
Abstract
Objective:
To examine trends with a focus on racial and ethnic disparities in reported gestational diabetes mellitus (GDM) and related outcomes (macrosomia, large for gestational age infants) before and during the COVID-19 pandemic in South Carolina (SC).
Methods:
A retrospective cohort study of pregnancies resulting in livebirths from 2015 through 2021 was conducted in SC. Statewide maternal hospital and emergency department discharge codes were linked to birth certificate data. GDM was defined by ICD-9-CM (i.e., 648.01–648.02, 648.81–648.82) or ICD-10-CM codes (i.e., O24.4, O24.1, O24.9), or indication of GDM on the birth certificate without evidence of diabetes outside pregnancy (ICD-9-CM: 250.xx; ICD-10-CM: E10, E11, O24.0, O24.1, O24.3).
Results:
Our study included 194,777 non-Hispanic White (White), 108,165 non-Hispanic Black (Black), 25,556 Hispanic, and 16,344 other race–ethnic group pregnancies. The relative risk for GDM associated with a 1-year increase was 1.01 (95% confidence interval [CI]: 1.01–1.02) before the pandemic and 1.12 (1.09–1.14) during the pandemic. While there were race–ethnic differences in the prevalence of GDM, increasing trends were similar across all race–ethnic groups before and during the pandemic. From quarter 1, 2020, to quarter 4, 2021, the prevalence of reported GDM increased from 8.92% to 10.85% in White, from 8.04% to 9.78% in Black, from 11.2% to 13.65% in Hispanic, and from 13.3% to 16.16% in other race–ethnic women.
Conclusion:
An increasing prevalence of diagnosed GDM was reported during the COVID-19 pandemic. Future studies are needed to understand the mechanisms underlying increasing trends, to develop interventions, and to determine whether the increasing trend continues in subsequent years.
Introduction
The global COVID-19 pandemic caused by SARS-CoV-2 highlighted the extent to which social determinants and inequities impact healthcare received and health outcomes. 1,2 The pandemic caused gaps in healthcare and social services, and widespread isolation due to social distancing. Healthcare access was hindered by clinic cancellations, interruptions in public transportation, financial instability, and self-imposed isolation. Healthcare delivery was also altered with an increase in telemedicine and some changes in diagnostic processes due to a desire to limit in-person contact with patients. In addition, there were widespread changes in lifestyle factors, which likely impacted diet and physical activity. Undoubtedly, these factors profoundly impacted the health and care of pregnant women, many of whom are more economically vulnerable than the overall United States (U.S.) population. 3
Population-based studies investigating the impact of the COVID-19 pandemic on maternal and infant morbidity and mortality in the context of race and ethnic disparities are crucial. In South Carolina (SC) before the COVID-19 pandemic, racial disparities in maternal and infant outcomes were documented, with Blacks/Others having a 2.6-fold greater rate of maternal mortality than Whites (43.3 compared to 16.4 per 100,000 live births) 4,5 and Blacks having a 2.6-fold greater rate of infant mortality compared to Whites (11.7 versus 4.5 per 1,000 live births). 6 Before the COVID-19 pandemic, the prevalence of diabetes during pregnancy, both prepregnancy and gestational (GDM), was increasing. 7 –9 In addition, two hospital studies conducted in Italy 10,11 and one study conducted in the U.S. 12 indicated a potential increase in GDM prevalence associated with pandemic lockdowns. Each of these studies proposed increased maternal stress during lockdowns as a potential mechanism for the reported increase in GDM. 10 –12 Finally, other studies of the pandemic onset also indicated an increase of GDM with the onset of the pandemic. 11,13 –15
Current U.S. clinical guidelines for GDM screening require extensive time at the clinic with a 1-hour oral glucose tolerance test (OGTT) followed by a 3-hour OGTT for those with a positive one-hour screen. 16 , 17 It is not known whether or how diagnoses of GDM were altered during the early phases of the pandemic when in-person visits were minimized to reduce transmission of SARS-CoV-2. It is also not known how care for patients identified to have GDM may have changed during the pandemic. The pandemic also likely impacted lifestyle factors, including diet and physical activity levels related to both GDM onset and outcomes.
The southeastern U.S. has one of the highest rates of obesity and diabetes, and poor maternal and infant outcomes in the nation with persistent racial and ethnic disparities. 5,9,18 The southeastern U.S. and minority populations are disproportionately impacted by diabetes, 18 as well as diabetes during pregnancy. 9,19,20 The onset of the COVID-19 pandemic likely impacted GDM risk factors, its diagnosis, and treatment. Therefore, our objective was to examine trends with a focus on racial and ethnic disparities in reported GDM and two closely related birth outcomes, namely macrosomia and having a large for gestational age (LGA) infant, before and during the COVID-19 pandemic in SC from January 2015 to December 2021.
Methods
Study design and population
A retrospective cohort study of pregnancies resulting in live births from 2015 through 2021 was conducted. The eligible sample population included SC resident mothers with live singleton or twin births, who delivered between January 2015 and December 2021. Birth certificate information was obtained from the SC Department of Health and Environmental Control and linked by the SC Revenue and Fiscal Affairs (RFA) Office to inpatient hospital discharge records, emergency department (ED) records, and the Medicaid eligibility file. These included maternal and infant inpatient and ED procedure and diagnostic codes. The linkage between databases is based on an algorithm developed by SC RFA, which relies on personal identifying information. Both maternal and offspring IDs are assigned across databases. Linked birth certificate, inpatient, ED, and Medicaid eligibility files were available from 2012 to 2021. The Institutional Review Board of the Medical University of South Carolina approved the study as exempt research.
Main exposure variable definitions
Time was defined based on quarter with respect to calendar time when a pregnancy delivery occurred. Race and ethnicity were viewed as social constructs based on self-identity. We use the terms Black, Hispanic, and White to refer to individuals who self-identify as non-Hispanic Black, Hispanic/Latina, and non-Hispanic White, respectively. Maternal race/ethnicity was defined based on the most common report across data sources, or when Hispanic ethnicity was identified three or more times, participants were classified as Hispanic/Latina regardless of the most common report. Race and ethnicity were self-reported to the extent where policies to obtain self-reported data on the birth certificate and for administrative data were followed.
Outcome definition
GDM and prepregnancy diabetes were defined as reported on the birth certificate or inpatient hospital or ED discharge codes. Records were available for at least 3 years before each pregnancy. Once a woman was identified as having prepregnancy diabetes ([International Classification of Diseases, Ninth/Tenth Revision, Clinical Modification] ICD-9-CM, 250.xx; ICD-10-CM, E10, E11, O24.0, O24.1, O24.3), they were considered to have diabetes and not eligible to develop GDM (ICD-9-CM, 648.01–648.02, 648.81–648.82; ICD-10-CM, O24.4, O24.1, O24.9). Diabetes reported during the first trimester was considered prepregnancy diabetes. Diabetes first reported during the second or third trimester was considered GDM.
Covariate definitions
Education (categorized based on less than high school graduate; high school graduate/General Educational Development (GED); high school graduate and some college; and a college degree or more); rural versus urban residence; receipt of Women, Infants & Children (WIC) during pregnancy; tobacco use during or prepregnancy; plurality (twin versus singleton); previous preterm births; and maternal prepregnancy weight and height were defined as reported on the birth certificate. Based on maternal body mass index (BMI), women were classified as underweight (14.0–18.4 kg/m2), normal (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), or obese (≥30 kg/m2). Being firstborn was based on birth certificate report of being the first live or stillborn infant. Use of Medicaid was defined based on eligibility within two months of delivery based on a statewide Medicaid eligibility file. Prepregnancy hypertension was defined based on inpatient hospital or ED discharge records (ICD-9-CM, 642.2, 642.9; ICD-10-CM, O10, O11), or the birth certificate indicating prepregnancy hypertension. Once a woman was identified as having prepregnancy hypertension, she was always considered to have prepregnancy hypertension.
Birthweights inconsistent with gestational age were identified based on a modified version of the criteria published by Alexander et al., which allowed for a birthweight up to 6500 g at a gestational age of 39 weeks, and 7000 g at a gestational age of 40–44 weeks. 21 LGA infants were based on the 90th percentile of weight for gestational age and limited to infants with plausible birthweights for their gestational age, according to growth curves derived using a U.S. national reference based on births in 2009–2010. 22 The same standard growth curve was used across all race–ethnic groups to define LGA. Macrosomia was defined as a birthweight of ≥4500 g. 23
Statistical analysis
Kruskal–Wallis and chi-square tests were used to examine bivariate associations between sociodemographic, lifestyle, and clinical characteristics, and outcomes of interest for pregnancies before and during the COVID-19 pandemic (i.e., 2015 through quarter 1, 2020; quarter 2, 2020 through 2021) and by maternal race–ethnic group (White, Black, Hispanic, and Other). The main exposure variables were time and race–ethnic group.
Generalized linear models with a modified Poisson, with a log link, were used to estimate the risk of pregnancies with GDM, macrosomia, and LGA infants. 24 –26 To express estimates as risk ratios, modified Poisson models were used because log-binomial models encountered convergence issues due to data sparseness. 25,26 Generalized estimating equations with exchangeable working correlation were used to account for repeated pregnancies among mothers. 27 To accommodate changes in trends, a predetermined change point was included in the models, quarter 1 of 2020 (i.e., March 31, 2020). To examine associations between race–ethnicity group and trends over time, appropriate interaction terms were included. Covariates included in our models were identified a priori. Three models were fitted for each outcome: (1) an unadjusted model that included time modeled across quarters with a single change point at quarter 1 of 2020, the main effect for race–ethnicity, and an interaction term between time and race–ethnicity, (2) a model that further included sociodemographic factors (age, education level, rural residence, Medicaid eligibility and WIC benefits during pregnancy), and (3) a model that additionally adjusted for lifestyle and clinical variables depending on the outcome of interest. Figures for each of the outcomes are based on Model 1. p-values of 0.05 and corresponding 95% confidence intervals (CIs) were used to determine statistical significance. Less than 0.2% of data were missing on any of the outcome variables and less than 2.0% of data were missing from any of the multivariable adjusted models. Analyses were conducted in SAS (SAS Institute, Cary, NC) and R (R Core Team, 2021) software.
Results
During the study period, 264,371 mothers had 344,842 pregnancies, which resulted in a live singleton or twin birth (Fig. 1). Analyses of macrosomia and LGA were limited to live singleton pregnancies (260,415 mothers; 338,784 pregnancies). All mothers had at least some information available from the linked inpatient hospital and ED procedure and diagnostic code file.
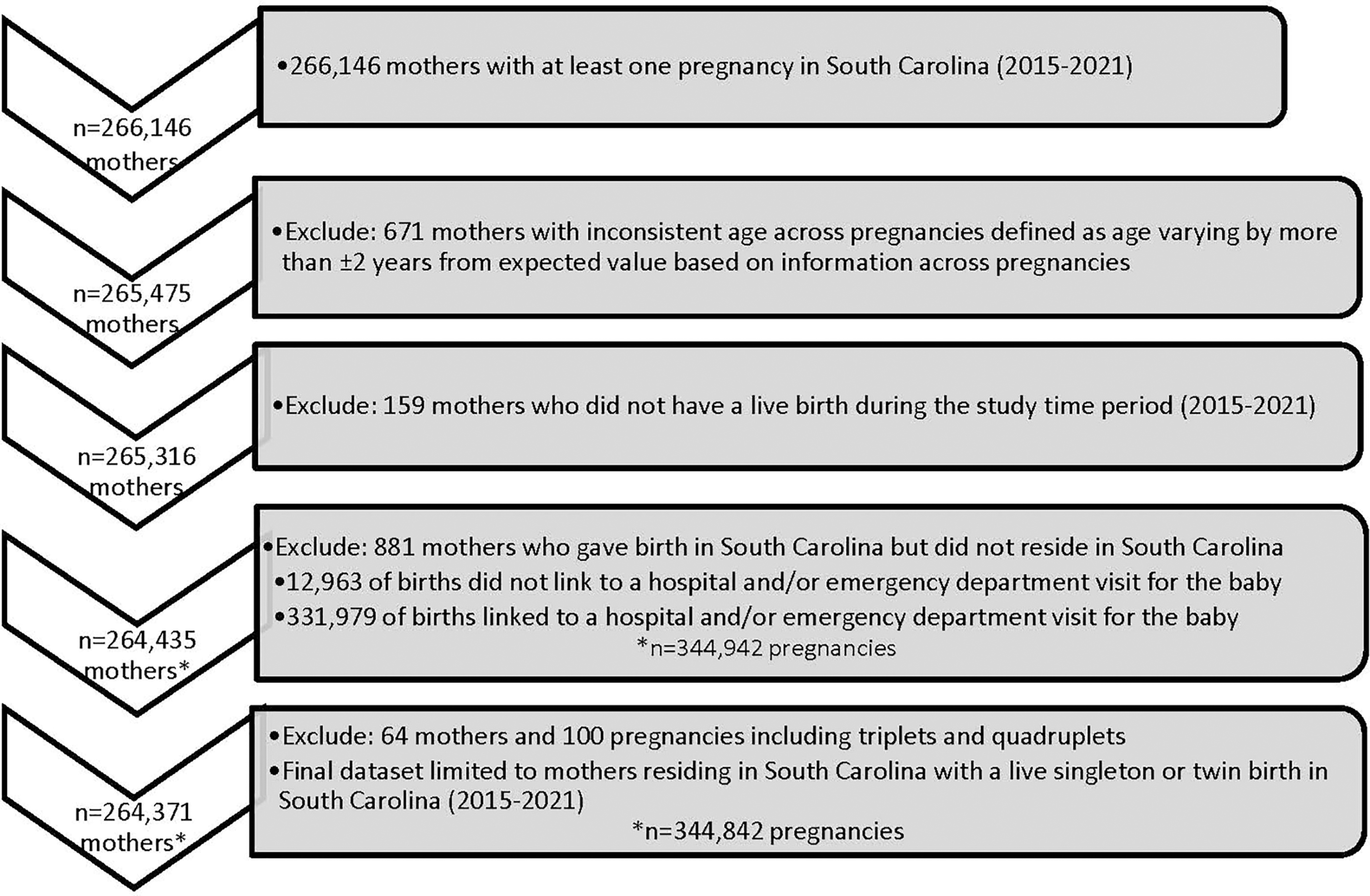
Consort diagram.
Characteristics of 344,842 pregnancies are found in Table 1, stratified by before and after March 31, 2020. The mean age at delivery before the pandemic was 27.8 years compared with 28.4 years after the pandemic. Medicaid eligible pregnancies increased from 50.9% before the pandemic to 57.9% after the pandemic, while receipt of WIC benefits declined from 42.5% to 32.5%. Report of tobacco use either during or prepregnancy also declined from 12.8% to 8.8%, while prepregnancy obesity prevalence increased from 32.1% to 35.5%. Characteristics of pregnancies stratified by maternal race–ethnic group are found in the Supplementary Table S1.
Characteristics of 344,842 Pregnancies Resulting in a Live Singleton or Twin Birth in South Carolina, 2015–2021, Stratified by before and after the 2020 Quarter 1 Change Point
Missing values—maternal education, 1068; tobacco use, 238; firstborn, 91; prepregnancy BMI, 4,389; macrosomia, 22; large for gestational age, 616.
p-values were determined using chi-square for categorical variables and Kruskal–Wallis test for continuous variables.
Race and ethnicity were viewed as social constructs based on self-identity. We use the terms Black, Hispanic, and White to refer to individuals who self-identify as non-Hispanic Black, Hispanic/Latina, and non-Hispanic White, respectively.
BMI, body mass index, kg/m2; GED, General Educational Development; WIC, Women, Infants & Children.
Regression Models Predicting Gestational Diabetes among Live Singleton and Twin Pregnancies in South Carolina, 2015–2021
For modeling purposes the change point is defined as the first quarter of 2020.
Race and ethnicity were viewed as social constructs based on self-identity. We use the terms Black, Hispanic and White to refer to individuals who self-identify as non-Hispanic Black, Hispanic/Latina, and non-Hispanic White, respectively.
BMI, body mass index; GED, General Educational Development; WIC, Women, Infants & Children.
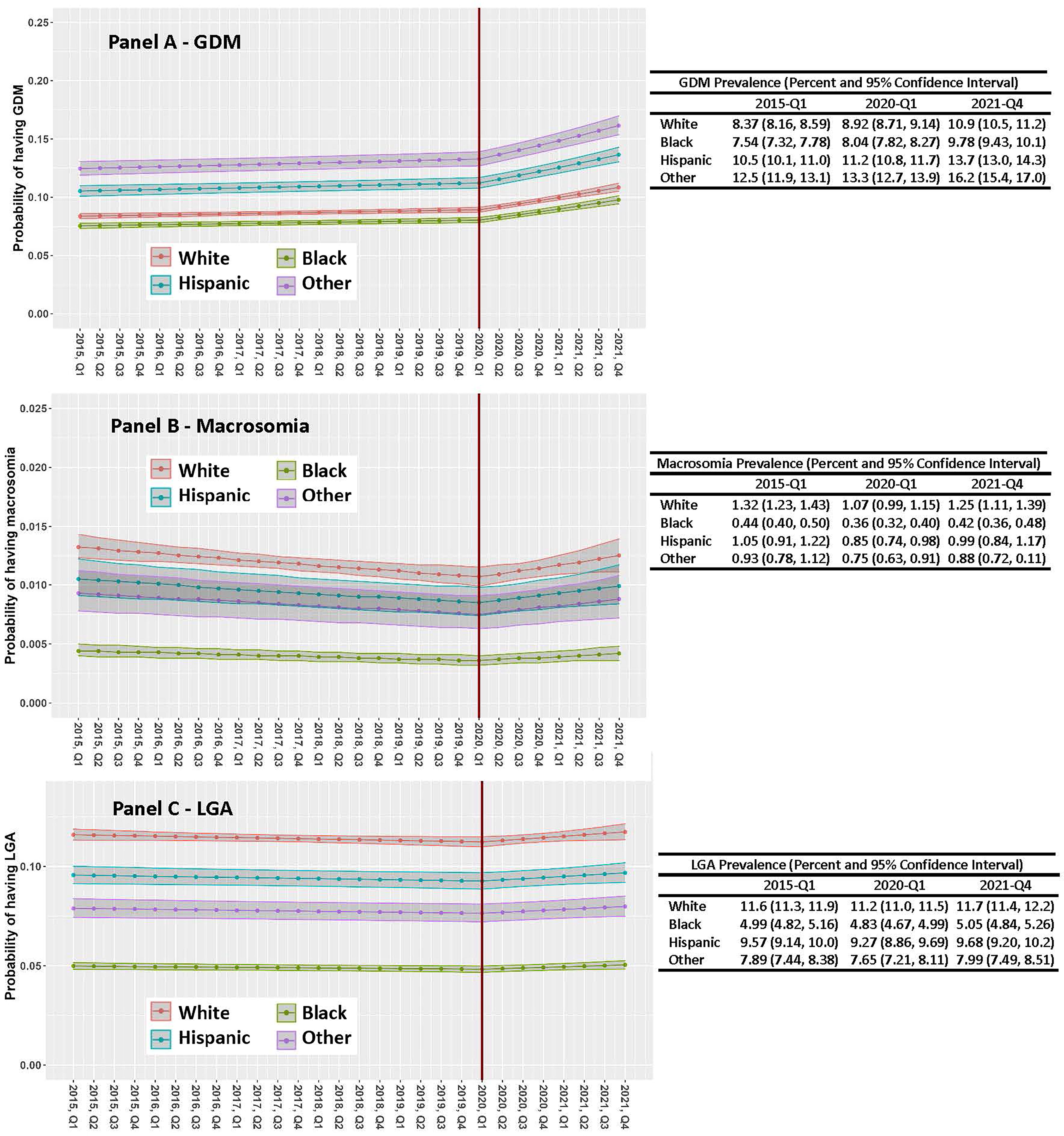
While the prevalence of reported GDM was increasing before the pandemic from 2015 through the first quarter of 2020, its rate of increase accelerated at the onset of the pandemic through 2021 (Fig. 2 Panel A). The relative risk (RR; 95% CI) for having GDM associated with a 1-year increase in time was 1.01 (1.01–1.02) before the pandemic and 1.12 (1.09–1.14) after the pandemic started. Moreover, while there were race–ethnic differences in the prevalence of GDM, trends were similar across all race–ethnic groups both before and after the onset of the pandemic, as shown in Fig. 2 Panel A (p-values for the interaction between time and race–ethnic group were nonsignificant [before, p = 0.0983 and during, p = 0.1786]). Adjusting for sociodemographic factors, including maternal age, education level, Medicaid eligibility, receipt of WIC services during pregnancy, and rural versus urban residence, attenuated trends only slightly, as did further adjustment for lifestyle and clinical factors (tobacco use, firstborn, twin pregnancy, previous preterm birth, prepregnancy BMI category, and prepregnancy hypertension). Factors most strongly associated with increased risk of GDM included Other race–ethnicity (RR = 1.49 [1.42–1.55]), maternal age (RR = 1.07 [1.07–1.07]), being overweight (RR = 1.59 [1.54–1.64]) or obese (RR = 2.61 [2.54–2.69]) prepregnancy, and having a history of prepregnancy hypertension (RR = 1.37 [1.33–1.31]).
Regression Models Predicting Macrosomia and Large for Gestational Age Infants among Live Singleton Pregnancies in South Carolina, 2015–2021
For modeling purposes, the change point is defined as the first quarter of 2020.
Race and ethnicity were viewed as social constructs based on self-identity. We use the terms Black, Hispanic and White to refer to individuals who self-identify as non-Hispanic Black, Hispanic/Latina, and non-Hispanic White, respectively.
BMI, body mass index; GED, General Educational Development; WIC, Women, Infants & Children.
While the prevalence of macrosomia was decreasing before the pandemic, its prevalence increased from the onset of the pandemic through 2021 (Fig. 2 Panel B). The RR (95% CI) for delivering an infant with macrosomia associated with a 1-year increase in time was 0.96 (0.94–0.98) before the pandemic and 1.09 (1.01–1.18) after the pandemic started. Moreover, while there were race–ethnic differences in the prevalence of macrosomia, trends were similar across all race–ethnic groups both before and after the onset of the pandemic, as displayed in Fig. 1 Panel B (p-values for the interaction between time and race–ethnic group were nonsignificant [before, p = 0.6079 and during, p = 0.8714]). Adjusting for sociodemographic factors accentuated downward trends before the pandemic slightly, and slightly attenuated upward trends after the pandemic as did further adjustment for lifestyle and clinical factors (tobacco use, firstborn, previous preterm birth, prepregnancy BMI category and prepregnancy hypertension, prepregnancy diabetes, and GDM). Factors most strongly associated with increased risk of macrosomia included being overweight (RR = 1.99 [1.79–2.20]) or obese (RR = 3.09 [2.81–2.40]) prepregnancy, and having prepregnancy (RR = 3.81 [3.27–4.43]) or gestational (RR = 1.76 [1.59–1.94]) diabetes. Factors most strongly associated with a decreased risk of macrosomia included being a Black woman (RR = 0.29 [0.26–0.33]), tobacco use (RR = 0.60 [0.52–0.69]) during or prepregnancy, and being underweight prepregnancy (RR = 0.31 [0.19–0.52]).
The prevalence of having an LGA infant was stable before and after the pandemic’s onset (Fig. 2, Panel C). The RR (95% CI) for having an LGA infant associated with a 1-year increase in time was close to the null value both before (RR = 0.99 [0.99–1.00]) and after (RR = 1.03 [1.00–1.05]) the pandemic started. Moreover, while there were race–ethnic differences in the risk of having an LGA infant, trends were similar and null across all race–ethnic groups both before and after the onset of the pandemic, as shown in Fig. 1 Panel C (p-values for the interaction between time and race–ethnic group were nonsignificant [before, p = 0.2711 and during, p = 0.2330]). Adjusting for sociodemographic factors did not alter trends, while adjustment for lifestyle and clinical factors (tobacco use, firstborn, previous preterm birth, prepregnancy BMI category and prepregnancy hypertension, prepregnancy diabetes, and GDM) resulted in a slight downward trend before the pandemic (RR = 0.98 [0.97–0.99]). Factors most strongly associated with an increased risk of having an LGA infant included being overweight (RR = 1.51 [1.47–1.56]) or obese (RR = 1.98 [1.92–2.03]) prepregnancy, and having prepregnancy (RR = 2.63 [2.50, 2.77]) or gestational (RR = 1.51 (1.47–1.56]) diabetes. Factors most strongly associated with a lower risk of having an LGA infant included being a Black woman (RR = 0.40 [0.39–0.41]) or woman of Other race–ethnicity (RR = 0.67 [0.63–0.71]), tobacco use (RR = 0.68 [0.52–0.69]) during or prepregnancy, and being underweight prepregnancy (RR = 0.56 [0.50, 0.62]).
Discussion
Our results indicate that, while reported prevalence of GDM was increasing before the COVID-19 pandemic in SC, its rate of increase accelerated at the onset of the pandemic. We also report that while the prevalence of macrosomia defined as a birthweight of ≥4500 g was decreasing before the pandemic, its prevalence increased from the onset of the pandemic through 2021. In contrast, we report that the prevalence of having an LGA infant was relatively stable before and after the pandemic’s onset. In addition, for each outcome, we report consistent trends over time across the four racial–ethnic groups examined with marked racial and ethnic differences in the absolute risk of GDM, macrosomia, and having an LGA infant.
Importantly, at the population level, threats such as the COVID-19 pandemic often have an amplified impact on childbearing women and infants, which perpetuates vulnerability across generations. There is robust support from decades of animal and epidemiological studies for the developmental origins of health and disease hypothesis pertaining to adiposity 28,29 and obesity, 30,31 as well as cardiovascular disease risk. 32,33 This hypothesis maintains that gestational programming may critically influence adult health and disease. 32,34 –36 Gestational programming is a process whereby stimuli or stressors that occur at critical or sensitive periods of development permanently change the structure, physiology, and metabolism of fetuses, predisposing them to disease in adult life. Hence, a change in the prevalence of GDM and its sequala could have long-lasting implications for the offspring. This study provides important population-level information on the prevalence of GDM and two closely related birth outcomes (macrosomia and being born LGA) during the pandemic.
Proposed mechanisms for the increase in GDM associated with the pandemic’s onset include the following: (1) changes in access to care, care delivery modalities, and GDM diagnostic practices; (2) increased stress associated with financial instability, self-imposed isolation, mandated isolation, and other pandemic-related experiences; (3) changes in lifestyle factors, including dietary patterns and physical activity levels; or (4) another mechanism unrelated to the COVID-19 pandemic. Two Italian studies and one U.S. study, each based on single hospitals with documented consistent GDM testing before and during the pandemic, reported higher rates of GDM during the pandemic period. The two Italian studies hypothesized that increased stress due to the mandated lockdown could be the mechanism resulting in increased rates of GDM among their relatively lean cohorts. 10,11 Obesity levels were higher in the U.S. study than in the two Italian studies, and the U.S. study indicated that, while the prevalence of GDM was higher during the pandemic, gestational weight gain among those with GDM was similar before and during the pandemic. The Italian and U.S. studies propose maternal stress as a potential contributor to gestational hyperglycemia. 12 Moreover, changes in maternal prepregnancy BMI do not appear responsible for the increased rates of GDM in this study because adjustment for maternal prepregnancy BMI levels in model 3 does not substantially alter the associations of interest.
Our finding of increased rates of macrosomia with the onset of the pandemic is consistent with the hypotheses that true increases in the prevalence of GDM were observed and/or that treatment of GDM during the pandemic was less effective. Given the high reported prevalence of GDM in our population-based study, 10.9% in White, 9.8% in Black, 13.7% in Hispanics, and 16.2% in women in the Other race–ethnic group at the fourth quarter of 2021, it is important to determine what factors during the pandemic contributed to increasing rates. Findings of higher GDM prevalence in women in the Other racial–ethnic group and Hispanics, as well as lower levels of GDM in Black women are consistent with prior studies. 7,8 The cause of racial–ethnic differences and the extent to which social determinants of health may be responsible for disparities are not known. The extent to which screening, detection, and treatment of GDM may reduce future risk of type 2 diabetes is also not known, 37 but is important to consider given the increasing trend in GDM.
One limitation of our study is the use of administrative databases and reliability of data obtained from these databases. Prior validation studies have been conducted with the general finding that reported diabetes during pregnancy is relatively accurate with few false positives. 38 –40 Moreover, birth certificates and administrative data continue to be important sources of data. 7,8,38 –41 Our study had the ability to longitudinally interlink vital status with inpatient hospital discharge and ED visit data at the state level. Hence, we were able to follow SC women over time through multiple pregnancies, inpatient hospital visits, and ED visits. Due to changes in prenatal care before and during the pandemic, the known correlation between diabetes during pregnancy and prenatal care, and the questionable quality of data from the birth certificate pertaining to prenatal care, we did not adjust for timing and consistency of prenatal care in our analyses. A strength of our study is that because we were able to follow women over time using an integrated dataset that included vital records and inpatient hospital discharge and ED visit data, we were able to differentiate between prepregnancy diabetes and GDM. However, the potential for miscoding between prepregnancy and GDM remains. There was also the potential of miscoding for race and ethnicity viewed as social constructs based on self-identity. While birth certificate and administrative data should rely on self-reported race and ethnicity, we noted discrepancies across sources in data capture and reporting. We also elected not to include information on fetal deaths. Finally, lack of data on other covariates, including maternal diet, physical activity, stress levels, procedures, and glucose levels pertaining to diagnosis of GDM and HbA1c levels throughout pregnancy, were also limitations.
We report an increasing prevalence of GDM and macrosomia following the onset of the COVID-19 pandemic. While the prevalence of reported GDM is impacted by screening, diagnostic, and reporting practices, as well as actual changes in prevalence over time, the reported increasing trend in GDM and macrosomia during the COVID-19 pandemic is notable. Potential explanations impacting actual changes in prevalence include changes in lifestyle factors (i.e., diet and exercise) and stress (i.e., social isolation, financial instability, transportation). Future studies are needed to understand the mechanisms underlying this increasing trend and to develop interventions targeting identified causal mechanisms.
Footnotes
Authors’ Contributions
K.J.H. and A.M.M. conceived and designed the study, researched data, analyzed and interpreted data, wrote the article, reviewed and edited the article, and supervised the study. C.W., B.N., D.A.W., K.C., S.S., and J.E.K. analyzed and interpreted data, wrote the article, and reviewed and edited the article. J.M., J.P., and H.F. interpreted data and wrote the article. All authors were involved in writing the article and had final approval of the submitted and published versions.
Author Disclosure Statement
The authors declare no conflict of interests.
Funding Information
This work was supported by the National Institutes of Health (NIH)
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.