
Abstract
Introduction:
Females suffer greater lifetime risk of stroke and greater morbidity and mortality from stroke compared with males. This study’s objective was to identify differences in metabolomic profiling of females and males with stroke and which differences were associated with neurological outcome.
Methods:
Females and males with acute ischemic stroke enrolled in the Emergency Medicine Specimen Bank at a comprehensive stroke center provided whole blood samples upon arrival for mass spectrometry-based metabolomics. We used descriptive statistics to characterize the cohort. A linear regression model was fit for individual metabolites to determine differences in relative abundance between males and females while controlling for covariates (age, race/ethnicity, postmenopausal status, cardiovascular risk factors, depression, time between sample collection and last known well, and initial National Institutes of Health Stroke Scale [NIHSS] score). For each differentially expressed metabolite, a linear regression model was fit to determine the association between the metabolite and NIHSS at 24 hours after admission while controlling for the covariates and acute treatments.
Results:
After adjusting for covariates, eight metabolites differed in females and males with a stroke. These included amino acids or their metabolites (proline and tryptophan), nucleotides (guanosine diphosphate [GDP], and inosine-3′,5′-cyclic monophosphate), citrate, dehydroascorbate, choline, and acylcarnitine-(5-OH). GDP and dehydroascorbate were significantly associated with 24-hour NIHSS (p = 0.0991).
Conclusions:
Few metabolites were differentially abundant in blood after a stroke when comparing females with males and controlling for confounders, but the interactions between biological sex and GDP, as well as biological sex and dehydroascorbate, were associated with 24-hour neurological function. This has important implications for future studies that evaluate the therapeutic potential of these metabolites in ischemic stroke.
Introduction
Ischemic stroke is one of the top 15 global causes of disability and among the top 10 global causes of years of life lost due to premature death. 1 In the United States, females have a greater lifetime risk of stroke, with 55,000 more females per year diagnosed with stroke compared with males in the United States. 1 Despite advances in stroke care, women who experience an acute ischemic stroke (AIS) also suffer greater morbidity and mortality from their stroke than men. 2,3 Age at the time of stroke and differences in societal factors contributing to delays in care or treatment, such as higher rates of atrial fibrillation and lower rates of anticoagulation, may contribute to these disparate outcomes. 3 However, there remain fundamental biological differences in the response to ischemia by sex, which may also contribute to disparities in patient outcomes. Prior studies have found notable differences in the cell death pathways activated in response to stroke, the immune response, and the epigenetic and genetic influences of the sex chromosomes. 4 However, understanding of sex differences in the metabolic response to stroke is lacking.
In AIS, omics analysis has identified dysregulated metabolic pathways that can be used to identify markers of increased risk, AIS subtypes, and poor outcomes. 5 These processes include derangements in metabolites involved in oxidative stress, neuronal cell death, and ischemic–reperfusion injury. 5 Compared with healthy controls, metabolic profiling of ischemic stroke patients has shown several differences in amino acid metabolism, including increased levels of lactate, carbonate, and glutamate but decreased levels of several other amino acids with roles in inflammation, energy, and oxidative stress. 6 Within this analysis, levels of tyrosine, lactate, and tryptophan were found to be highly predictive of the diagnosis of AIS compared with controls. In preclinical male rodent models and in patients with a cardioembolic stroke, branched chain amino acids (leucine, isoleucine, and valine) were found at decreasing levels after ischemia compared with controls. 7 Furthermore, lower branched chain amino acid levels were associated with female sex and worse outcome at 3 months. In addition, subgroup analysis of targeted metabolomics focusing on tryptophan metabolism through the kynurenine pathway has revealed increased levels of quinolinic acid in females with acute ischemic stroke compared with males. 8 However, after adjusting for age, there was no difference in quinolinic acid levels, or other metabolites within the pathway. However, that study did not address other key confounders. Together, these studies suggest that metabolomics may provide further insight into a sexually dimorphic response to stroke. The objective of this study was to leverage metabolomics to identify sex differences in the acute response to ischemic stroke and to identify those changes associated with neurological outcomes.
Methods
Study population and clinical data extraction
This is a retrospective cohort analysis of 54 females and 56 males with final diagnosis of AIS, who presented to the University of Colorado Health Hospital, a comprehensive stroke center, in Aurora, CO, between March 20, 2018, and March 20, 2023. Diagnosis of AIS was determined by a stroke neurologist based on a patient’s clinical presentation and confirmed by magnetic resonance imaging when available. Eligible subjects were adults (18 years of age or older) and English- or Spanish-speaking, who agreed to participate in the Emergency Medicine Specimen Bank, providing a whole blood sample for analysis. A trained research assistant extracted the following variables from the electronic health record to characterize the patient cohort: patient demographics (age, biological sex, race, and ethnicity), comorbid health conditions (hypertension, dyslipidemia, atrial fibrillation, diabetes mellitus, depression, prior stroke or transient ischemic attack, coronary artery disease, congestive heart failure, chronic kidney disease, and end-stage renal disease), current medications, acute stroke interventions (intravenous thrombolysis or mechanical thrombectomy), initial National Institutes of Health Stroke Scale (NIHSS) score upon emergency department arrival, and NIHSS score at 24 hours from arrival. Data were extracted using standardized procedures and REDCap data collection forms. This work was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki) and was approved by the Colorado Multiple Institutional Review Board (COMIRB #17–1642 and COMIRB #21–2515).
Sample collection and untargeted metabolomics analysis
Upon arrival to the emergency department, under a delayed consent process, whole blood was collected into ethylenediaminetetraacetic acid-coated vacutainers by nursing staff and immediately frozen at −20°C. Samples were thawed on ice once and aliquoted for permanent storage at −80°C. For extraction of metabolites, a single aliquot was thawed on ice, and 10 µL was transferred to a 96-well plate with a 96-well pipettor (Integra) and then diluted with 190 µL of cold 5:3:2 (v/v/v) methanol:acetonitrile:water. Plates were agitated at 800 rpm for 30 minutes at 4°C, and then extracts were passed through a filter plate (Biotage ISOLUTE Filter+, cat no 120-2000-P25) into a collection plate (Biotage cat no 121-5202) using a positive pressure manifold. Filtrate aliquots (120 µL) were transferred to new plates, dried, and reconstituted in 0.1% formic acid. Samples were randomized and analyzed on a Thermo Vanquish ultra-high pressure liquid chromatograph coupled to a Thermo Orbitrap Exploris 120 mass spectrometer with 10 µL injection in positive and negative ion modes (separate runs) using a 5-minute C18 gradient. 9 RawConverter converted data files from .raw to .mzXML. Maven (Princeton University) was used to annotate and integrate peaks. The peak area (relative concentration) for each identified metabolite was reported (Supplementary Table S3).
Statistical analysis
We used descriptive statistics to characterize the sample population with regard to patient demographics, comorbidities, current medication list at the time of admission, and neurological function at presentation and 24 hours (NIHSS score). We report the proportions for categorical variables and the means with standard deviation and median with interquartile range for continuous variables. We used principal component analysis (PCA) and partial least squares discriminant analysis (PLS-DA), 10 available in a web-based analytical pipeline, MetaboAnalyst 5.0, as a multivariate approach to explore the variation in the dataset. For initial PCA and PLS-DA, data were normalized by the median and auto scaling was used. We then used a linear regression model for each metabolite to determine whether its relative abundance (peak intensity) varied by biological sex while adjusting for key confounders. The potential confounders included age, race and ethnicity, time to last known well, initial NIHSS, presence of a cardiovascular risk factor (hypertension, dyslipidemia, diabetes mellitus, prior stroke, coronary artery disease, or chronic kidney disease), depression (known to influence tryptophan metabolism), and postmenopausal status. 11 From these identified metabolites, individual linear regression models were fit to determine the association between relative metabolite concentration and 24-hour NIHSS score while controlling for receipt of an acute intervention (intravenous thrombolysis or mechanical thrombectomy), an interaction effect between the individual metabolite and sex, and those confounders in the original model. Although long-term follow-up was unavailable for many subjects, 24-hour NIHSS was consistently documented and has been shown to predict neurological function at 90 days. 12
Results
Patient characteristics
There were 54 females and 56 males with a mean age of 66 years and 65 years, respectively (Table 1). Of females, 63% were non-Hispanic Whites, and of males, 52% were non-Hispanic Whites. There was a slightly higher proportion of males with hypertension or dyslipidemia compared with females but a slightly higher proportion of females with atrial fibrillation and depression. The mean time to collection of the blood sample from last known well was 10 hours (standard deviation 12 hours) in females and 19 hours (standard deviation of 27 hours) in males. The initial NIHSS and the NIHSS at 24 hours were both higher in females (initial mean 5.2, standard deviation 6.0; 24-hour mean 3.9, standard deviation 6.6) compared with males (initial mean 3.7, standard deviation 3.4; 24-hour mean 3.1, standard deviation 3.5).
Patient Characteristics
Missing data for one male subject.
IQR, interquartile range; LKW, last known well; NIHSS, National Institutes of Health Stroke Scale; SD, standard deviation; TIA, transient ischemic attack.
Metabolites differing by sex (unadjusted analysis)
To obtain a broad understanding of potential metabolomic differences in males and females with AIS, we performed an unadjusted analysis. Using PCA for all metabolites in the dataset, data were grouped into metabolite clusters that summarized the overall patterns of variation within the overall population. This revealed two separate clusters of metabolites that explained 11% and 9.8% of the variance, respectively, and clusters were not differentiated by biological sex (Fig. 1A). Using PLS-DA to compare metabolic differences in males and females, component 1 of the PLS-DA explained only 6.2% of the variance in metabolome expression (Fig. 1B). Component 2 explained 7.5% of this difference. The top 15 metabolites contributing to the greatest variance in component 1 PLS-DA (Fig. 1C) included multiple acylcarnitines, multiple amino acids, and dehydroascorbate. These metabolites (excluding acylcarnitines) are involved primarily in alanine, aspartate, and glutamate metabolism, cysteine and methionine metabolism, and the tricarboxylic acid (TCA) cycle according to Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analysis (Fig. 1D).
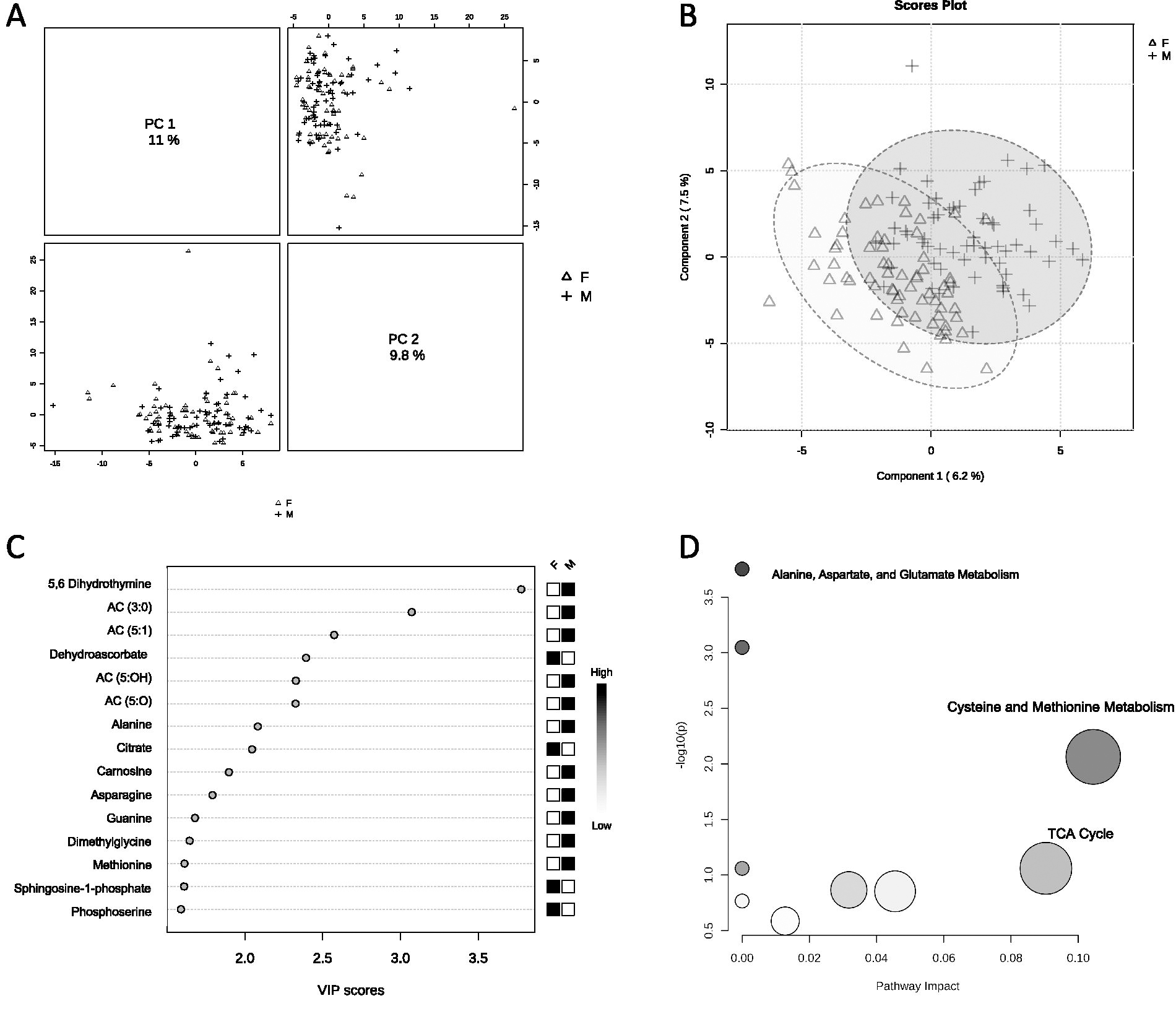
Principal component analysis, partial least squares discriminant analysis, and KEGG pathway analysis of whole blood samples from patients with acute ischemic stroke without adjusting for potential confounders.
Differentially abundant metabolites and neurological outcome
A linear regression model was fit to assess sex differences in relative metabolite levels while controlling for confounders (age, race and ethnicity, postmenopausal status, presence of cardiovascular risk factors, history of depression, time of sample collection to last known well, and initial NIHSS). Blood samples were obtained before an acute intervention. As such, acute interventions were not included as a confounder in the initial analysis of sex differences in relative metabolite levels. Females and males had significantly different levels of eight metabolites (Table 2, Supplementary Table S1). These metabolites were either amino acids or nucleotides, or were involved in the TCA cycle, glycerophospholipid biosynthesis, redox homeostasis, or carnitine and fatty acid metabolism. A linear regression model for neurological outcome (NIHSS score at 24 hours) was then fit for each of the eight identified metabolites controlling for the above confounders, receipt of an acute intervention (intravenous thrombolysis or mechanical thrombectomy), and an interaction factor between sex and the individual metabolite. In the adjusted model, only the interaction between biological sex and guanosine diphosphate (GDP) and dehydroascorbate was significantly associated with NIHSS at 24 hours. In females, both GDP and dehydroascorbate levels increased with higher 24-hour NIHSS, representing increasing levels with worsening neurological function. In males, the levels of GDP and dehydroascorbate decreased with increasing 24-hour NIHSS, representing decreasing levels with worsening neurological function (Fig. 2, Supplementary Table S2).
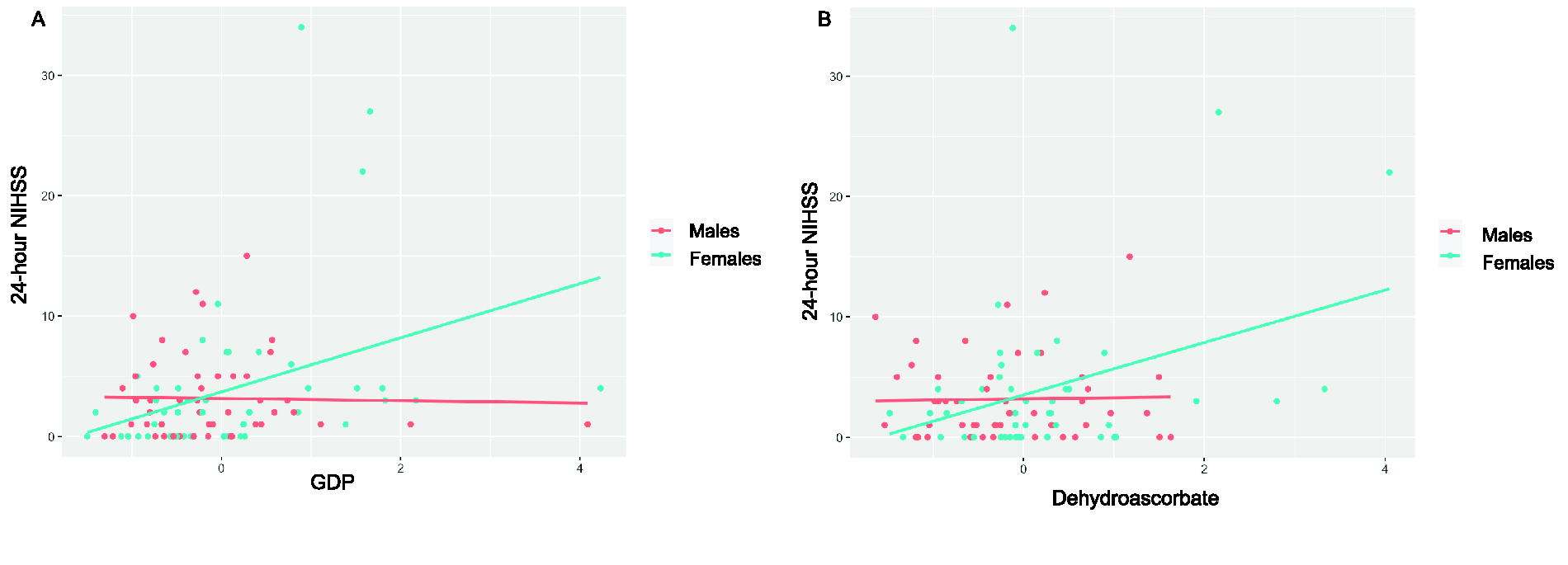
Comparison of metabolite abundance and 24-hour NIHSS in males and females.
Metabolites Significantly Differing by Biological Sex
The peak intensity of individual metabolites reflects the relative concentrations.
TCA, tricarboxylic acid.
Discussion
This study represents a dedicated untargeted metabolomics analysis of sex differences in the blood following acute ischemic stroke. There were eight metabolites differentially abundant in females compared with males after controlling confounders such as age, race, and ethnicity, presence of cardiovascular risk factors, presence of depression, postmenopausal status, time of sample collection to last known well, and initial NIHSS. However, of these metabolites, GDP and dehydroascorbate had a positive association with increasing (worsening) 24-hour NIHSS in females and a negative association with increasing (worsening) 24-hour NIHSS in males after controlling for confounders. This study focuses on the hyperacute response to stroke, which may be amenable to future therapeutic intervention. However, it has previously been shown that the 24-hour NIHSS correlates with 90-day modified Rankin scale. 12 This may suggest that not only are the observed metabolic differences important for the acute stroke response, but they may also have long-term neurological consequences.
The timing of changes in metabolite abundance over the hyperacute phase of stroke, within hours of stroke onset, could suggest that these metabolites are acting as acute-phase reactants. Acute-phase proteins are involved in the acute inflammatory response with additional roles in gluconeogenesis, lipogenesis, and lipolysis; the complement response; and the coagulation system. 13 Although none of the identified metabolites are traditionally defined as acute-phase proteins, some metabolites [citrate, dehydroascorbate, choline, tryptophan and AC-(5-OH), and GDP] may have roles in the acute-phase response.
GDP is a purine nucleotide derived from guanosine. Extracellular GDP is hydrolyzed into GMP and then subsequently guanosine. 14 Although the precise role of GDP in stroke has not been studied, guanosine has been shown to activate neuroprotective responses in rodent models of ischemia. 15 This includes stimulation of astrocytes to promote cell survival, proliferation, and differentiation through G protein-coupled receptor signaling. In vivo rodent models have also found that systemic administration of guanosine can lead to decreased infarct volumes and neurological deficits. 15 –17 However, these studies have not been recapitulated in humans and are primarily based in male rodent models. Based on these preclinical and in vitro data, it is not surprising that decreasing levels of GDP in males are associated with worsening neurological function (higher NIHSS) at 24 hours. The fact that increasing levels of GDP in females are associated with worsening neurological function at 24 hours might suggest additional downstream factors may be interfering with the neuroprotective effects of GDP in females. These differences are lost when using only models of one sex.
Dehydroascorbate is also known as dehydroascorbic acid (DHA) and is an oxidized metabolite of ascorbic acid (vitamin C). 18 In male rodent models of ischemic stroke, intraperitoneal DHA after middle cerebral artery occlusion decreased cerebral edema, helped maintain the blood–brain barrier, reduced the inflammatory response to ischemia, and reduced cell death. 19 In other preclinical models, intravenous DHA also led to improved cerebral blood flow poststroke, a sixfold reduction in infarct volume, and improved neurological function. 20 Unfortunately, these studies did not assess for sex differences in the response to DHA. These preclinical data are in line with the results of the untargeted metabolomic analyses that revealed decreasing abundance of DHA in males was associated with worsening neurological function at 24 hours. However, like with GDP, the finding that increasing levels in females were associated with worsening neurological function again suggests unidentified processes may modulate these otherwise neuroprotective metabolic processes.
Of the other metabolites that were differentially expressed in males and females with ischemic stroke, most represented amino acids or were part of amino acid metabolism. Specifically, KEGG pathway analysis of the differentially expressed metabolites (excluding acylcarnitines) revealed the highest contributions to alanine, aspartate, and glutamate metabolism, cysteine and methionine metabolism, and the TCA cycle (Fig. 1D). This is consistent with previous studies that have demonstrated increased levels of lysine, phenylalanine, methionine, tryptophan, leucine, lactate, ethanolamine, alanine, isoleucine, valine, tyrosine, 3-hyroxybutyric acid, glycerol gamma-aminobutyric acid, and glycine in ischemic stroke compared to controls. 21 There were concomitant decreased levels of aspartate, taurine, serine, N-acetyl-aspartic acid, and glutathione in ischemic stroke compared with controls. 21 Through pathway enrichment analysis, these metabolites mapped to seven key pathways, which also included alanine, aspartate, and glutamate metabolism.
Prior targeted metabolomic analyses and subgroup analyses revealed possible sex differences in quinolinic acid, a downstream metabolite of tryptophan metabolism using the kynurenine pathway, and branched chain amino acids. 7,8 However, after controlling for only age, there was no difference in any kynurenine pathway metabolite. Furthermore, it is unclear if association between branched chain amino acids and female sex would persist had authors controlled for initial stroke severity and age. This untargeted metabolomic analysis revealed that after adjusting for key confounders beyond just age (i.e., history of depression, NIHSS score, cardiovascular risk factors), males and females with stroke had different relative abundances of tryptophan. Although tryptophan was not associated with sex differences in NIHSS at 24 hours, tryptophan metabolism has also been shown to play important roles in poststroke cognitive decline and early stroke mortality and has been implicated in the immune response in other conditions. 22 –25 The role of tryptophan in sex differences in these additional downstream consequences of stroke deserves future investigation.
The heterogeneity of subjects within this study sample represents both strengths and limitations. Females had slightly more severe stroke on presentation and tended to have samples collected closer to their last known well time compared with males. Despite the initially high NIHSS for females, the 24-hour NIHSS was similar for both males and females. This is somewhat inconsistent with epidemiological data that suggest females have worse neurological outcomes compared with males. 2,3 Given these baseline differences, a strength of this study compared with other targeted metabolomic analyses was the ability to control for time to last known well, treatment with intravenous thrombolysis or endovascular therapy, and subtle differences in initial stroke severity. This affords an improved assessment of metabolic processes driving disparate neurological outcomes in males and females. By focusing in on metabolic changes in the hyperacute stages of an ischemic stroke, this study can help identify key processes that are differentially regulated in males and females. Although this stage may not reflect the cumulative metabolic effects over times, the identified metabolites may be amenable to therapeutic manipulation for improved neurological outcomes.
Conclusions
This untargeted metabolomic analysis reveals overall similarities in the blood metabolome of males and females with acute ischemic stroke, except for several metabolites primarily involved in amino acid metabolism and carnitine and fatty acid metabolism. The interaction between biological sex and GDP and the interaction between biological sex and dehydroascorbate were the only differentially expressed metabolites associated with neurological function at 24 hours. This has important implications for future studies that evaluate the therapeutic potential of these metabolites in ischemic stroke.
Footnotes
Acknowledgments
The authors would like to acknowledge the help of the University of Colorado School of Medicine Metabolomics Core for generation of metabolomics data and Alexis Vest and members of the Emergency Medicine Specimen Bank for their assistance with sample collection and processing.
Authors’ Contributions
All authors read and approved the final article. Conceptualization: L.D., S.N.P., P.S.H., J.A.R., and A.A.M.; methodology and data collection: L.D., H.M.H., J.A.R., and A.A.M.; formal analysis: L.D., J.A.R., and T.V.; writing—original draft preparation: L.D.; writing—reviewing and editing: L.D., H.M.H., S.N.P., J.A.R., T.V., P.S.H., and A.A.M.; and funding acquisition: L.D., S.N.P., J.A.R., and A.A.M.
Disclaimer
Its contents are the authors’ sole responsibility and do not necessarily represent official NIH views.
Author Disclosure Statement
The authors report no conflicts of interests
Funding Information
The research leading to these results received funding from the following sources: Clinical and Translational Sciences Institute Pilot Grant Award (
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.