen in recent work on the relationship of PTSD, combat experience, and preterm labor, wherein control for recency of combat experience eliminated a PTSD effect that was suspected from prior literature. 28
In terms of birth-related factors, we found that preterm labor was associated with a significant increase in PPD risk (OR = 1.45, p = 0.028). Our analysis did not find significant associations between other obstetric factors such as pre-eclampsia, multiple birth, or gestational diabetes and PPD in this population. This diverges somewhat from prior research reporting that obstetric factors, and gestational diabetes in particular, were associated with modest but significant elevations of PPD risk. 2,16,20,29
In terms of military-specific characteristics, soldiers with higher pay grades had substantially lower risks of developing PPD—in both the total group and among women without a prior history of depression. Previous studies mostly corroborate this finding. Both Nguyen et al. and Nicholson et al. found higher military pay grade to be protective against PPD, although Appolonio & Fingerhut did not find pay grade to be associated with PPD risk. 21,22,30 Our finding that a larger number of prior deployments was associated with elevated rates of PPD also agrees with prior reports 30 and is in contrast to what one might expect from the “healthy warrior effect” wherein healthier SMs are preferentially retained. 31
Our analysis of individuals with no prior history of depression showed that the incidence of PPD diagnosis in the novel onset group was 10.4%, compared with 15.9% for the entire sample. This finding is in line with most previous literature that has robustly found prior depression to be a significant risk factor for PPD. 15,16 An exception is a result from a meta-analysis in which a similar PPD prevalence was reported among mothers without, as compared with those with, psychiatric histories. 32 It is possible that some variability in these associations could exist across different types of populations.
Regarding military factors, high pay grade appeared to have an even stronger protective effect for the novel onset group. Although multiple deployments did not significantly increase risk as it did in the entire sample, the effect size was very similar. Silverman et al. directly compared mothers with and without histories of depression, finding both younger age and certain obstetric factors to be risk factors only associated with the novel onset group. 16 Our analysis, however, did not corroborate these findings. To the best of our knowledge, relatively little prior research has been done on novel onset PPD; this could be a productive avenue in the future.
Our study has a number of strengths. Our study was the first in this population, to our knowledge, to both rely on diagnostic data and to include data both before and during pregnancy. Because diagnostic codes result from clinical encounters and are based on stricter criteria compared with self-report, we would expect our incidence estimates to be conservative. Based on consultation with military mental health care specialists, our study included all of the major depression diagnostic codes, in addition to the ICD-9 code that PPD officially maps to (648.44-Mental disorders of mother, postpartum condition or complication), which is itself quite nonspecific. In our experience, the 648.44 code was very little used by providers in this health system (data not shown) and prior literature has generally used a similar approach to the one that we employed. That being said, it is the case that in prior studies of PPD leveraging diagnostic codes, there has been heterogeneity in ascertainment strategy. 5,21 We used a more expansive set of codes than Nicholson et al., 21 and while we used a slightly more restricted set than that used by Do et al., we did not impose requirements on number of visits or medical clinic type. 5 Our rationale was to maximize specificity by only utilizing codes that were specific to depression and to thereby avoid identifying other phenotypes as outcomes. However, we recognize that some true cases of PPD may have been missed because of these exclusions. Our cumulative incidence is likely a conservative estimate for that reason.
One potential shortcoming one could imagine of relying only on diagnostic codes (versus employing a survey with symptom scales) would be the lack of ability to detect subclinical or as-yet-unreported depression. The concern would then be that the study was only ascertaining those individuals with sufficiently severe symptomatology to seek help.
The U.S. military, however, is charged with providing a comprehensive system enabling early detection of mental health problems. 33 This approach leads to an arguably stronger set of detection capabilities than might be seen in most other systems, leading to robust capture of cases through detectable diagnoses in our data. A key element of the detection system is the presence of a mandatory survey process, the annual Periodic Health Assessment (PHA). It specifically queries each SM each year about the presence of depression and other mental health issues. 34 While the PHA will detect general depression symptoms that SMs choose to report, additional assessment for PPD as a targeted problem is directed within the military health system. 35 The approach is part of clinical practice guidelines within the system.
Furthermore, active-duty SMs are provided free, universal health care; the absence of access barriers may additionally provide more opportunity to detect depression or any diagnosis than in many civilian populations. In addition, most of the Army is in combat-deployable units in which an EMT-trained medic is also stationed, working alongside the SMs daily. These medics are trained in triage of the comprehensive range of problems SMs face, including mental health problems. They will typically report any concerns to unit clinicians, leading to assessments and diagnoses.
As with many studies, we were not able to distinguish PPD from follow-up care for existing depression by looking at the diagnosis code. We also utilized our longitudinal data to examine PPD cases that were apparently new developments following pregnancy. We cannot exclude the possibility that these individuals had received diagnoses prior to 1 year before pregnancy, but it seems likely that PPD diagnoses observed in this group did not reflect ongoing, follow-up care.
It is important to note that the dataset for this study relied on monthly data collection. Accordingly, estimates for gestational age are on the order of months, and thus, in some cases, there may be misclassification of health care events related to the exact timing of depression. That is, it is possible that there is some error in the classification of depression occurring before versus during pregnancy or during pregnancy versus following delivery. In the former case, it is not clear that misclassification before versus during pregnancy would occur in a systematic direction. The net result, we expect, would be conservative effect estimates for each of these predictors.
Misclassification of depression occurring just before delivery (i.e., in the same month) as PPD is more problematic as it would, in our analysis, be classified as a case of PPD. Because many cases of PPD occur in the first weeks following delivery, it is essential to include these cases.
All depression-related care events occurring during the month of delivery were classified as PPD. Therefore, our incidence estimates may be slight overestimates if a substantial fraction of those cases occurred only before delivery and were not also seen for depression following delivery.
An additional consideration is that the incidence rates we observed in our study (2012–2013) may not reflect current circumstances. However, it was important for our study purposes to focus on a time period during which the military context was particularly demanding and 2012–2013 fit that criterion, given the high deployment tempo at that time. Another key secular difference that should be noted comparing our study period with the present would be the change in policy extending maternal leave occurring in 2016, 36 which conceivably could impact PPD as well as service continuation. Until 2016, servicewomen were required to return to work within 45 days (6 weeks) following childbirth; this has since been extended to 91 days (12 weeks). 36
Conclusions
In summary, we found that 15.9% of soldiers on active-duty in the U.S. Army with deliveries in 2012 and 2013 received a diagnosis of PPD. Among those without a prior history of depression, 10.4% of soldiers were diagnosed with PPD. The most important risk factors were a history of mental health diagnoses both before and during pregnancy.
Footnotes
Acknowledgments
The authors gratefully acknowledge data sharing by and support of the U.S. Army Office of the Surgeon General, which have permitted this research to occur. This article was produced by the authors and does not represent the position of the U.S. Army, the U.S. Department of Defense, or the U.S. federal government.
Authors’ Contributions
S.W.: formal analysis (lead), writing—original draft (equal), and review and editing (supporting); J.K.: review and editing (equal); M.L.T.: review and editing (supporting); D.A.N.: data curation (lead) and review and editing (equal); A.D.: original draft (equal); K.W.-B.: conceptualization (supporting) and review and editing (supporting); J.G.S.: conceptualization (supporting) and review and editing (supporting); K.A.S.: conceptualization (supporting) and review and editing (supporting); L.M.K.: conceptualization (lead), data curation (equal), formal analysis (supporting), original draft (equal), and review and editing (equal).
Data Availability
The data used in this study were provided via agreements with the Defense Health Agency and with the U.S. Army Office of the Surgeon General. These agreements preclude us from making the data available.
Authors’ Disclosure Statement
None of the authors have conflicts of interest to disclose.
Funding Information
This research was supported in part by Federal Award No.: