
Abstract
Background:
The postpartum period is a window to engage birthing people in their long-term health and facilitate connections to comprehensive care. However, postpartum systems often fail to transition high-risk patients from obstetric to primary care. Exploring patient experiences can be helpful for optimizing systems of postpartum care.
Methods:
This is a qualitative study of high-risk pregnant and postpartum individuals. We conducted in-depth interviews with 20 high-risk pregnant or postpartum people. Interviews explored personal experiences of postpartum care planning, coordination of care between providers, and patients’ perception of ideal care transitions. We performed thematic analysis using the Capability, Opportunity, Motivation, Behavior (COM-B) model of behavior change as a framework. COM-B allowed for a formal structure to assess participants’ ability to access postpartum care and primary care reengagement after delivery.
Results:
Participants universally identified difficulty accessing primary care in the postpartum period, with the most frequently reported barriers being lack of knowledge and supportive environments. Insufficient preparation, inadequate prenatal counseling, and lack of standardized care transitions were the most significant barriers to primary care reengagement. Participants who most successfully engaged in primary care had postpartum care plans, coordination between obstetric and primary care, and access to material resources.
Conclusions:
High-risk postpartum individuals do not receive effective counseling on the importance of primary care engagement after delivery. System-level challenges and lack of care coordination also hinder access to primary care. Future interventions should include prenatal education on the benefits of primary care follow-up, structured postpartum planning, and system-level improvements in obstetric and primary care provider communication.
Introduction
The postpartum period is a window of opportunity to engage birthing people in their long-term health by facilitating connections to primary care. Birthing people are at risk for severe morbidity and mortality in the year after delivery; 1,2 approximately half of pregnancy-related deaths occur postpartum, 60% of which are thought to be preventable with consistent, timely access to care. 2,3 High-risk pregnancies such as those affected by hypertensive disorders or gestational diabetes are known to signal increased risk for adverse health outcomes beyond the reproductive years. 4,5 Despite the accepted role of longitudinal care during this period in the lifecourse, 6 postpartum care in the United States is underutilized and fragmented. 7,8 Traditionally, postpartum patients complete one visit with their obstetric provider (OB) at 6 weeks postpartum, but attendance is poor, 9 content is insufficient, 8,10 and this single visit is late in timing and inadequate to fully address needs. 2 Postpartum systems also fail to transition patients from OB to primary care providers (PCP). Rates of primary care engagement after delivery are at best 50%, with significant disparities among individuals from marginalized communities. 11 –13
The structure of postpartum care is shifting toward a more patient-centered model. The American College of Obstetricians and Gynecologists (ACOG) recommends an initial assessment within 3 weeks postdelivery followed by a comprehensive visit by 12 weeks and a handoff from an OB to a PCP for those with chronic conditions or pregnancy complications. 14 To leverage this moment of care to impact maternal health, particularly for high-risk individuals, there is a need for interventions that increase patient engagement and strengthen interprofessional relationships between pregnancy care providers and PCPs.
Successful interventions will change behavior to target the factors that shape a person’s ability to engage in health care postpartum. The Capability, Opportunity, Motivation, Behavior (COM-B) model conceptualizes the personal and environmental factors that interact to enable a behavior. 15 For a behavior to take place, COM-B posits that an individual must have the capability, motivation, and appropriate opportunity to act (Fig. 1). The model identifies the following six components: physical capability (skills), psychological capability (knowledge), physical opportunity (environment), social opportunity (sociocultural norms), automatic motivation (emotions and impulses), and reflective motivation (evaluation and planning). 15 COM-B has been used to guide the design of public health interventions, 16 including in obstetrics settings, such as promoting weight management in pregnancy 17 and lifestyle modification after gestational diabetes. 18,19 COM-B can be applied postpartum to map the factors that prevent or facilitate care engagement and care transitions in the year after delivery.

The Capability, Opportunity, Motivation, Behavior framework applied to postpartum care engagement, adapted from Michie et al., 2011. 15
Using the COM-B theory of change as a guiding framework, our study explored how high-risk birthing people access postpartum health care. We also examined how this population navigates the transition between obstetric care and primary care and ways this transition could be optimized.
Materials and Methods
Study design
This is a qualitative study using semistructured, in-depth individual interviews and thematic analysis. This study received appropriate IRB exemption and is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research. 20
Setting and participants
We used convenience sampling to recruit participants via social media and flyers in both ambulatory and inpatient obstetric care settings of two large academic hospitals in the Northeastern United States. We also identified and reached out to potential participants at a postpartum transition clinic for hypertensive pregnancies 21 to intentionally sample from a population with complex needs. Eligible participants spoke English, were 18 years or older, and currently in the third trimester or within 1 year postpartum. We limited participation to those who would most benefit from primary care follow-up, defined as individuals with a chronic condition or pregnancy complication and/or those with social complexity, such as housing or financial instability (see Participant Characteristics). Prospective participants were screened for eligibility through a Qualtrics (Provo, UT) intake form, which also collected self-reported sociodemographicinformation. When medical or social neeeds were identified on the intake form, prospective participants were offered appropriate follow up and social services. If eligible for enrollment, participants were contacted by a member of the research team, provided study information, and asked to complete a verbal consent process to schedule a virtual Zoom interview. 22
Data collection
SP, JK, and AW conducted individual interviews between September 2021 and March 2022. We used a semistructured interview guide to ask about barriers and facilitators of postpartum care engagement and care transitions. The guide consisted of open- and closed-ended questions with systematic probes to capture information on specific actions such as seeing a PCP. Questions explored preferred sources of support and care postpartum, postpartum care planning, care organization between providers, and ideal postpartum care and care transitions. Participants received a $50 gift card upon interview completion. Interviews were audio recorded, anonymized, and manually transcribed verbatim by SP and AW. Recordings were deleted after transcription and analysis.
Reflexivity statement
Two of the interviewers (SP and JK) had extensive experience in qualitative research and all three (SP, JK, and AW) had experience in reproductive research. While conducting interviews, SP and AW were both graduate students with public health training and a background in clinical medicine. JK was an academic researcher with years of experience in qualitative methodology. Those most closely involved in data acquisition and coding analysis (SP, AW, and JK) met regularly with the larger research team, including individuals with strong backgrounds in qualitative research (JM), data synthesis (AK), and both clinical research and clinical care (AC and CZ) to discuss emerging codes and interpretations of texts.
Data analysis
A deductive codebook was created and mapped to the interview guide and principles of COM-B. The codebook was amended with inductive codes as themes emerged from the data. SP and AW coded transcripts using NVivo (March 2020). Thematic analysis was guided by code saturation, the point at which a range of subthemes related to the study questions are identified and no new subthemes appear in subsequent interviews. 23,24 Code saturation aims to identify the full spectrum of subthemes rather than all dimensions of a given subtheme. Team meetings were held throughout the coding process to establish intercoder agreement at the beginning (by way of double-coding 10% of transcripts and working through areas of disagreement), discuss subsequent application of codes, reach consensus on adding new codes to the codebook, and assess for code saturation.
Results
Participant characteristics
We interviewed 20 high-risk pregnant or postpartum people, averaging 34 minutes per interview. Six participants (30%) were patients of the postpartum transition clinic for hypertensive pregnancies. Participants’ mean age was 33.5 years and the majority were postpartum (85%), primigravid (65%), privately insured (80%), and highly educated (100% at least some college). Sixty-five percent of participants identified as white, 20% as Asian, and 10% each as Middle Eastern or Black. Participants experienced a range of chronic and pregnancy-related conditions, the most common of which were hypertensive disorders, asthma, gestational diabetes, and abnormal placentation (Table 1).
Participant Demographics (n = 20)
Selected more than one category.
Missing data.
Findings
Overall, barriers to care were mentioned more frequently than facilitators. We found the highest density of responses within the Psychological Capability (knowledge) and Physical Opportunity (environment) subcategories of COM-B (Fig. 2). Within Psychological Capability, participants described an overwhelming lack of knowledge and guidance around postpartum care expectations, reporting limited prenatal counseling regarding appropriate postpartum follow-up (Table 2). Within Physical Opportunity, barriers included difficulty balancing the needs of newborn and maternal health, a lack of standardized and routine postpartum follow-up, limited appointment availability, and lack of resources (insurance noncoverage, transportation/financial issues). Other less commonly mentioned barriers included distrust in the medical system/medical providers and mental health stigma (Social Opportunity) as well as birth trauma (Automatic Motivation). Alternatively, facilitators to care (Table 3) included knowledge and skills acquired from a prior pregnancy (Physical Capability), social support and community resources (Social Opportunity), and streamlined care through postpartum care plans (Psychological Capability) and care coordination (Physical Opportunity).
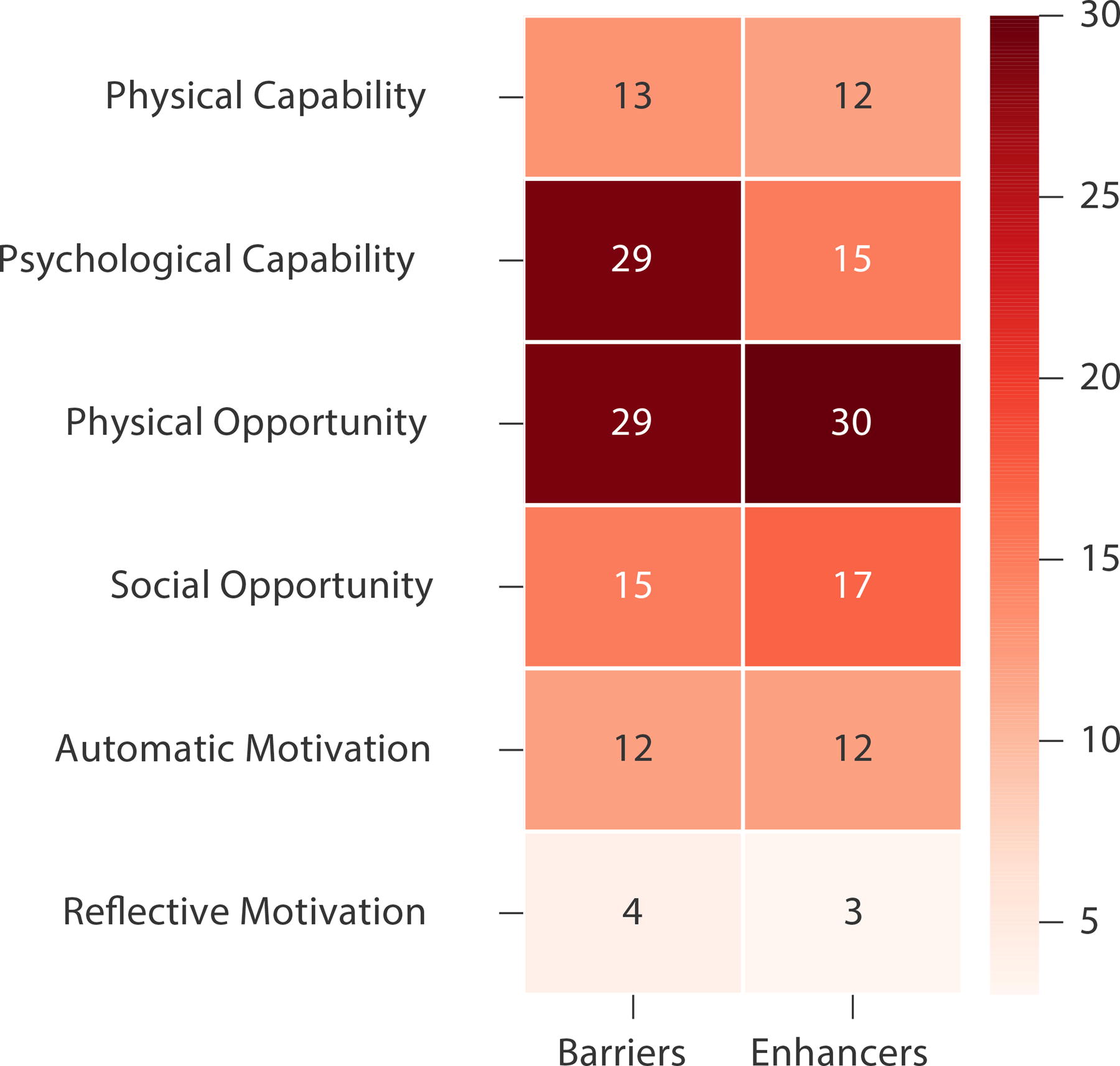
Heatmap demonstrating the frequency of participant responses categorized by Capability, Opportunity, Motivation, Behavior subdomain (darker = higher frequency, number of mentions denoted in each category).
COM-B: Barriers to Accessing Support and Medical Care Postpartum
COM-B: Facilitators to Accessing Support and Medical Care Postpartum
Barriers: Limited routine follow-up, lack of preparation, and no standardized transitions
Participants commonly reported insufficient knowledge about who to contact and how to access care postpartum (obstetric and primary care) in addition to facing structural barriers such as a lack of available appointments. The most significant barriers were limited routine follow-up, lack of preparation for the postpartum period, and no standardized transitions from obstetrics to primary care (Table 2).
Seventy percent of participants expressed frustration over the limited routine follow-up and the fragmentation of care they experienced in the months following delivery. People discussed the contrast between the frequency of prenatal appointments before birth and the lack of similar continuity after delivery, noting, “I definitely felt like it was off that up to having a baby I’d have visits every single week and then after it’s like nothing.” Participants also felt that a single 6-week visit was “insufficient,” and wanted more postpartum touchpoints with their OB, saying, “I really do feel like there needs to be at least six months follow-up with your OB. I’m four months postpartum and I still don’t feel back to myself.”
Participants reported being especially unprepared for navigating care after their 6-week postpartum visit, noting a lack of official guidance on the next steps. One participant commented:
“I didn’t know if I call my OB, if I call my PCP…does my OB even consider me a patient anymore? You don’t even know who to talk to.”
This care fragmentation caused some participants to inadvertently delay important medical care.
“I definitely have some postpartum depression or anxiety. Maybe if I was seen routinely since delivery, we would’ve figured it out sooner.”
Along with unclear guidance, participants were not aware of the role and scope of primary care in managing their postpartum concerns. Most participants lacked a formalized hand off from their OB to a PCP and found this transition difficult to manage on their own.
“You’re done with OB and you have primary care, but they don’t necessarily specialize in what’s going on with you…you tell your story and give all the information again and ‘am I telling them all my right symptoms?’ It makes it more confusing and burdensome.”
Other participants were unable to schedule appointments with their PCP because of limited availability and provider turnover. This lack of continuity often resulted in further lapses in care and feeling isolated from the medical system.
“I think it’s just the nature of the PCP world…They just keep changing, leaving…So I don’t really view them as a resource although I know that they’re there.”
In addition, some participants felt reluctant to transition back to primary care during the postpartum period. They struggled leaving their OB saying, “that’s who I’d been seeing so much being pregnant and we had spent so much time together over the past few months.”
Facilitators: Postpartum care plans and care coordination
Participants who most successfully engaged in care had clear postpartum care plans, coordination between obstetrics and primary care, and access to material resources, including support at home, financial stability, and parental leave (Table 3).
Postpartum care plan and organized communication between OB and PCP providers were the most significant facilitators to care transitions. Participants found it helpful to have simple “bullet points of what you should be doing, what are the sources, where should we contact, and what should the next steps be.” After learning about ACOG’s model of postpartum care plans, one participant commented, “I personally did not realize how hard that fourth trimester was gonna be. When you mentioned, ‘did they have a postpartum care plan?’ I wish that was a formal thing they did.”
Participants from the postpartum transition clinic reported the most confidence in their ability to follow up with primary care. Speaking of her provider, one participant noted, “once she got me somewhat stable, she then transitioned my care over to my PCP. It was a very gradual thing from one person to another person. It wasn’t like they just released me cold turkey and were like sink or swim.” Another participant said working with providers at the transition clinic felt similar to “a huge weight” off her shoulders because she finally had a provider who “listened,” “had a plan,” and “looked at [her] whole picture.”
Discussion
Despite the clear benefits of primary care reengagement, high-risk postpartum individuals encounter numerous obstacles to continuity of care. Through the lens of COM-B, our results suggest that high-risk pregnant and postpartum people receive inadequate counseling on the importance of postpartum care transitions (Psychological Capability) and have limited individualized planning for meeting their postpartum needs (Physical Opportunity). Participants expressed dissatisfaction with a perceived lack of ownership of their care by health care providers and wished for more routine, organized postpartum follow-up. Our findings also demonstrate the ongoing gap between ACOG’s postpartum recommendations and current practice; high-risk postpartum people continue to lack a standardized method of transitioning from obstetric to primary care.
Our results are consistent with other qualitative studies showing that postpartum people are unprepared for navigating the health care system after delivery. 8,10,25 Similar to our study, Martin et al. found that postpartum people were frustrated with the significant time delay between delivery and their first follow-up at 6 weeks postpartum. 25 Exploring the lived experiences of postpartum mothers, Tully et al. found that birthing people often feel overwhelmed and struggle not knowing who to contact about their health concerns postpartum. 10 Our study clarifies that time delays and knowledge gaps extend beyond obstetric follow-up and into primary care transitions. There is a specific need for education on how to access medical care beyond the traditional 6-week postpartum visit. This gap represents a missed opportunity for individuals with high-risk pregnancies needing follow-up after delivery. 26,27
Even with advantages conferred in the contemporary United States by private insurance, education, and whiteness, our participants still identified structural and systemic barriers to engagement with care. In particular, “insurance churn” after delivery 28 and national shortages of primary care providers 29 are structural factors that impact a patient’s ability to maintain access to care postpartum. Participants highlighted lack of access to and availability of primary care appointments as a barrier to effective transitions. High-risk individuals from communities impacted by racism and poverty face these and additional social and structural barriers that further inhibit primary care reengagement and contribute to suboptimal outcomes. 11,30
Individualized care planning, postpartum patient navigation, and postpartum transition clinics may address knowledge gaps and health system-level barriers. Participants in our study loudly echoed a sense of confusion around how and where to access medical care postpartum. Beginning as early as the first prenatal visit, pregnancy care providers may optimize anticipatory guidance during prenatal appointments to facilitate connections to care after birth. Identification of a PCP or medical home where patients, and possibly their baby, will receive long-term care can be a first step in this process. Routine prenatal counseling should include an individualized discussion of medical conditions and health risks in the postpartum period and the importance of transition of care to a PCP. Building this conversation into prenatal care and repeating this message can empower patients to establish a connection or reconnection with a PCP before delivery, which is especially important in areas with poor PCP availability. Using prenatal visits to lay the foundation for the importance of postpartum follow-up may begin to fill knowledge gaps and set realistic expectations for our patients. Participants also benefited from clearly delineated follow-up instructions as well as coordinated “warm handoffs” between medical providers. Participants who used a transition clinic had an additional medical provider dedicated to stabilizing their immediate postpartum medical and social needs before facilitating a transition back to primary care. In one recent estimate, rates of primary care reengagement from a postpartum transition clinic were 79.5%. 21 Many study participants noted a lack of primary care availability as a barrier to care; transition clinics provide an avenue for essential care immediately following delivery until care can be established with a PCP.
Postpartum patient navigators are another promising opportunity. Patient navigators are trained, nonmedical personnel who facilitate engagement with health care by identifying and overcoming patient-specific barriers to care. 31 Navigating New Motherhood, a postpartum navigation program in Chicago, Illinois, has found success using patient navigators to increase attendance at postpartum visits. 32 In this pilot program, patient navigators addressed many of the barriers raised by participants in our study by helping to schedule postpartum appointments, provide appointment reminders (via phone, text, or e-mail), offer food and transportation resources, and facilitate connections to mental health care providers and psychosocial support. 32 Patient navigation programs and postpartum transition clinics attempt to mitigate many of the structural barriers identified by our participants, however, higher level system changes are still needed.
National groups such as the “Bridging the Chasm Collective” have outlined key items for improving health beyond pregnancy, including care systems that encourage collaboration between maternity care and primary care. 33 Informed by our findings, future interventions may build on those outlined in the “Bridging the Chasm” report and should include the following: prenatal education on the benefits of primary care follow-up; structured risk assessments and postpartum planning; system-level improvements in obstetric and primary care provider communication; and integration of support services such as postpartum patient navigation and doulas and other community perinatal professionals.
Strengths and limitations
Exploring barriers and enhancers through the COM-B framework strengthened our study by rooting our analysis in a robust theory of behavior change. Despite this strength, it was at times difficult to categorize our findings given the interrelatedness of the COM-B subdomains (Fig. 1). For example, participants who lacked the knowledge (psychological capability) of how and where to access care also tended to lack the skills (physical capability) for arranging appropriate appointments. When issues arose, we discussed among our team to reach consensus. This also illustrates the complexity of the factors that inform care seeking behavior postpartum.
As is inherent to any qualitative study, the generalizability of our findings has limitations. Participants were recruited through self-selection in a convenience sample. This self-selection may have impacted the types of experiences captured in our study. As referenced above, our study population was largely white, highly educated, privately insured, and receiving care at large academic medical centers. While their experiences may not be representative of pregnant and postpartum people more broadly, the number of barriers identified by a well-resourced group of participants who were largely protected from structural and systemic racism is notable. We suspect our study underrepresents the barriers faced in the year after birth, especially for those who experience racism and other systemic, social, and structural barriers.
Conclusions
Understanding the factors that influence postpartum care seeking behavior is essential for designing patient-centered interventions and systems that support continued access to quality care. Structuring this information within the COM-B framework further clarifies opportunities for meaningful intervention. The barriers and facilitators we identified highlight the need for ongoing interdisciplinary approaches to improve maternal health outcomes. 34 Our findings may also have implications for other disciplines with well-described gaps during transitions of care, including transitions from pediatrics to adult medicine, 35 postoncology cancer care, 36 and posthospital discharge. 37
Footnotes
Acknowledgments
The authors would firstly like to thank the participants, who generously donated their time and expertise to this study. They would also like to recognize the contributions of countless individuals at Ariadne Labs, most especially Jasmine Kaduthodil. Additionally, assistance with graphic design was provided by John Lazar.
Authors’ Contributions
S.E.K.P.: Conceptualization, investigation, formal analysis, writing—original draft, and visualization. A.C.C.: Conceptualization and writing—review and editing. J.M.: Methodology, validation, and formal analysis. A.W.: Investigation, formal analysis, and writing—review and editing. A.K.: Writing—review and editing. C.A.Z.: Conceptualization, writing—review and editing, and supervision.
Author Disclosure Statement
The authors report no relevant disclosures or conflicts of interest.
Funding Information
This project was partially supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (DHHS) under grant