
Abstract
Objective:
To determine subclinical cardiovascular disease (sCVD) in middle-aged women with clinically manifested hand osteoarthritis (HOA) and to improve the characterization of cardiovascular risk in this population.
Design:
We cross-sectionally evaluated the relationship between HOA and sCVD in 1,803 volunteers from the Mexican Teachers’ Cohort. From 2012 to 2016, a subsample from Mexico City, the Northern state Nuevo León, and the Southern states Chiapas and Yucatán was invited for clinical evaluations, during which neurologists examined carotid arteries using ultrasound, and a standardized HOA questionnaire was also administered. HOA was defined as age ≥45 years, hand joint pain, and morning stiffness that lasted no longer than 30 minutes. sCVD was assessed using the intima-media thickness (IMT) and atherosclerotic plaques.
Results:
Among participants with a mean age of 51 years (±4), 18.4% met the criteria for HOA, and the prevalence of carotid atherosclerosis was 23.1%. After multivariable adjustment, women diagnosed with HOA had a 1.8% (95% confidence interval [CI] 0.3, 3.3) greater mean IMT than those without this joint disease. Similarly, women with HOA had 36% (95% CI 1.01, 1.84) higher odds of carotid atherosclerosis.
Conclusions:
HOA is associated with sCVD in middle-aged women. This relationship might be due to low-grade chronic inflammation; however, further research is required to clarify the underlying mechanisms.
Introduction
Osteoarthritis (OA) is a clinical syndrome characterized by joint pain and different degrees of functional limitation, with heterogeneity in both localization and progression, 1 and an inflammatory component that affects articular cartilage, subchondral bone, and synovial tissue.
OA continues to increase owing to population aging and longer life expectancy, resulting in a high impact on years lived with disability 2 and increasing societal costs. 3
In 2019, ∼528 million people worldwide were living with OA; an increase of 113% since 1990; 60% are female. 4
North America has the highest regional prevalence of OA (5,924 per 100,000 individuals). 5
Over 30 million cases of clinical OA have been calculated in the United States between 2008 and 2011. 6 . However, estimates differ according to case definition 7 and localization of the joints affected, with hip, knee, and hand being the most prevalent. 8 –10 Among those typical body sites, a systematic review has found that the hand is the least studied. 7
Many studies have shown that patients with rheumatic diseases have an increased risk of cardiovascular disease (CVD). 11
Some authors have reported atherosclerosis related to hand osteoarthritis (HOA); the latter has been defined both radiologically and photographically. Specifically, for OA, some pathways have been described, such as shared (vascular) risk factors, chronic inflammation, physical disability, and anti-inflammatory and/or analgesic medication. 12 However, compared with knee and hip OA, 13 the hand seems to be a separate subset of the disease as far as genetic factors, pathogenesis, and disease course are concerned. 14,15
Jonsson et al 16 took hand photographs and measured carotid intima-media thickness (cIMT) and coronary calcium, establishing a linear association between the severity of HOA and atherosclerosis, but not cardiovascular events, in older women, but not in men.
Koutroumpas et al 17 used hand radiography and common carotid and femoral artery ultrasonography and found evidence of subclinical atherosclerosis and endothelial dysfunction in patients with erosive HOA.
Haugen et al 18 assessed HOA using radiographs and information about joint pain, mortality, and cardiovascular events and found that symptomatic HOA, but not radiographical HOA, was associated with an increased risk of coronary events.
Provan et al 19 found that hand osteophytes were associated with the pulse pressure augmentation index, an indirect marker of vascular disease.
A recent systematic review found an association between vascular pathology and the risk of HOA, suggesting that narrow arterioles in the synovium may result in localized decreased blood flow that may initiate osteoclastic resorption, alter subchondral bone integrity, and lead to reduced bony support for overlying cartilage, resulting in cartilage damage. 20
Progressive subclinical arterial wall alterations precede cardiovascular clinical events, which reflect advanced atherosclerotic disease. cIMT has been proposed as a tool to aid cardiovascular risk stratification as it comprises a direct measure of atherosclerosis, is associated with future cardiovascular events, and is a safe, inexpensive, and widely available technique when compared with other cardiovascular assessment methods such as coronary artery calcium score or cIMT by magnetic resonance imaging. 21 cIMT and carotid artery plaque provide surrogate endpoints of cardiovascular outcomes in many clinical trials evaluating the efficacy of cardiovascular risk factor modification. 22 –25
Different joints are susceptible to different risk factors of vascular pathology. Emerging evidence proposes obesity-associated inflammation as the main pathophysiological mechanism in knee and hand joints, as opposed to alterations in bony shape in hip OA. 20 Therefore, through the measurement of cIMT, we aimed to determine subclinical (sCVD) in women with clinically manifest HOA to help characterize cardiovascular risk in this population. 21
Materials and Methods
Study population
We used data from the Mexican Teachers’ Cohort (MTC), a prospective study of 115,315 female teachers aged ≥25 years that began in 2006 when participants responded to a baseline questionnaire on demographic and reproductive characteristics, lifestyle, and medical conditions. The study participants were public school teachers from 12 geographically and economically diverse states in Mexico.
Between September 2012 and June 2017, a random sample of 4,233 MTC participants from four states (Chiapas, Yucatán, Monterrey, and Mexico City) aged 40 years and older living within a 50 km radius of clinical sites were invited for clinical examinations and laboratory assessments as part of an ancillary study on cardiovascular disease. Approximately 60% (n = 2,615) of the invited participants provided written informed consent.
For the purpose of this analysis, women aged <45 years (n = 354), those who did not complete the supplementary questionnaire’s corresponding HOA section at the clinical visit (n = 110), those who did not have complete cIMT measurements (n = 246), and those with prevalent myocardial infarction, stroke, rheumatoid arthritis, or other rheumatological autoimmune diseases (n = 102) were excluded. Therefore, the final sample for this study comprised 1,803 women (Fig. 1).
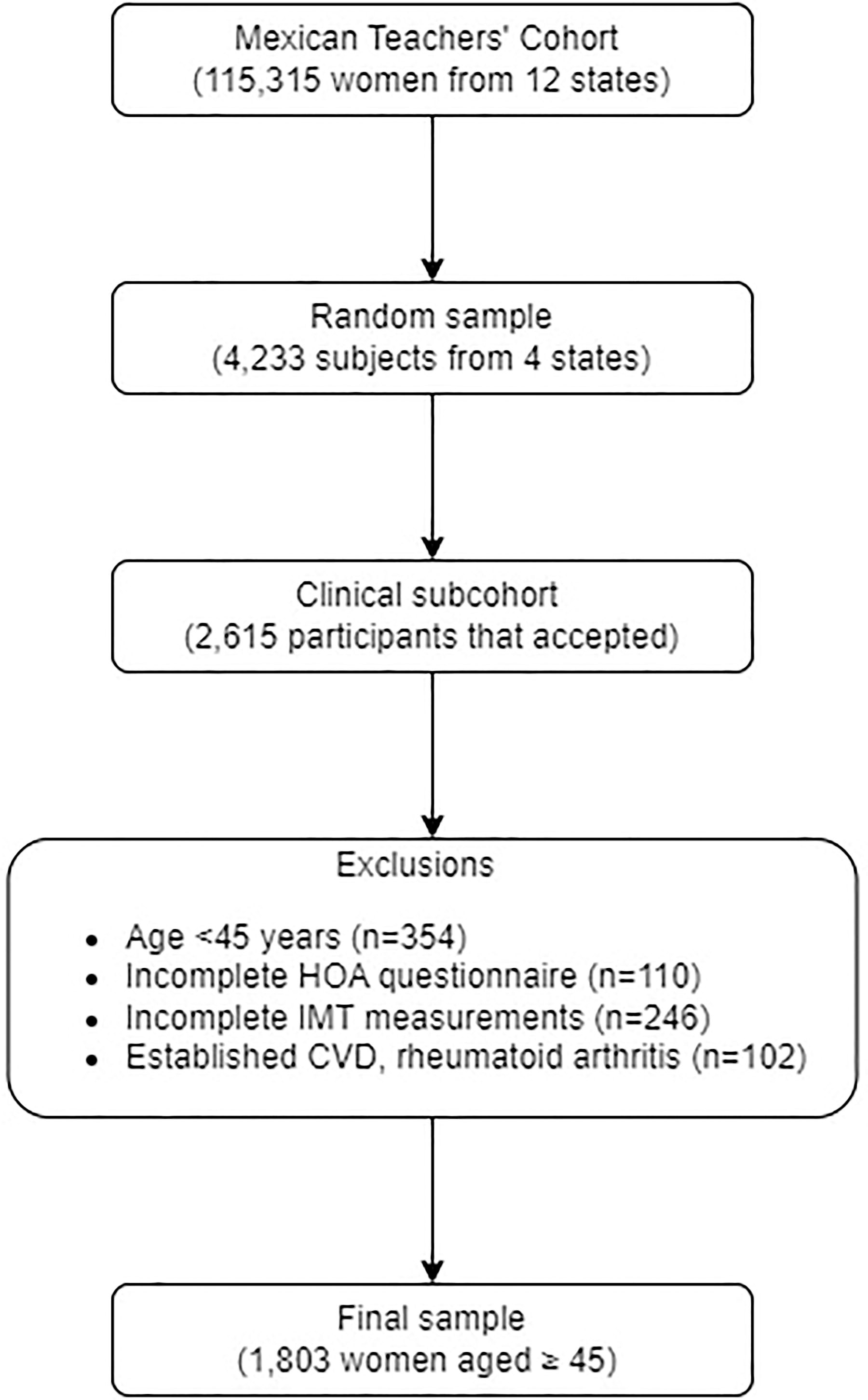
Sampling flow diagram. CVD, cardiovascular disease; HOA, hand osteoarthritis; IMT, intima-media thickness.
The study was approved by the Research Ethics Committee of the National Institute of Public Health (approval ID 947).
Assessment of clinical hand osteoarthritis
We determined the presence of HOA during the clinical visit using three self-reported items based on the 2008 United Kingdom National Institute for Health and Care Excellence (NICE) diagnostic criteria for HOA: 26 –28 “Do you have pain in the hands?” (Yes/No); “Do you wake up with stiff hands (when you wake up do you have trouble moving your hands)?” (Yes/No); and “How many minutes does it take to feel your hands without stiffness?.” We defined HOA as having an age of 45 years or older, hand joint pain, and morning stiffness lasting no more than 30 minutes, with no previous diagnosis of autoimmune rheumatologic disease.
Covariates
Covariate information was based on the MTC’s baseline and follow-up questionnaires administered in 2008 and 2011, respectively, and information was collected during the clinical visits. The baseline questionnaire collected information on education level, health insurance, and whether the participants or their parents spoke indigenous language. We asked them about the weekly hours spent doing moderate (i.e., riding a bike, dancing, and hiking) or vigorous (i.e., swimming and running) recreational physical activity as well as moderate (i.e., cleaning windows, scrubbing bathrooms and floors, and washing clothes by hand) or vigorous (i.e., carrying heavy bags from the market, moving furniture, and moving heavy boxes) daily activities, providing eight possible answers (from none to ≥10 hours/week) for each category. Smoking and drinking statuses were determined using self-reported data.
At clinical sites, interviews were conducted, self-reported questionnaires were distributed, and anthropometry, blood pressure measurements, and blood tests were performed. Prequalified and uniformly trained research staff measured weight with an electronic digital scale (Tanita Corp; Arlington Heights, Illinois, USA) to the nearest 0.1 kg and height with a wall stadiometer (Seca Corp; Hamburg, Germany) to the nearest millimeter. For diabetes, hypertension, and hypercholesterolemia, we used the self-reported diagnosis and treatment of the disease from questionnaires and updated the information collected at the clinical site. We also used clinical information obtained from the study sites for diagnosis. Blood pressure measurements were collected automatically by placing cuffs on the four extremities (VaSera VS-1000; Fukuda Denshi, Tokyo, Japan). Eight-hour fasting blood samples were drawn through venipuncture and processed within 30 minutes to measure plasma concentrations of glucose, total cholesterol, and high-density lipoprotein (HDL) cholesterol in the clinical laboratory at each site using standard assays. Women were classified as having diabetes if their fasting plasma glucose level was ≥126 mg/dL. In addition, fasting plasma total cholesterol ≥240 mg/dL or LDL cholesterol ≥160 mg/dL was used to determine whether the participant had hypercholesterolemia. Women with a systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg were considered hypertensive.
Subclinical cardiovascular disease
Subspecialty trained vascular neurologists used SonoSite™ MicroMaxx™ ultrasound and Asus™ laptop with M’AthStd Software™ (Intelligence in Medical Technologies, Paris, France) to measure cIMT and identify atherosclerotic plaques. Following the Mannheim Carotid Intima-Media Thickness and Plaque Consensus, 29 both common carotid arteries were measured with the patients in a supine position, with their heads rotated 0° to 30°. cIMT was measured between the lumen–intima and media–adventitia interfaces on the far wall of the common carotid artery, at least 5 mm below its end, where the carotid bifurcation was visible using a 10 mm arterial segment, and the overall mean was calculated. If the neurologist could not obtain an adequate image, the procedure was repeated on the near wall. Focal structures protruding at least 0.5 mm into the lumen, 50% greater in thickness relative to the surrounding cIMT, or greater than 1.5 mm were considered atherosclerotic plaques. We repeated the measurements among 147 women in our study to assess reproducibility and found it to be high (r = 0.89 (95% confidence interval [CI] 0.84, 0.93) for Chiapas and r = 0.92 (95% CI 0.86, 0.96) for Yucatán. We defined carotid atherosclerosis (CAS) as mean left or right cIMT ≥0.8 mm or the presence of plaque.
Statistical analysis
The cIMT was positively skewed; therefore, we used log transformation to normalize the distribution. 30 Age- and multivariable-adjusted linear regression models were used to estimate the percentage differences in the mean cIMT and 95% CIs (significance level 0.05) according to the presence of HOA. We used logistic regression models to estimate age- and multivariable-adjusted odds ratios (ORs) and 95% CIs (significance level 0.05) of CAS comparing women who met the criteria for HOA with those who did not. Multivariable models included traditional vascular risk factors, such as age, smoking status, alcohol intake, diabetes, hypertension, and hypercholesterolemia. We conducted additional analyses adjusting for other potential confounders, such as the “mechanical” factors of body mass index, total intensity exercise, and total daily activities. Finally, we considered the study site, educational level, and health insurance as surrogates of socioeconomic status and indigenous ethnicity in our models.
We performed a sensitivity analysis by changing the definition of HOA proposed by the 2014 NICE1 guidelines, specifically, as age ≥45 years, hand joint pain, and no morning joint-related stiffness or morning stiffness no longer than 30 minutes. We explored alternative definitions of cIMT and CAS as well as an indigenous subgroup analysis as complementary sensitivity analyses. All the analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
The mean age of the participants was 51.0 ± 4.3 years, and the prevalence of HOA was 18.4% (n = 333). The mean cIMT was 0.686 ± 0.095 mm, and the prevalence of CAS was 23.1% (n = 416). The baseline characteristics according to the HOA diagnosis are presented in Table 1. The prevalence of past smoking, diabetes, hypertension, and hypercholesterolemia was higher among women who met the HOA criteria than among those who did not.
Characteristics of 1,803 Women from the Mexican Teachers’ Cohort by Diagnosis of Hand Osteoarthritis (HOA) according to the NICE 2008 Definition
SD, standard deviation.
The mean cIMT was significantly higher in women with HOA (0.702 ± 0.101 mm) than in those without (0.686 ± 0.095 mm). After adjusting for age, clinical site, smoking, alcohol consumption, hypertension, hypercholesterolemia, diabetes, body mass index, total intensity exercise, total daily activities, health insurance, and indigenous ethnicity, we observed an association between HOA and cIMT (Table 2). The mean carotid intima-media layer was 1.8% thicker (95%CI 0.3, 3.3) in women with HOA compared with those without HOA.
Adjusted Differences in Mean Carotid Intima-Media Thickness (cIMT) and Adjusted Odds Ratios for Carotid Atherosclerosis (CAS), Comparing Women with and Without Hand Osteoarthritis (HOA) According to the NICE 2008 Definition
Model 2: model 1 + clinical site + smoking + alcohol consumption + hypertension + hypercholesterolemia + diabetes.
Model 3: model 2 + body mass index + total intensity exercise + total daily activities.
Model 4: model 3 + health insurance + indigenous ethnicity.
Similarly, we observed a higher prevalence of CAS in women with HOA (27.6 vs 22.0%). After adjusting for demographic characteristics and risk factors common to HOA and CAS, women who had HOA had 36% higher odds of CAS than those without HOA (95% CI 1.01, 1.84) (Table 2).
When we repeated our analysis using a less stringent definition of HOA (pain regardless of stiffness according to the NICE 2014 definition), no statistically significant association with CAS was reached (OR, 1.25; 95%CI 0.97, 1.61). However, cIMT was significantly higher in women with HOA (adjusted difference 1.3%; 95% CI 0.05, 2.5) (Supplementary Table S1).
Another sensitivity analysis performed among the indigenous subpopulation after adjusting for confounders found no association between HOA and CAS (odds ratio [OR], 1.79; 95%CI 0.71, 4.51.) or cIMT (adjusted difference −0.67%; 95%CI −5.04, 3.69). However, after excluding those with indigenous ethnicity, cIMT was significantly larger (adjusted difference, 1.99%; 95%CI 0.39, 3.6).
Finally, we explored the relationship between the 2008 NICE diagnostic criteria for HOA and six alternative outcome definitions, finding a significant association when comparing the maximum cIMT on the right side and not reaching significance in the other cases (Supplementary Table S2.
Discussion
After careful adjustment for multiple potential confounders, we found a significant association among HOA, cIMT, and CAS in middle-aged women. We assessed HOA using the NICE 2008 clinical definition based on the paradigm that symptomatic and radiological subtypes are different entities. Distinguishing between these subtypes focuses on the expression of joint pain and stiffness as clinical surrogates of low-grade chronic inflammation, which is a basic pathophysiological component of both OA and CVD. Furthermore, we performed an additional analysis of patients who met the criteria for a less stringent updated definition of HOA (NICE 2014), in which pain, regardless of stiffness, was used, which significantly attenuated the relationship and highlighted the central role of chronic low-grade inflammation. This less stringent definition may bias the results by including patients who develop other arthropathies. Hence, the original analysis may better reflect the association between HOA and CVD.
Many other risk factors common to both OA and CVD have been described, such as ethnicity, physical activity, smoking, alcohol consumption, obesity, hypercholesterolemia, hypertension, and diabetes. 1,28 Our participants with HOA had slightly higher frequencies of diabetes, hypertension, hypercholesterolemia, smoking, and physical inactivity. Nevertheless, our association remained significant after adjusting for all these factors. There is evidence that vascular pathology starts and contributes to the progression of OA, as explained by the mechanisms by which episodical disruption of blood flow from small vessels in the subchondral bone generates subchondral ischemia that compromises nutrient and gas exchange into the articular cartilage, generating degradative changes. 31,32 There is also evidence that correlates HOA with specific inflammatory factors that may regulate chondrogenesis. For instance, Jimi et al 33 described how nuclear factor-κB signaling, a transcription factor that regulates the expression of genes that control cell proliferation and apoptosis as well as genes that respond to inflammation and immune responses, could influence chondrocyte generation in OA models. Further evidence of the relationship between HOA and cardiovascular risk factors such as dyslipidemia was addressed by Baudart et al 34 in a meta-analysis. These researchers found an association between dyslipidemia and HOA (OR 2.12, 95%CI 1.46–3.07).
Our findings could have therapeutic implications, since systemic NSAID/cyclooxygenase 2 inhibitors are currently used in the management of OA, but on the other hand have been associated with a higher risk of CVD. 35 The cardiovascular risk profile in patients with OA should be considered, and caution should be exercised with both NSAIDs and other analgesic classes. 36
Patients with OA may become physically inactive due to pain and functional limitations, 37 although less sedentarism is related to better physical function. 38 Physical limitations and sedentarism confer an increased risk for heart disease and other chronic conditions associated with metabolic syndrome, 39 notwithstanding the above, certain types of physical activities increase mechanical stress that can result in damaged joint tissue. 13,15
In patients with obesity, the risk of HOA increases twofold, 40 not only due to the mechanical effect of overload but also by systemic factors released mainly by abdominal adipose tissue that reach and activate joint cells. 41,42 We evaluated the association of CAS with HOA and no other joints intending to limit weight and general physical activity as confounding factors for CVD risk, and we adjusted for them.
We consider that our study has valuable strengths. First, our large population-based cohort provided us a representative sample. Second, we were able to perform standardized clinical evaluations and apply internationally recognized classification criteria for OA, our main exposure. Third, we have demonstrated a robust assessment of CAS, our main outcome, by accredited vascular neurologists. And lastly, experienced biostatisticians curated our statistical approach; we have corrected for confounding factors and added pertinent sensitivity analyses in order to strengthen our main findings.
There are some limitations in our study. The cross-sectional nature of our study hinders the establishment of the temporal sequence of the different variables studied and the drawing of causal inferences. However, by excluding participants with known CVD (myocardial infarction and stroke), the possibility of reverse causality decreases. We performed several detailed multivariate analyses to limit the confounding effect of our association. However, similar to any other observational analysis, residual confounding cannot be excluded. Our exposure assessment was based on self-reporting, but there is hardly any better way to inquire about pain, the main manifestation. In addition, study subjects could not be aware of their “carotid” status, whereas neurologists were blinded to study participantś “articular” responses. Finally, the generalization of our results may be limited to women, perhaps Hispanics, although we adjusted for indigenous origins.
Conclusions
We believe that HOA can be considered as a separate cardiovascular risk factor. Screening for this common illness and trying to minimize cardiometabolic risk in this population seem worthwhile, while simultaneously motivating further research in this area.
Footnotes
Acknowledgments
The authors thank Victor Sastré, Director of Regulation of the Teacherś Incentives Program (TIP), and José Luis Vela García, Julio Sabido Bastarrachea, and Humberto Rivera Perez, State TIP coordinators for Chiapas, Yucatán, and Nuevo León, for their support in contacting MTC participants and assisting with logistics operations during clinical visits. The authors thank Margarita Blanco Cornejo, Under-Director of Prevention and Health Protection at the Medical Sub-Directorate of ISSSTE, for technical and administrative support.
Data Access Statement
Owing to the sensitive nature of the data, requests to access the dataset from qualified researchers may be sent to the Mexican Teachers’ Cohort (MTC). Data Access:
Authors’ Contributions
R.R.F.-M.: conceptualization, data curation, formal analysis, methodology, software, visualization, and writing (original draft, review, and editing). T.S.R-R.: Conceptualization and writing (review and editing). C.C-B.: Investigation, project administration, resources, supervision, and writing (review and editing). M.L.: Data curation, funding acquisition, investigation, methodology, project administration, software supervision, and writing (review and editing). M.H.F-T.: data curation, formal analysis, software, and supervision. V.V-M.: Validation, visualization, and writing (review and editing). C.E.H-V.: Validation, visualization, and writing (review and editing). A.C-K.: conceptualization, formal analysis, methodology, supervision, visualization, and writing (review and editing).
Author Disclosure Statement
M.L. received limited salary support from Bloomberg Philanthropy through an institutional grant from the National Institute of Public Health, Mexico. M.L. also received a nonrestricted investigator-initiated grant from
Funding Information
This work was partly supported by an unrestricted investigator-initiated grant from
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.