
Abstract
New U.S. Centers for Disease Control and Prevention (CDC) guidelines for hepatitis C virus (HCV) testing of perinatally exposed infants and children released in 2023 recommend a nucleic acid test (NAT) for detection of HCV ribonucleic acid (i.e., NAT for HCV RNA) at 2–6 months of age to facilitate early identification and linkage to care for children with perinatally acquired HCV infection. Untreated hepatitis C can lead to cirrhosis, liver cancer, and premature death and is caused by HCV, a blood-borne virus transmitted most often among adults through injection drug use in the United States. Perinatal exposure from a birth parent with HCV infection is the most frequent mode of HCV transmission among infants and children. New HCV infections have been increasing since 2010, with the highest rates of infection among people aged 20–39 years, leading to an increasing prevalence of HCV infection during pregnancy. In 2020, the CDC recommended one-time HCV screening for all adults aged 18 years and older and for all pregnant persons during each pregnancy. Detecting HCV infection during pregnancy is key for the identification of pregnant persons, linkage to care for postpartum treatment, and identification of infants with perinatal exposure for HCV testing. It was previously recommended that children who were exposed to HCV during pregnancy receive an antibody to HCV (anti-HCV) test at 18 months of age; however, most children were lost to follow-up before testing occurred, leaving children with perinatal infection undiagnosed. The new strategy of testing perinatally exposed children at age 2–6 months was found to be cost-effective in increasing the identification of infants who might develop chronic hepatitis C. This report describes the current perinatal HCV testing recommendations and how they advance national hepatitis C elimination efforts by improving the health of pregnant and postpartum people and their children.
Introduction
Hepatitis C virus (HCV) is a single-stranded RNA virus that causes hepatitis C, an infection of the liver. Without treatment, HCV infection can result in cirrhosis, liver cancer, and death. 1 –3 Elimination of hepatitis C is a national and global priority because of the associated morbidity and mortality. 4 –6 HCV is transmitted via blood, with infections in the United States occurring most often from injection drug use (IDU), transmission from birthing parent to child during pregnancy or delivery (perinatal transmission), and less commonly through sexual contact. 7 Rates of new HCV infections in the United States have increased dramatically since 2010 in parallel with increases in IDU. 8 –10 As a result of increasing rates of infection among persons 20–39 years of age, diagnoses of HCV infections during pregnancy have been increasing steadily. 11 –13
In 2020, the U.S. Centers for Disease Control and Prevention (CDC) released new universal HCV screening recommendations, which include one-time screening for all adults and screening for pregnant persons during each pregnancy, except in settings where the prevalence of HCV infection is <0.1%. 14 Data informing the optimal timing of testing during pregnancy are lacking; however, testing at the initiation of prenatal care or at the time of pregnancy confirmation harmonizes HCV screening with other infectious disease testing during pregnancy. As of 2021, less than half of pregnant persons were receiving HCV screening during pregnancy, 15 leading to missed opportunities for linkage to curative postpartum treatment and identification of perinatally exposed children. Perinatal transmission occurs in up to 7% of exposed infants. 16,17 Historically, HCV testing recommendations instructed clinicians to test perinatally exposed children with an HCV antibody (anti-HCV) test at 18 months of age, the time by which passively transferred maternal HCV antibody has cleared and is no longer detected in a child’s blood. However, this strategy resulted in less than one-third of perinatally exposed children receiving HCV testing. 18 –21
In 2023, CDC issued new recommendations for HCV testing of perinatally exposed infants with a nucleic acid test (NAT) for detection of HCV ribonucleic acid (RNA) at 2–6 months of age to increase the number of perinatal infections identified. This is expected to lead to the identification of more infants and children with perinatal HCV infection who have a diagnosis and can be linked to care for evaluation and curative direct-acting antiviral (DAA) therapy. 22 In the era of universal screening for adults and pregnant persons, widespread availability of highly sensitive tests, and access to well-tolerated and curative DAA therapy for people 3 years and older, hepatitis C elimination is an achievable target that can improve the health and well-being of both adults and children with hepatitis C.
Epidemiology of HCV Infection
The shifting epidemiology of hepatitis C over the past decade has resulted in increasing perinatal HCV exposure among infants. 12,13,23 Since 2010, with increasing IDU, especially among young adults, the incidence of hepatitis C has risen steadily, 10 and incident cases increased by 129% during 2014–2021. During 2021, incident hepatitis C cases were highest among persons aged 20–39 years, and 57% of all cases with risk information available reported IDU. 7 Acute HCV infection was highest among people who identified as non-Hispanic American Indian/Alaskan Native (AI/AN) and those living in eastern and southeastern states. Newly reported chronic HCV infections were highest among persons aged 20–39 years, followed by persons aged 50–70 years, and HCV-associated mortality was 3.4 times higher among non-Hispanic AI/AN and 1.7 times higher among non-Hispanic Black persons than among non-Hispanic White persons.
Although these numbers demonstrate a striking HCV burden, they are likely an underrepresentation given that the implementation of universal screening of all adults and pregnant persons needs improvement. 14 One recent analysis found less than half of people are screened for HCV infection during pregnancy, leading to missed opportunities to diagnose the birthing parent and perinatally exposed child, and link those with hepatitis C to life-saving treatment. 15
Universal Screening
In the United States, HCV testing of all blood, plasma, organ, tissue, and semen donors since 1991 has decreased the risk of acquiring HCV infection through medical procedures and interventions. 24 Until 2012, HCV testing among the general population was risk-based. In 2012, to address the prevalence of hepatitis C, which was five times higher among adults born before 1945 and after 1965, recommendations for HCV screening were expanded to include the cohort of individuals born between 1945 and 1965 (i.e., baby boomers). 25 In 2020, due to the increasing prevalence of HCV infection in the general population, the CDC began recommending universal one-time screening for all adults aged 18 years and older and screening all pregnant persons during each pregnancy, except in areas where the prevalence of HCV infection is <0.1%. 14 Because risk factor information for hepatitis C is not always disclosed, universal screening mitigates bias and removes stigma associated with testing, allowing identification of those who can transmit the infection to others, including via perinatal transmission. In addition to the CDC, the United States Preventive Services Taskforce, 26 the American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA), 27 the American College of Obstetricians and Gynecologists (ACOG), 28 and the Society for Maternal Fetal Medicine 29 also recommend universal screening for hepatitis C during pregnancy. However, more work is needed to facilitate the implementation of these recommendations.
Postpartum HCV Infection Treatment
Currently, there is insufficient evidence to recommend treatment with DAAs during pregnancy; a person with hepatitis C should ideally be identified and treated before pregnancy to prevent perinatal HCV exposure. 27 However, this does not always occur. The Surveillance for Emerging Threats to Pregnant People and Infant Network 30 has shown that during 2018–2021, only 21% of pregnant people with HCV infection were diagnosed before pregnancy, indicating missed opportunities for linkage to care and curative treatment before pregnancy. 31 If identification and treatment before pregnancy are not possible, pregnancy is an opportunity to diagnose HCV infection and facilitate a linkage to care during pregnancy for initiation of treatment during the postpartum period after breastfeeding is completed. The AASLD-IDSA advises that people who become pregnant while on DAA therapy to discuss the risks and benefits of continuing therapy with their clinician. 27 Furthermore, per the AASLD-IDSA guidelines, treatment can be considered during pregnancy on a case-by-case basis. Early data on the safety of therapy throughout pregnancy has shown that DAAs are effective and safe in curing HCV infection and decrease the risk of perinatal transmission. 32 Further trials of DAA during pregnancy are ongoing (https://clinicaltrials.gov/study/NCT05140941) in addition to a global registry to collect data on DAA use during pregnancy. 33
Perinatal HCV Transmission
Perinatal HCV transmission is limited to infants and children born to people with current HCV infection. 34 Transmission occurs in utero or during delivery and has been estimated to occur in 6–7% of pregnancies with detectable HCV RNA. 16,17 Coinfection with poorly controlled human immunodeficiency virus (HIV) is associated with an elevated perinatal HCV transmission rate (12%). 17 The risk of vertical transmission of HCV associated with amniocentesis or chorionic villus samples is generally low, 35 and ACOG recommends shared decision making when counseling patients about the risk of vertical transmission. 28 Mode of delivery (i.e., cesarean section over vaginal delivery) and breastfeeding have not been associated with perinatal transmission. 27,29 As in adults, perinatal HCV infection is often asymptomatic. 36,37 Although spontaneous clearance can occur in up to 67% of children with perinatal HCV infection by age 5 years, 38 chronic perinatal HCV infections can progress to cirrhosis, hepatocellular carcinoma, and death. 39 –42
Previous HCV Testing Recommendations for Perinatal Exposure
In general, HCV testing for perinatally exposed infants and children can be completed as early as age 2 months with a NAT for HCV RNA or as early as age 18 months with an anti-HCV test. 43 Before the 2023 CDC recommendations for early HCV testing among perinatally exposed infants, testing with an anti-HCV test at age 18 months was recommended by professional organizations. 43 –45 Although these organizations allowed for earlier HCV RNA testing in situations where there was a concern for loss to follow-up, usually testing was postponed until after age 18 months. With this strategy, most perinatally exposed infants and children were not tested and, therefore, not diagnosed.
Evidence for New HCV Testing Recommendations for Perinatal HCV Exposure
Given increasing perinatal infections, challenges with significant pediatric loss to follow-up, and higher rates of attending well-child visits among infants age ≤6 months compared to children aged 18 months and older, 19,46,47 CDC evaluated the evidence supporting testing all perinatally exposed infants and children with a NAT for HCV RNA at age 2–6 months compared to the traditional approach of anti-HCV testing at or after age 18 months. 22 Current HCV RNA tests have high sensitivity and specificity and can be used for diagnosis of perinatal HCV transmission in infants at age 2–6 months. 48 Cost-effectiveness analyses demonstrated that compared to anti-HCV with reflex to HCV RNA testing at or after age 18 months, testing perinatally exposed infants at age 2–6 months with a single NAT for HCV RNA was cost-saving, resulted in better health outcomes, and would prevent long-term morbidity and mortality associated with hepatitis C. 49
New Perinatal HCV Testing Recommendations
In November 2023, the CDC released new recommendations for all perinatally exposed infants (i.e., born to persons with detectable HCV RNA during pregnancy) to be tested with a NAT for HCV RNA at 2–6 months of age (Fig. 1). 22 Infants with a detectable HCV RNA should then be managed in consultation with a clinician with expertise in the management of pediatric HCV infection. No further follow-up is required for infants with undetectable HCV RNA unless clinically warranted (i.e., clinical symptoms, signs, or laboratory findings consistent with hepatitis C). Infants born to persons with probable HCV infection during pregnancy (i.e., anti-HCV positive, HCV RNA status unknown) should also be tested with a NAT for HCV RNA at 2–6 months of age as should infants born to persons with unknown HCV RNA status during pregnancy (e.g., separation from birthing parent). Infants who were not tested at 2–6 months of age with a NAT for HCV RNA should be tested for HCV RNA if aged 7–17 months or with an anti-HCV with reflex to HCV RNA if aged 18 months and older (Fig. 2). Other considerations include testing of siblings with the same birthing parent as infants with identified perinatal HCV exposure unless the birthing parent’s HCV testing was known to be negative in the prior pregnancies. Finally, infants born to a birthing parent with a risk of acute HCV infection during pregnancy (e.g., IDU) who were not tested close to the time of delivery would also benefit from testing.

Algorithm for hepatitis C virus (HCV) infection testing in perinatally exposed infants*.
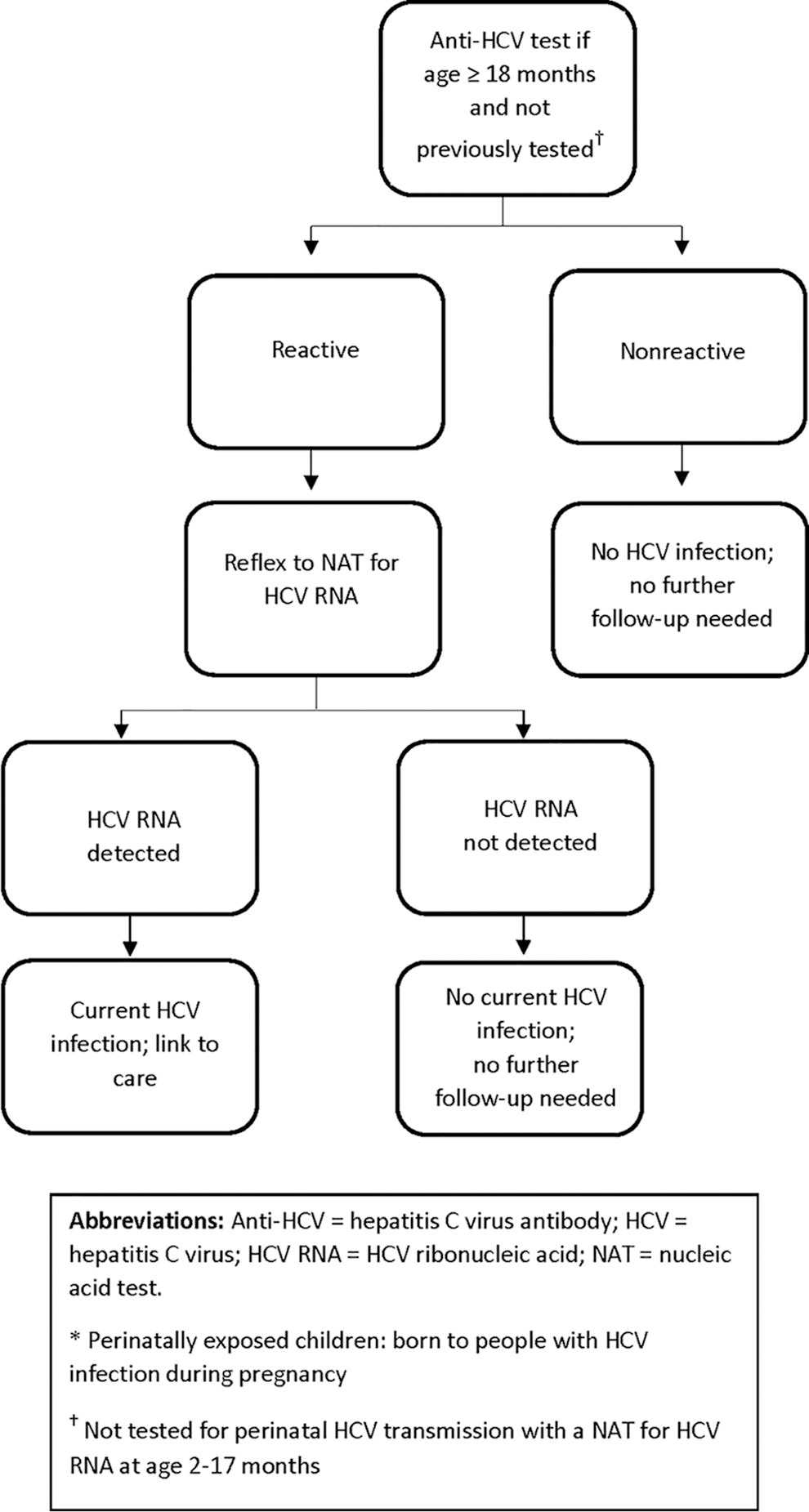
Alternative algorithm for hepatitis C virus (HCV) infection testing in perinatally exposed children* age ≥18 months who have not previously been tested†.
Hepatitis C Elimination and Perinatal Health
The World Health Organization’s targets for hepatitis C elimination are to reduce the incidence of new chronic infections by 90% and mortality from chronic infections by 65% during 2015–2030 (https://iris.who.int/bitstream/handle/10665/206453/WHO_HIV_2016.04_eng.pdf?sequence=1). National goals also include an emphasis on reducing new viral hepatitis infections, including perinatal viral hepatitis infections, decreasing HCV-related morbidity and mortality, and increasing the proportion of people with hepatitis C who are aware of their infection. 4 Furthermore, the federal government has proposed a national hepatitis C elimination strategy, with a 5-year program focused on accelerating the availability of HCV point-of-care tests, providing increased access to curative hepatitis C treatment including during the postpartum period, and addressing barriers to hepatitis C care. 5 A recent update to CDC guidance for HCV testing specified the importance of complete testing with a single specimen collection (i.e., blood draw) for both steps of the test algorithm (anti-HCV with automatic, or reflex, HCV RNA testing on all anti-HCV positive samples). 50 However, as point-of-care HCV RNA tests become available in the United States, viral first screening strategies (i.e., HCV RNA without preceding antibody testing) might be cost-effective in settings with a high burden of hepatitis C and could markedly improve diagnosis and linkage to care by integrating testing and confirmation of results during a single health care encounter.
Given that people of reproductive age are experiencing the largest increase of newly identified acute and chronic HCV infections, including people who are pregnant and their children in hepatitis C elimination initiatives is critical. Recently published recommendations for universal HCV screening during pregnancy and among perinatally exposed children are aimed at improving the uptake of routine HCV screening and testing among populations disproportionately impacted and those who have difficulty accessing care; broad coverage is required to accomplish global and national elimination goals.
There are also critical strategies that must be implemented to improve postpartum treatment of HCV infection and reduce subsequent perinatal HCV exposures. Clinicians might be inclined to refer pregnant people with HCV infection to a specialist only after the pregnancy is completed. However, by this time, the postpartum person might be focused on the care of their infant or have lost insurance coverage; data has shown postpartum visit attendance and treatment rates are incredibly low. 51,52 Antenatal referral while insurance coverage is active and the pregnant person is engaged in routine care can ensure that they have the opportunity for education, time to consider hepatitis C treatment, and are informed about the importance of hepatitis C treatment for themselves and HCV testing for their exposed infant. Telemedicine for these education-based visits during pregnancy might help patients engage in more flexible care that also eliminates potential transportation barriers. 53 Further research is also needed about DAA treatment safety and efficacy during pregnancy, hepatitis C cure during the antenatal period with associated reduction of perinatal transmission to the infant, and resulting decreased overall community transmission.
Policy and Program Opportunities
Policy and program opportunities for increasing HCV testing include automatic electronic medical record prompts; state laws requiring HCV screening during pregnancy and infant HCV testing as indicated; and obstetric panels to ease ordering and ensure automatic HCV RNA testing of all anti-HCV reactive samples. With increasing screening and diagnosis of HCV infection in pregnancy, more exposed infants are being identified. However, in many instances, handoff between delivering clinicians and those caring for neonates is incomplete, especially when pregnant people and their infants move between clinicians or facilities. During transitions, critical information including pregnancy hepatitis C status and associated lab results might not be in the neonatal record. This is especially of concern in pregnancies complicated by a change in the neonatal caregiver with the incomplete transfer of pregnancy records. Institutional systems must be implemented to create systems for facilitating the hand-off of necessary hepatitis C information to allow for appropriate testing of infants and children exposed to HCV in utero. Furthermore, universal national Medicaid expansion through 12 months after birth is critical to facilitating postpartum DAA treatment with an emphasis on health equity, especially for people with low income, substance use disorder, or other life complexities. Programmatic opportunities include funding for programs to ensure testing and treatment of children, similar to HIV and hepatitis B virus models (e.g., National Perinatal Hepatitis B Prevention Program), which are very successful in following exposed infants to appropriate care. Finally, ensuring appropriate HCV testing and treatment has occurred should be integrated outside of prenatal, postpartum, and pediatric care settings, including among non-health care related partners that provide services to pregnant people, such as within mental health services, substance use treatment programs, emergency rooms, syringe service programs, homeless shelters, federally qualified health centers, health departments, carceral settings, and organizations engaged in maternal and child health (e.g., Supplemental Nutrition and Assistance Program, Special Supplemental Nutrition Program for Women, Infants, and Children).
Innovative Approaches and Solutions
The implementation of HCV rapid, viral first (i.e., HCV RNA single-step testing) diagnostics and future Food and Drug Administration (FDA) approval of DAA therapy for use during pregnancy are achievable goals that will support HCV elimination. With these additional tools and data, the United States can advance to test and treatment initiation for pregnant people in a single visit while they are engaged in routine prenatal care. A randomized controlled trial showed that rapid treatment initiation for hepatitis C among people who inject drugs was associated with significantly higher rates of cure than usual care, which included facilitated referrals and navigators. 54 In other words, reducing the number of visits required for diagnosis and treatment appears highly impactful. This is also important in the pediatric setting. Allowing pediatricians to perform HCV RNA fingerstick or heel stick testing at point-of-care would preclude the need for phlebotomy, which is more challenging among pediatric populations and might require additional visits to a laboratory. If such testing were available, this real-time viral testing could identify children with perinatal HCV infection at age 2–6 months while they are more likely to be engaged in regular care. 19,46 This would allow for earlier engagement with clinicians with expertise in pediatric HCV management and might improve the likelihood of curative therapy at age 3 years before complications of liver disease develop. Improving the ease of testing and treating pregnant people and children is an essential component of hepatitis C elimination.
Conclusions
CDC recommendations for HCV testing during each pregnancy and of all perinatally exposed infants at age 2–6 months are essential for the elimination of hepatitis C 22 ; however, many additional opportunities remain to leverage evidence-based interventions. Clinicians, patients, and public health professionals must work together to implement this guidance and continue the charge toward national HCV elimination.
Footnotes
Acknowledgments
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Authors’ Contributions
L.P.: Conceptualization, Methodology, Writing—Original draft preparation, Writing—Review and Editing, Project administration; K.M.: Methodology, Writing—Review and Editing; E.J.C.: Methodology, Writing—Review and Editing; S.K.: Writing—Review and Editing; N.F.-Writing—Review and Editing; K.W.: Writing—Review and Editing; V.T.T.: Writing—Review and Editing; S.Y.K.: Writing—Review and Editing; C.W.: Conceptualization, Writing—Review and Editing, Supervision; A.S.: Conceptualization, Writing—Review and Editing, Supervision.
Disclaimer
In this report, the term “maternal” is used at times for clarity to identify the person who is pregnant or postpartum. The authors recognize that pregnancy is not equated with the decision to parent, nor do all parents who give birth identify as mothers.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.