
Abstract
Introduction:
Differences in time commitments and resources contribute to the difficulties of work–life integration for many physician-scientists, particularly for women with family caregiving responsibilities. Understanding the challenges faced by this population is critical for the retention of these critical members of the workforce.
Methods:
We conducted semi-structured telephone interviews with recipients of the 2017 Doris Duke Charitable Foundation’s Fund to Retain Clinical Scientists (FRCS) and reviewed application narratives from the 2020 award recipients. Award recipients were asked about their caregiving responsibilities and careers, particularly as they related to the impact of the FRCS award and the aftereffects of the COVID-19 pandemic. Analysts then iteratively revised the coding scheme and interpreted the data using qualitative thematic analysis.
Results:
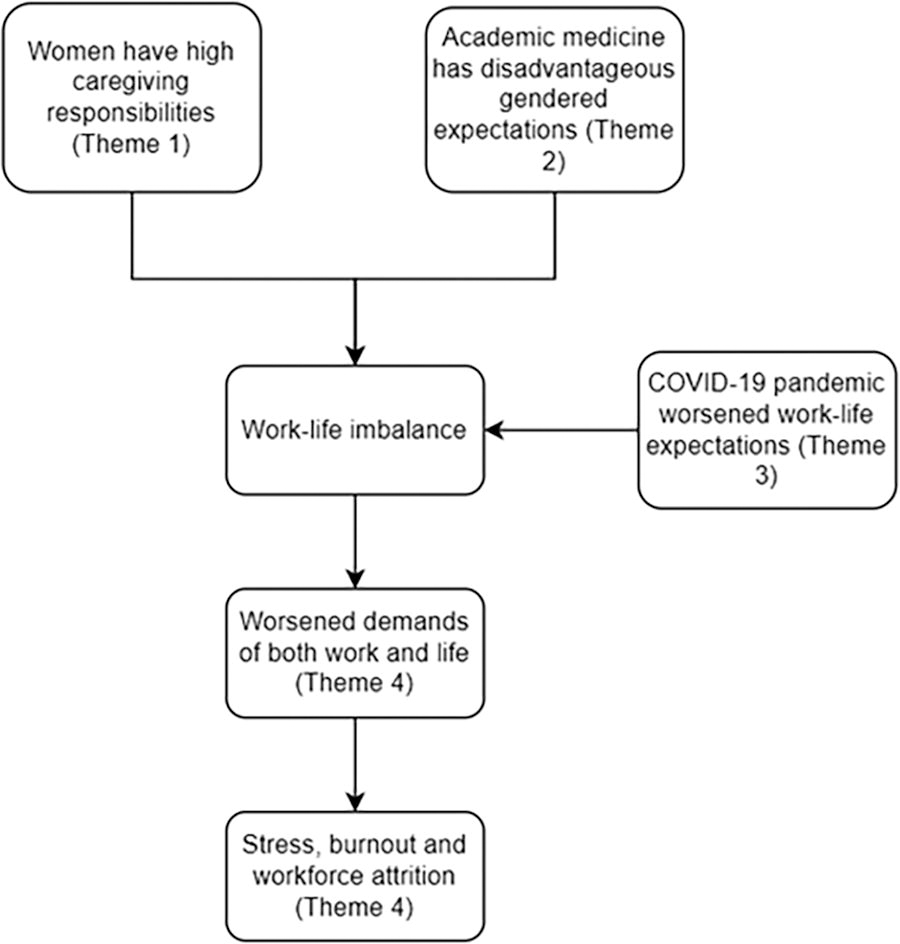
Of the 14 interviewees and 19 narrative contributors, 25 (76%) were women. The main qualitative themes that emerged were as follows: (1) women experience unrealistically high caregiving burdens, (2) women are overburdened by disadvantageous and undervalued expectations at work, (3) work–life expectations increased during the COVID-19 pandemic, and (4) unrealistic work–life expectations led to guilt and burnout.
Conclusions:
These findings provide a rich understanding of the factors contributing to guilt and burnout among physician-scientists, particularly women, and how work duties that increase physician obligations exacerbated these challenges. Understanding these experiences is critical to supporting and retaining a diverse workforce in academic medicine.
Background
Physician-scientists are uniquely positioned to investigate patient-centered questions, and diversity in this pool is critical to designing innovative and relevant insights. While the number of women in medical school has increased, high attrition rates result in a disproportionately low representation among tenured faculty, independent physician-scientists, and leaders in academic medicine. 1 –3 Woman physician-scientists face unique challenges; for example, they spend a disproportionate amount of time on domestic work compared with their male counterparts. 4,5 This limits time available to women to pursue professional goals. 6 Women of color are particularly likely to face extraprofessional caregiving demands 7 and also must navigate heightened challenges due to the unique intersection of biases they face.
Several academic institutions have developed policies to address these issues, including expanding childcare options or extending tenure timelines.
8
In 2015, the
The aim of this study was to gain further insight into the extent of caregiving challenges, including perceptions of the impact of gender on work–life integration, balance, and boundaries. The onset of the COVID-19 pandemic allowed us to explore the impact of caregiving in a world transformed by a pandemic, and the FRCS provided unique access to physician-scientists known to have family caregiving responsibilities.
Materials and Methods
We conducted a qualitative descriptive study 11 to explore early-career physician-scientists’ experiences of caregiving during the COVID-19 pandemic. The full methods of the program evaluation were reported previously. 6 Briefly, we invited all 38 physician-scientists who received FRCS support in 2017 (the second cohort of awardees) to participate in semi-structured telephone interviews. These awardees received financial support for 1–2 years and could only use funds to cover direct research costs and could not use them to pay for dependent care costs. Of the 38 awardees invited, 14 consented and participated. We also analyzed written narratives in which applicants explained their unique caregiving responsibilities when they applied for the FRCS award. We received consent and obtained narratives from the 2020 cohort of awardees, which were selected to be contemporaneous with the 2020 interviews and to triangulate themes of the COVID-19 pandemic. This study was approved by the University of Michigan Institutional Review Board.
We conducted interviews between August and October 2020. We developed a semi-structured interview guide, which explored career development, caregiving responsibilities, reflections on the FRCS, and the impact of the COVID-19 pandemic.
Individual interviews were conducted by phone by two nonphysician interviewers and lasted 30–60 minutes. Audio-recorded interviews were transcribed by a professional transcription service. Transcripts were deidentified and compared to audio-recordings for accuracy. We additionally reviewed 19 written narratives of those who received the FRCS award in 2020. Narratives were approximately 1 page.
The interview transcripts and written narratives were uploaded to MAXQDA (VERBI Software, 2021) for data management and analysis.
Analysis
The data were analyzed iteratively through steps informed by the framework method to thematic analysis. 12 Members of the coding team read all transcripts and narratives, making analytical memos and noting any preliminary codes. Two lead coders then independently open-coded the same three transcripts and came to consensus on an initial codebook. A process of refining and applying codes iteratively was repeated until no new codes were generated and we had established a final codebook.
The coding team systematically coded each transcript and narrative using the final codebook and identified meaningful passages. The coding team met to discuss impressions and form themes. We were able to achieve information power 13 with an interview sample size of 14 and a written narrative sample size of 19, as determined by the specificity of our sample and quality of dialog that produced information-rich cases.
Results
Of the 14 interviews and 19 narratives included in this study, 25 awardees (79%) were women. This sample was representative of the broader pool of 2017 and 2020 awardees (76% women). Eighteen (55%) were less than 40 years of age and 11 (79%) were Caucasian. Nineteen (58%) awardees were caregivers to children aged 0–4 years old, and 6 (18%) were responsible for another adult or elder. See Table 1 for demographic details.
Characteristics of Awardee Interviews and Narratives Included in Qualitative Analysis
Respondents could report ages for more than one child.
Qualitative analysis identified that the caregivers in our sample of mostly women are burdened by strong feelings of guilt due to the unrealistic gendered expectations in the domestic sphere and workplace. This guilt was augmented by the effects of the COVID-19 pandemic, which led participants to experience emotional exhaustion and burnout. The thematic map (Fig. 1) illustrates the key findings of this study.
Theme 1: “The mom is always called first”—gendered caregiving responsibilities are perceived as unrealistically high and inescapable
Interviewees expressed that “caregiving tends to fall on the shoulders of … the moms” (Interviewee 08, White Female, 40s) (Table 2). On top of childcare expectations, many woman participants also shouldered other domestic responsibilities such as housework, eldercare, family health care, and schedule coordination. While many women expressed that they had supportive spouses, some noted that their husbands often took a “very different … approach” (Interviewee 12, White Female, 30s) to caregiving, often described as more hands off.
Theme 1: “The Mom is Always Called First”—Gendered Caregiving Responsibilities Are Unrealistically High and Inescapable
Participants described the following two primary factors that led to uneven distribution of childcare duties: (1) biological requirements of pregnancy and lactation and (2) gendered societal expectations surrounding childcare. Regarding the former, participant Interviewee 07 (White Female, 40s) described the “physical symptoms, … limitations, and … sleep deprivation” that came with pregnancy and breastfeeding, and how they “disrupt[ed] [her] work schedule.” These work disruptions and additional domestic responsibilities were unique to the birthing parents and could not be outsourced to the nonbirthing parent.
These biological differences were often exacerbated by societal expectations of gendered roles in childcare. Interviewee 04 (White Female, 40s) described difficulties delegating childcare duties to her husband due to gender biases of schools and day cares:
It doesn’t matter how you list phone numbers at school, but the mom is always called first.
While several interviewees hired nannies to off-load a portion of their caregiving responsibilities, many woman interviewees expressed that they “were not able to or interested” (Interviewee 14, Asian Female, 40s) in off-loading these responsibilities.
Men, on the other hand, described off-loading their caregiving responsibilities to their wives or hiring help:
She [my wife] did the lion’s share of the childcare but stuff that I did was kind of able to be supplemented with someone from outside to be able to come in. (Interviewee 09, White Male, 40s)
Several participants also served as health care navigators for their families. Interviewee 06 (White Female, 40s) attributed her large role in her mother’s care to being a woman:
My brother is retired and lives in the same town as my mom but I am the person who calls her every day, and has taken over her finances, and manages her doctor’s appointments, even though I have a nine hour drive away. … That is because I’m a woman – no question.
She suggested that women are more likely than men to be involved in eldercare, even when there are geographical barriers. This highlights the intersection of gendered caregiving and physician roles leading to women being pushed into health care navigator responsibilities, which required a lot of “time and energy” (Interviewee 12, White Female, 30s).
The women of color in our cohort also mentioned that the strong gendered expectations in eldercare and childcare were augmented by their cultural expectations. Interviewee 10 (Other Female, 40s) described herself as being from two cultural backgrounds, which both placed heavy responsibilities on women as caretakers. This intersection of gender and cultural identity increased time-consuming domestic obligations, limiting time for academic obligations.
Furthermore, one of our participants—a woman of color—described how biases against minoritized people made it more difficult and time-consuming to meet the same expectations placed on nonminoritized populations. She described an urgent need to be “engaged with [her] kids” to “buffer” the negative social constructs placed on minoritized men and women:
They were viewed as [minoritized] kids who really wouldn’t amount to much, and I see a pattern where they were not getting the attention that they needed… I had to … [be] in school a lot of the time so that it was clear that … they had parents that were involved and demanding that they get the attention that they require. (Interviewee 05, Other Female, 40s)
She observed that the education system and her community were not offering the same opportunities to her children as to their White peers, and she felt obligated to bridge this gap with her own time and effort, further reducing time and mental bandwidth available to focus on her professional pursuits.
The women in this sample, including the women of color, expressed feeling pressured by societal, racial, and gendered factors to take an enormous role in caregiving and were often unable to adequately off-load these responsibilities to others.
Theme 2: “People don’t expect … women to be … heavy hitting NIH researchers” — disadvantageous gendered roles in academic medicine led to the undervaluation of women
Compounded with heightened expectations around caregiving, women in this study also noted that gendered expectations in the workforce often limited their career advancement (Table 3).
Theme 2: “People Don’t Expect … Women to Be … Heavy Hitting NIH Researchers”—Women Are Overburdened by Disadvantageous and Undervalued Expectations at Work, Which Inhibits Academic Progress
Several participants noted that men were more likely to have stay-at-home spouses to shoulder extraprofessional responsibilities (Interviewee 02, White Female, 40s), whereas women did not (Theme 1). Thus, when they were compared academically to their male colleagues who had fewer commitments outside of work, these standards had a “differential impact” (Interviewee 06, White Female, 40s) and “[made] it harder to keep up as a woman” (Interviewee 13, White Female, 40s).
In addition to their substantial duties at home, many women also described being pushed into time-consuming, menial tasks or committees that did not contribute to their career advancement:
There is an assumption that women will kind of do the cleaning up work, the crossing T’s and dotting I’s work. … There is an assumption that women will do a lot of the heavy lifting but, somehow, that men end up getting credit for it. (Interviewee 06, White Female, 40s)
She pointed out that there is still a workplace culture where women are responsible for secretarial work, whereas men are allowed to focus on the bigger picture.
On the department scale, multiple women described being pushed into certain roles that were time consuming but undervalued:
There is a lot of value in education; however, from an academic perspective there’s not a lot of return on that investment… If I’m not careful I get pushed into education efforts. (Interviewee 12, White Female, 30s)
More broadly, one woman academician expressed that women were less likely to be in “king specialties”, meaning specialties which were more competitive and higher paid, which led to women in her institution making “on average, … $25,000 less than men” (Interviewee 04, White Female, 40s). In sum, women are spending their already limited time at work on undervalued tasks, which contributes to women being siloed into underpaid and undervalued positions.
In contrast, one male academician felt that his gender played a role in his department’s feedback to prioritize leadership opportunities over his caregiving responsibilities:
They…[replied]… that as a White male your role is really in the medical center in a leadership position, that you should have someone to take care of this [caregiving responsibilities] for you. (Interviewee 11, White Male, 40s)
Compared with the women in this study, Interviewee 11 (White Male, 40s) was encumbered by the expectation that men should pay less attention to home duties, while focusing on academic ambitions.
These gendered differences were pronounced for the women of color in our study. They expressed that less was “expected of [them]” at work because of their race and that they were less likely to be acknowledged (Interviewee 05, Other Female, 40s):
[My attending] said to me, “You are a [minoritized race] woman with an accent, nobody is going to listen to you. (Interviewee 05, Other Female, 40s)
Another interviewee of color felt that she was being “manipulated” into doing menial tasks at work, but was unable to “fight against that” because of strong cultural principles of not “going against an authoritarian figure” (Interviewee 10, Other Female, 40s). As a result, she felt underqualified and unable to promote herself for fair pay.
Theme 3: “Maintaining productivity has become untenable”—work–life expectations were exacerbated by the aftereffects of the COVID-19 pandemic
The COVID-19 pandemic introduced drastic changes in work–life expectations that disproportionately affected women with caregiving responsibilities (Table 4). Depending on the provider’s specialty, participants experienced a major increase in clinical duties, such as those working in the ICU, an increase in administrative and academic duties, or both. Participants described ways in which this unpaid and often unrecognized work that was already disproportionately placed on women increased during the pandemic.
Theme 3: “Maintaining Productivity Has Become Untenable”—Work–Life Expectations Were Exacerbated by the COVID-19 Pandemic
For many in our study, research productivity was tied to their evaluations and promotion. The pandemic directly impacted research productivity as research projects became “logistically non-tenable” (Interviewee 03, White Female, 30s), and had to be “shut down” (Interviewee 01, White Male, 40s) to respect hospital policies. Interviewee 13 (White Female, 40s) described having a “harder time helping people in the lab analyze data” via Zoom compared with in person and felt that work “was taking longer and [was] more difficult to do.” Many participants perceived that COVID increased the burden of administrative assignments, while making it more difficult to carry out those activities that are important to career advancement.
Nearly all participants expressed hardships with the decrease in access to childcare and eldercare, with one interviewee calling it an “absolute nightmare” (Interviewee 14, Asian Female, 40s). Parents were expected to take on the duties of “childcare, virtual learning and mobility” (Narrative 01, White Female, 30s), which “require[d] more coordination” (Interviewee 12, White Female, 30s), time, and effort. Women, already faced with an expectation to take on the majority of caregiving responsibilities, faced enormous increases in their responsibilities during the pandemic due to remote schooling and decreased access to help:
We had to let her [the nanny] go because … we cannot have somebody… coming in and out of our house. So, that was one of the things that we lost, that I lost. (Interviewee 10, Other Female, 40s)
Many participants also experienced WFH for the first time during the pandemic:
They call it working from home. It should be called living at work, right, because, … there really is no separation. (Interviewee 02, White Female, 40s)
Physically going to work allowed separation between work and home duties, but enforcing this separation in the WFH era caused new and significant guilt:
There’s the guilt of being sort of up here in the bedroom when everyone else has like crazy things happening. … And those are things I feel like I should attend to even though I know that like this normally would happen, and I would be at work and I would not even hear it and I would not know about it. (Interviewee 01, White Male, 40s)
Physicians used to off-load childcare duties to schools or other caregivers. However, WFH forced physicians to see their home and work responsibilities in the same space and forced them to choose which is more important every minute of the day. That stress of needing to constantly prioritize one while ignoring the other led to increasing guilt.
Theme 4: “Momma, are you happy?”—unrealistic caregiving and work expectations lead to guilt, stress, burnout, and workforce attrition
Women in our study described how failing to meet unrealistic caregiving and work expectations which were further heightened by the COVID-19 pandemic led to feelings of guilt, which contributed to stress, burnout, and, in some cases, pushed individuals to consider leaving academic medicine (Table 5).
Theme 4 “Momma, Are You Happy?” The Unrealistic Caregiving and Work Expectations Lead to Guilt, Stress, Burnout, and Workforce Attrition
Many participants expressed feeling “a sense of guilt that [they] don’t do more for [their] family” (Interviewee 11, White Male, 40s). One female participant felt “ashamed that [she] couldn’t just … manage it all” (Interviewee 08, White Female, 40s). If woman physicians are expected to do more in the household compared with men, then women are more likely to fall short of these unrealistic expectations, which provides more occasion for them to feel guilty about their perceived failures. One prominent example was Interviewee 07 (White Female, 40s) detailing her conversations with her son:
I think there are days when I am less able to enjoy my children and be present with them. … My son, who is about to be four, can tell. Like he will ask questions like, ‘Momma, are you happy?’ which I think is him reading that I am like kind of tuned out or just exhausted. And that makes me sad.
She had an ideal of herself as a parent, but when her work and caregiving expectations become overwhelming to the point of exhaustion, she described feelings of guilt about not upholding her duty of being a “good” and engaged mother.
This same guilt also persisted in unmet workplace expectations. There were varying opinions within our cohort as to whether women were held to higher, similar, or lower standards compared with their male colleagues. The majority felt that “expectations are similar … for men and women” (Interviewee 13, White Female, 40s), but that trying to achieve these same benchmarks was harder for women because of the significant gendered imbalances of demands on their time. Many woman participants expressed a need to prove their value at work and exceed expectations to avoid being seen as underperforming:
There’s a fear of looking like you can’t hack it if you ask for help but, especially, as a woman, especially as a mom. (Interviewee 08, White Female, 40s)
She additionally saw her personal failures as being reflective not only of herself but also of all women and mothers, which augmented her fear and guilt.
Many in this study additionally described feeling “anxious” (Interviewee 02, White Female, 40s), “emotionally exhausted” (Interviewee 04, White Female, 40s), and “burnt out” (Interviewee 07, White Female, 40s):
I [felt] a lot of emotional fatigue when I was in clinic and [I think I cried like] every night …, you know, just feeling bad for what my patients were going through and, …, then also feeling bad that my kids were missing out on school and being with their friends. (Interviewee 12, White Female, 30s)
Our interviewees already had a precarious work–life integration, so the additional stressors during the pandemic made the situation for many almost untenable.
Interviewees cited leaning on their families, mentors, and the financial support from FRCS to cope with these worsening stressors:
I don’t think I would have continued if I didn’t have that [FRCS] support because it was just impossible. (Interviewee 05, Other Female, 40s)
Although some interviewees mentioned institutional policies or programs aimed at alleviating these stressors, they were too “expensive” (Interviewee 02, White Female, 40s), too oversaturated such that there was “not enough availability” (Interviewee 02, White Female, 40s), or simply “not enough” (Interviewee 06, White Female, 40s).
Several women additionally coped by “slowing things down” and “saying no” to professional opportunities (Interviewee 08, White Female, 40s). A few of our interviewees felt they couldn’t meet all their expectations at work and either took a step back from career advancement or considered leaving academic medicine altogether:
I think my academic career is going to end. … I choose to do a bad job on my research work … so that I can spend time with my kids, so I can be present, so I can sleep, so I can exercise. Like every day I am consciously choosing to do a bad job in some aspect of my professional development, so it was like to preserve my family. (Interviewee 07, White Female, 40s)
This illustrates how the unrealistic expectations placed on women in their homes, coupled with the intense pressures placed on early-career academic physicians, leave many women with a feeling of having to choose between their careers and their families.
Discussion
In this qualitative study of early-career physician-scientists with extraprofessional caregiving responsibilities, we found that expectations around caregiving and domestic work were particularly acute for women and often conflicted with traditionally defined career success. Failing to meet these expectations resulted in noteworthy guilt, stress, burnout, and considerations of leaving academic medicine. This was exacerbated when caregiving demands increased during the COVID-19 pandemic.
Previous studies identified gendered differences in caregiving and work expectations, including the concept of “intensive mothering” where mothers are expected to devote more time and energy to childcare than fathers. 14 –16 This concept holds for woman physician-researchers. 5,14 In our study women were also subject to the “motherhood penalty,” a bias that assumes that women are less committed to their jobs due to caregiving responsibilities. 14,15
Women are often held to the same ideal worker norm as men, which requires a relentless employee dedicated to their paid work without allowing their personal lives to intervene. 16,17 This is disadvantageous to women given the time demands of intensive mothering. This ideal worker norm is enhanced by the “culture of bravado” in medicine, which can contribute to self-neglect and burnout. 17 Motherhood is also portrayed culturally as a self-sacrificing pursuit; 15 thus physician-mothers may be particularly prone to self-sacrifice and self-neglect. Meanwhile, men may face pushback when they prioritize family over work, which further pushes caregiving burdens onto mothers. 18 The COVID-19 pandemic further exacerbated these gendered work–life challenges. 19
Intensive mothering and the ideal worker norm, combined with gendered differences in clinical practice and office housework, reinforce the idea that time is a valuable commodity in academic medicine. 6 This work–family time conflict can bring about work–family guilt, which is worse in women. 20,21 The increased guilt that mothers have surrounding childcare and housework compared with fathers has been termed the “guilt gap.” 22 Our study points to a work and family guilt gap contributing to higher levels of stress, exhaustion, and burnout in women in academic medicine. 23,24 With less time to dedicate to career-advancing opportunities and higher work–family guilt, women in academia experience increased anxiety, are less likely to achieve independent grant funding 25 and high-level leadership positions, 26 and experience higher rates of attrition. 27 Women are also prone to experiencing guilt when using family-supportive policies due to concern for potentially negative personal and professional consequences. 28
Our study participants viewed the FRCS as a valuable tool for work–life integration, which is consistent with our prior qualitative work with FRCS recipients prior to the pandemic. These earlier participants reported that the FRCS flexible funds allowed them to allocate more time to career advancement and caregiving responsibilities, while also reducing the stigma and emotional strain associated with caregiving. 6,9,10 The flexible funds structured to relieve the tension between competing time demands in home and work–life align with a National Academy of Sciences report which recommends implementing and normalizing policies that support family caregiving and childbearing. 29 Continuing to add and expand similar programs could be instrumental in promoting the retention of women in academic medicine.
One limitation of our study is the small sample size; however, this unique cohort of academic physicians with significant caregiving responsibilities provides an illuminating perspective. Another limitation is the fact that the analytic team was all-female, although including diverse racial and professional backgrounds (sociology, psychology, medicine, and public health), which enriched the analysis. Finally, our study population had few underrepresented in medicine and no LGBTQIA representation, which limits our ability to analyze the intersectional impact of multiple marginalized identities. Future studies should consider oversampling for these characteristics.
This study provides a rich understanding of the gendered expectations within academic medicine, how the COVID-19 pandemic and WFH exacerbated these challenges, and the guilt that results when these expectations are not met, particularly for women with significant caregiving responsibilities. Providing resources to support this population is essential for the development and retention of a diverse workforce in academic medicine.
Authors’ Contributions
J.T.: data curation, formal analysis, writing—original draft. L.S.: conceptualization, investigation, methodology, data curation, formal analysis, writing—original draft. R.D.J.: conceptualization, investigation, methodology, data curation, formal analysis, writing—review and editing. L.P.: data curation, formal analysis. L.B.: conceptualization, writing—review and editing. G.D.: conceptualization, writing—review and editing. W.D.: conceptualization, writing—review and editing. H.C.: conceptualization, writing—review and editing. C.M.: writing—review and editing. B.M.: conceptualization, writing—review and editing. J.R.: conceptualization, writing—review and editing. R.J.: supervision, funding acquisition, conceptualization, methodology, formal analysis, writing—review and editing. All authors contributed to and approved the final version of the article.
Author Disclosure Statement
R.J. reports funding from the
L.B., G.D., W.D., C.M., B.M., and J.R. report funding from the
Footnotes
Funding Information
This work was supported by the Doris Duke Charitable Foundation. The funders played no role in the decision to submit for publication.
Ethics Approval
This study was approved by the University of Michigan Institutional Review Board # HUM00111446.