
Abstract
Background:
Protection against postpartum depression is a commonly cited maternal benefit of breastfeeding. However, recent studies have found that negative breastfeeding experiences may actually increase the risk of depressive symptoms.
Objective:
To investigate women’s self-reported associations between breastfeeding experiences and depressive symptoms on a social media platform.
Study Design:
An electronic search was conducted on Reddit of all original user posts using keywords “breastfeeding” and “depression” from February 2013 to July 2021. Relevant posts and corresponding comments were manually extracted, evaluated for inclusion and exclusion criteria, and analyzed for thematic content.
Results:
In total, 584 entries was analyzed. Mothers most frequently described difficulty breastfeeding as the cause of new onset mental health symptoms (53%); however, mothers breastfeeding without difficulty were also susceptible (20%). Mothers also reported exacerbated preexisting mental health symptoms—predominantly related to difficulty breastfeeding (17%), but again, others experienced no difficulty (6%). Common words included among all entries were “guilt” (17%), “fail” (14%), “pressure” (7%), “shame” (6%), and “alone” (6%). Among mothers mentioning bonding (n = 99), 58% reported that breastfeeding inhibited infant bonding, versus 1% enhanced bonding; furthermore, 63% reported increased bonding after switching to formula versus 8% unchanged and 6% decreased bonding. Nearly one-quarter (23%) of all posts described inadequate breastfeeding counseling. Finally, 9% of all posts reported a negative experience with health care providers versus 6% a positive experience.
Conclusions:
Mothers struggling to breastfeed may not experience the classically described benefits of breastfeeding, instead experiencing increased depressive and other mental health symptoms and impaired maternal–infant bonding. Furthermore, limited provider disclosure about potential breastfeeding challenges and alternatives to breastfeeding may exacerbate mental health symptoms associated with breastfeeding difficulties. Balanced information should be presented to mothers contemplating breastfeeding in order to minimize maternal perceptions of “failure.”
Introduction
Breastfeeding has classically been associated with numerous health and relationship benefits for both mother and baby, including protection against postpartum depression (PPD). 1,2 In a study cited by the Surgeon General, researchers found that women who bottle-fed versus breastfed their infants were twice as likely to screen positive for PPD. 3 As a result of such health benefits, significant efforts have been made to have all new mothers breastfeed. Hospitals are under pressure to encourage breastfeeding to earn a “Baby Friendly” designation, and women feel pressure by shared goals to breastfeed exclusively for six months (with continuation for 2 years). 1,4,5 Recently, questions have been raised about the universality of breastfeeding benefits. Although positive breastfeeding experiences, characterized by high maternal breastfeeding satisfaction and self-efficacy and positive emotions during infant feeding, have been associated with lower rates of PPD, negative breastfeeding experiences may conversely increase depressive symptoms among mothers. 6 –8 Studies have found that mothers who face breastfeeding challenges, including poor infant latching, breast pain, breast infection, and low milk supply, exhibit increased depressive symptoms. 6,9 Studies have also found that maternal breastfeeding intention plays a role in the development of adverse mental health outcomes. Specifically, mothers with unmet breastfeeding expectations—that is, mothers who plan to breastfeed but cannot—exhibit higher rates of PPD than mothers who never intended to breastfeed. 10 Suggested moderating factors include maternal self-compassion, body functionality or image, and parental authenticity. 11,12
Breastfeeding has also been associated with enhanced maternal–infant bonding. 13,14 In a study cited by the American Psychological Association (APA), researchers found that breastfeeding status predicted toddler attachment security. They also found a direct correlation between breastfeeding duration and increased maternal sensitivity, persisting throughout childhood. 15 However, recent data have challenged the application of these findings to women who struggle with breastfeeding and/or depression. In one study, researchers found that mothers who experienced breastfeeding difficulty and/or PPD were more likely to report lower levels of bonding than mothers who did not experience these problems. 16
The present study examines mothers’ self-reported associations between breastfeeding and PPD based on anonymous and unprompted maternal narratives found on the social networking site Reddit. Social media presents a unique avenue for patients to express their uncensored, intimate thoughts without feelings of vulnerability, or fears of stigmatization that can accompany the usual in-office visit. This study aimed to highlight novel feelings, attitudes, and experiences that may not have been captured through previous, more traditional, investigations of the adverse impacts of breastfeeding.
Materials and Methods
This study was determined not to involve human subjects by the Western University Human Subjects Committee (Project #1735647–1). Data was collected exclusively from publicly available online social media content through the platform Reddit. Anonymity was maintained, with any personal identifying information excluded during data collection. All data was manually analyzed and coded by the authors of this study to preserve the meaning of each entry.
Data collection
An electronic search was conducted on Reddit including all original user posts with both keywords “breastfeeding” and “depression.” Data collection began with posts dated July 23, 2021, and continued retrospectively until February 12, 2013, when all available posts had been exhausted. Each post was individually evaluated and selected for inclusion if it met the following criteria: (1) the post described a mother’s personal experience with breastfeeding and associated mental health symptoms; (b) this was the post’s primary focus; (c) the post was written by the affected mother or a well-informed spouse; and (d) the post had at least one comment or “vote” by a different user. Criteria (d) was employed to identify shared or relatable experiences among mothers and weed out “spam” posts which users ignore. Exclusion criteria included posts from outside sources, repeat posts, and posts identified to be spam. Corresponding comments for each original post were also included if they met the same above criteria (with both referred to collectively below as “entries”).
Content analysis
Qualitative content analysis was performed based on steps outlined by Braun and Clarke. 17 First, entries were categorized into one or more of six predominant themes, based upon if the mother’s mental health symptoms were related to (1) breastfeeding in general, (2) difficulty breastfeeding, or (3) weaning from breastfeeding; if her symptoms were (a) new or (b) preexisting; and, if preexisting, if they were (i) improved or (ii) worsened by breastfeeding. A seventh theme was added for entries that discussed breastfeeding consequences of mental health symptoms (Fig. 1). Next, entries were organized into related sub-themes. Quantitative content analysis was also employed to examine the frequency of certain significant words repeated by different users. Chi-squared analysis was performed using a p-value of <0.05 to test for statistical significance.
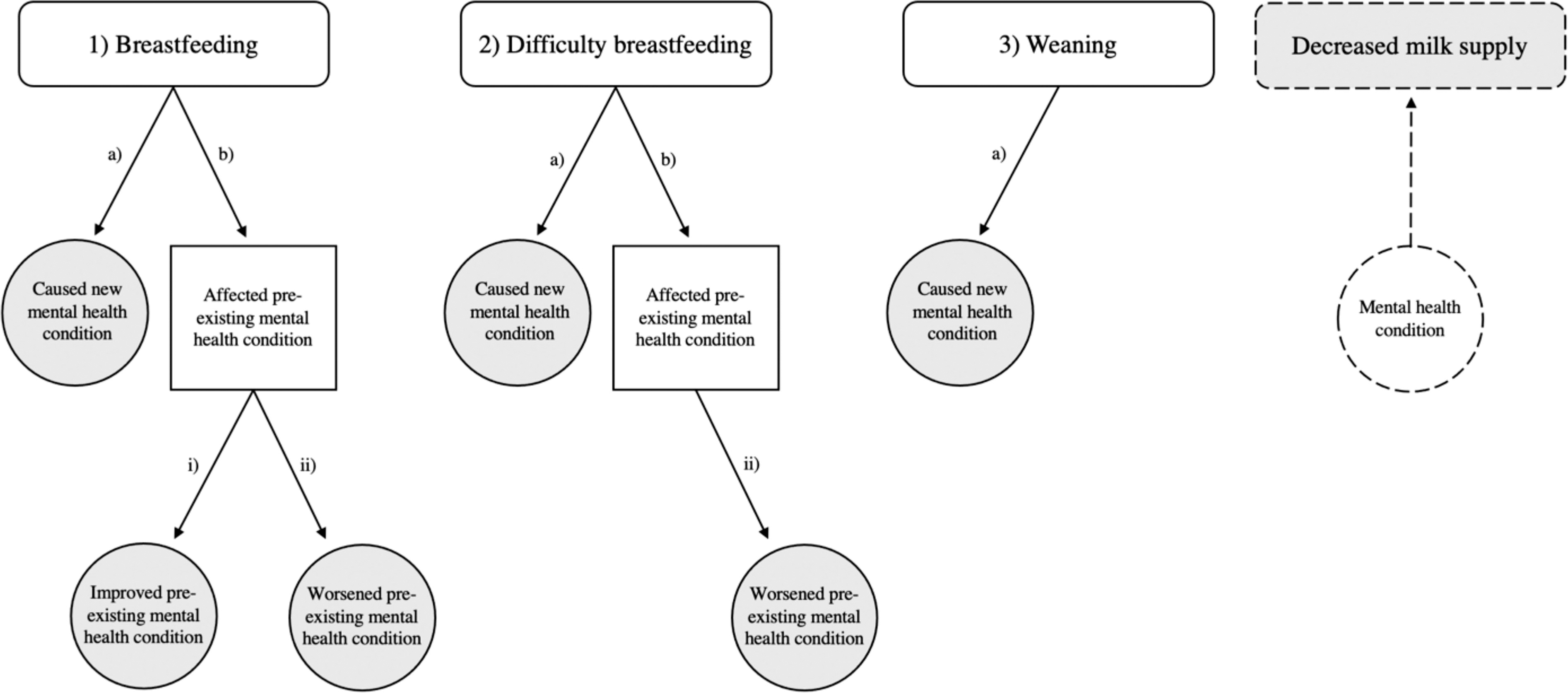
Thematic analysis workflow.
Results
Our search yielded a total of 584 evaluable entries after application of inclusion and exclusion criteria, of which 94 were original posts and 490 corresponding comments.
Maternal mental health conditions
Although our search terms were set to only look at how depression relates to breastfeeding, nearly half of all entries (n = 246) described another primary or comorbid mental health condition. Predominantly, this included an unspecified diagnosis (n = 135) or anxiety (n = 128). A smaller number of entries described a wide variety of other mental health diagnoses (Table 1).
Maternal Mental Health Conditions Associated with Breastfeeding Attempts
Data are presented as number (percentage).
ADHD, attention-deficit/hyperactivity disorder; DMER, dysphoric milk ejection reflex; OCD, obsessive-compulsive disorder; PMDD, premenstrual dysphoric disorder; PTSD, posttraumatic stress disorder.
Thematic analysis
Among all entries (n = 584), mothers most frequently described difficulty breastfeeding as the cause of new onset mental health symptoms (53%); however, mothers breastfeeding without difficulty were also susceptible (20%). Mothers also reported exacerbated preexisting mental health symptoms—more frequently related to difficulty breastfeeding (17%), but still others experienced no difficulty (6%). Other themes yielded from this study included weaning-induced mental health symptoms (17%) and decreased milk supply due to mental health symptoms (2%). Only 3% of all entries described breastfeeding as improving mental health symptoms (Fig. 2), though this outcome was limited by our search criteria.

Major themes describing relationship between breastfeeding and depression (or other mental health condition). Entries were categorized into one or more of seven major themes in order to characterize the relationship between breastfeeding and maternal mental health. The blue bar indicates the number of mothers who reported depressive symptoms. The gray bar indicates the number of mothers who reported other mental health symptoms. The proportion of total mothers describing each theme is indicated to the right of each combined bar.
Maternal impact
Difficulty breastfeeding and negative breastfeeding experiences had a profound impact on mothers. They described negative feelings about themselves as women and their aptitude as mothers. Among all entries, the most common feelings were guilt (17%) and failure (14%) (Fig. 3). Mothers stated:

Frequently used words by mothers. A word cloud was generated to highlight significant words repeated by mothers. The larger the text, the more frequently the word was used by mothers.
“I felt like it was my fault. That I failed.”
“I feel like a failure that I can’t provide for my baby.”
Mothers also described feelings of pressure (7%), shame (6%), and loneliness (6%). For some mothers (1%), these feelings stemmed from a perception that they could not feed their child in the “natural” way (Fig. 3). Mothers stated:
“All I wanted was to feed my son ‘the natural way’ after I couldn’t give birth to him ‘the natural way’ and I can’t even do that. I think often that my son would be better off without me in his life. I wonder why I ever thought I’d be a good mother. I just want this pain and stress to end.”
“I thought I was the worst parent in the world for giving up on breastfeeding after 3 months. I cried every night for a month and wondered why I had ever chosen to have kids.”
Negative maternal emotions (namely guilt, failure, pressure, shame, and loneliness) were used throughout this study as a marker of maternal psychological distress to draw associations between certain maternal characteristics and negative psychiatric outcomes related to breastfeeding. Consistent with current literature indicating prepartum and antepartum depression and anxiety as risk factors for PPD, mothers who reported a prior mental health diagnosis were more likely to describe feelings of failure than mothers who reported a new mental health diagnosis (p = 0.005). 18,19 Of note, mothers who reported past or current other mental symptoms (predominantly anxiety) were just as likely to experience negative emotions as mothers who reported past or current depression (Table 2).
Association Between Maternal Characteristics and Negative Emotions
Data are presented as number (percentage), unless otherwise indicated.
Excludes undefined mental health condition.
Indicates a significance of p < 0.05.
Stigma against formula
Among all entries, 32% (n = 186) described experiencing or feeling external stigma against formula feeding. There was a statistically significant relationship between external stigma against formula and feelings of guilt (p < 0.001), failure (p < 0.001), pressure (p = 0.01), and shame (p < 0.001) (Table 2).
Breastfeeding intention
Seventeen percent of all mothers (n = 100) reported intention to breastfeed versus formula feed and 7% of all mothers (n = 41) described having a preconceived negative idea themselves about formula feeding. Consistent with other studies linking unmet breastfeeding expectations to increased PPD, there was a statistically significant relationship between breastfeeding intention and feelings of guilt (p < 0.001), failure (p < 0.001), and loneliness (p = 0.002). 9,10,20,21 There was also a statistically significant relationship between negative preconceptions about formula and feelings of failure (p = 0.002) and pressure (p = 0.007) (Table 2). Mothers who reported a prior mental health diagnosis were no less likely to report breastfeeding intention than mothers who reported a new mental health diagnosis, contradicting ideas that depression may decrease mothers’ motivation to breastfeed. 9
Inadequate breastfeeding counseling
Nearly one quarter (23%) of all mothers (n = 584) reported inadequate breastfeeding counseling. Primarily, these mothers (n = 133) felt uninformed about potential negative breastfeeding outcomes, including weaning-induced mental health symptoms (36%) and dysphoric milk ejection reflex (DMER) (22%)—an acute onset episode of negative mood symptoms following milk let-down, suspected to be related to abrupt drops in dopamine. 22 Mothers also felt unprepared for how hard breastfeeding would be (23%) and were unaware that breastfeeding could affect their mental health (15%). Finally, 11% of mothers reported inadequate education on formula feeding and 8% inadequate counseling on postpartum mental health conditions. Mothers stated:
“They tell you all the benefits and crap, but not once did anyone tell me how hard it was gonna be mentally.”
“I think the slogan for the fourth trimester should be ‘Not As Advertised’. You hear all these wonderful stories about bonding, and cuddles, and a deeper love than you have ever felt before, and then left wondering if you are doing it wrong because you are having meltdowns, stressed, and everything seems like an uphill battle.”
Despite mothers’ frustrations about poor breastfeeding counseling, no significant relationship was found between inadequate breastfeeding counseling and maternal negative emotions (Table 2).
Experience with health care providers
Overall, 9% of all entries reported a negative experience with health care providers, versus 6% a positive experience. Negative experiences (n = 52) included pressure to breastfeed (71%), stigma against formula feeding (28%), silence about formula feeding (25%), and criticism for not breastfeeding (18%). One mother stated:
“They made me feel like a terrible, stupid human for not being able to figure out how to feed him the right way…They encouraged me by listing all the benefits from breastfeeding. Those benefits replay in my mind every time I think about going to formula - how could I deny my son those benefits, even if it causes physical and mental pain to me?”
Positive experiences (n = 34) included providers who didn’t judge formula use (36%), emphasized mental health over breastfeeding (30%), and encouraged formula (27%). Mothers offered encouragement and hope to each other by recalling specific helpful pieces of advice from their own providers (Table 3). One mother stated:
Advice from Health Care Providers that Mothers Found Helpful
Data are presented as number.
“The thing that I held onto was something my doctor said: ‘The best way to have a healthy baby is to have a healthy mom.’”
Surprisingly, experience with provider (negative versus positive) had no association with maternal negative emotions (Table 2). Where entries specified the category of provider, mothers listed predominantly negative experiences with “baby-friendly” hospitals (100% negative), lactation consultations (88% negative), midwives (82% negative), nurses (76% negative), and unspecified doctors (67% negative) (Fig. 4). One mother stated:
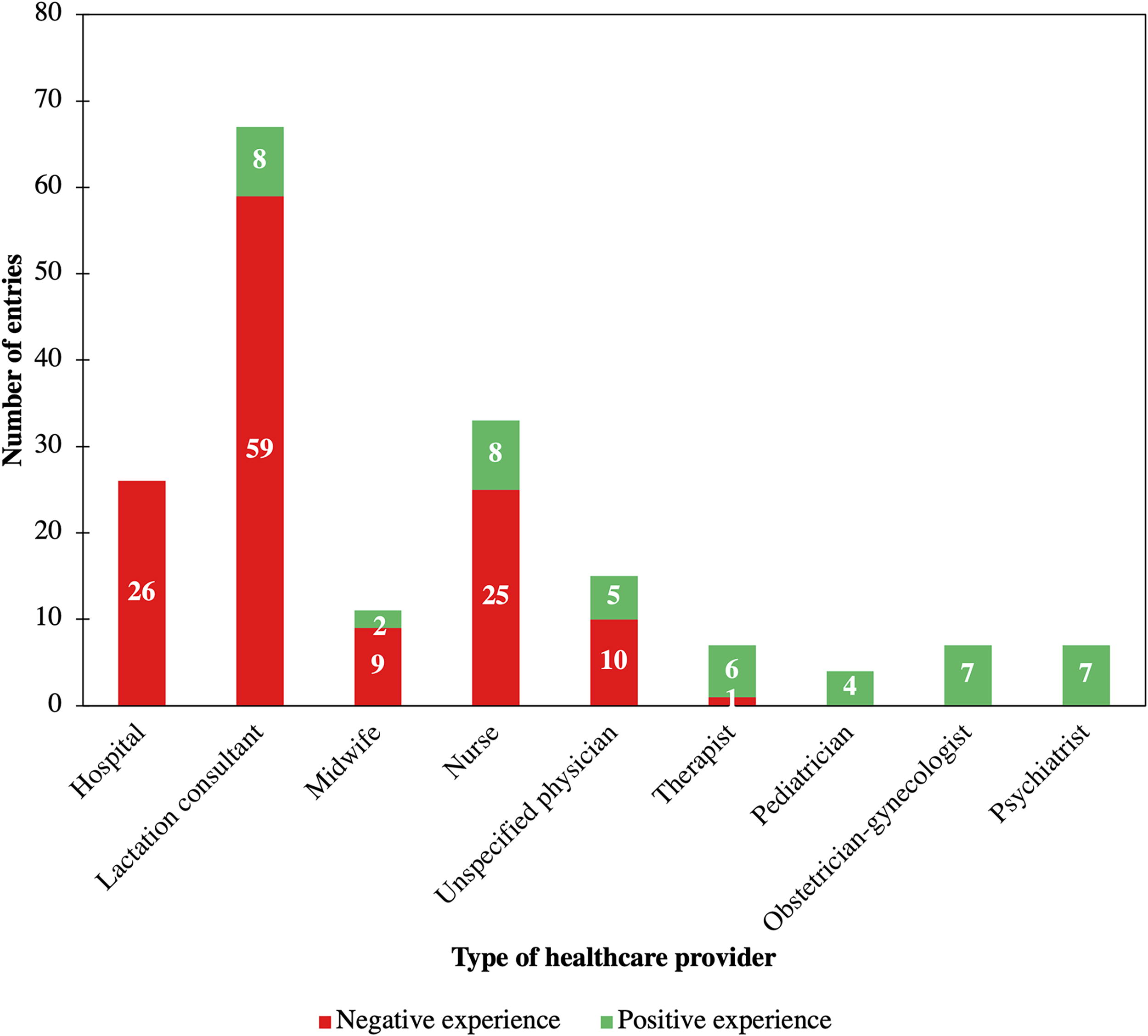
Maternal experiences with health care providers. We compared reported maternal experiences (either positive or negative) with different health care providers. The red bar indicates the number of mothers who reported a negative experience with each health care provider. The green bar indicates the number of mothers who reported a positive experience with each health care provider.
“I gave birth in a baby friendly hospital (gag, never again) and was horribly, horribly guilted and shamed into breastfeeding when I was struggling so so much. They made it seem like formula would cause my child to be permanently damaged…When I finally supplemented with formula, I felt like a failure of a mom. But that was just my disorder, my PPD speaking to me, it wasn’t real. My PPD went away almost immediately once I started supplementing with formula.”
Conversely, mothers listed predominantly positive experiences with psychiatrists (100% positive), obstetrician-gynecologists (100% positive), pediatricians (100% positive), and therapists (86% positive) (Fig. 4). One mother stated:
“At our first well-visit my daughter’s pediatrician (a guy) asked if I was breastfeeding. I shamefacedly said ‘No’ expecting yet another lecture, but he just nodded and said ‘Okay’ and moved on. I quite literally almost cried I was so grateful.”
Of note, while obstetrician–gynecologist experiences appeared overwhelmingly positive, some negative “unspecified physician” experiences (many of which occurred within hospitals in labor and delivery units) could likely be attributed to obstetrician–gynecologists.
Breastfeeding difficulty
The reasons for maternal breastfeeding difficulty (n = 361) were myriad. The most common cause of breastfeeding difficulty was low supply (40%), followed by poor latching (29%), an undefined problem (28%), and inadequate time (17%). A smaller number of entries described other causes of breastfeeding difficulty (Table 4).
Causes of Maternal Breastfeeding Difficulty
Data are presented as number (percentage).
Compared to mothers experiencing no difficulty, mothers who reported breastfeeding difficulty were more likely to describe feelings of failure (p < 0.001) and guilt (p = 0.005) (Table 2). This is consistent with recent evidence linking breastfeeding challenges to increased mental health symptoms. 21 Mothers who breastfed without difficulty, yet still experienced mental health symptoms secondary to breastfeeding, were more likely to feel lonely than mothers whose symptoms were related to difficulty breastfeeding (p = 0.03) (Table 2).
Despite previous studies indicating depression as a risk factor for early breastfeeding cessation and decreased breastfeeding self-efficacy, mothers who reported a prior mental health diagnosis or depressive symptoms were no more likely to report breastfeeding difficulty than mothers who reported a new mental health diagnosis or other mental health symptoms, respectively. 9,19,23,24 Experience with provider (either positive or negative) also had no association with breastfeeding ability (Table 5).
Association Between Maternal Characteristics and Breastfeeding Ability
Data are presented as number (percentage), unless otherwise indicated.
Excludes undefined mental health condition.
Maternal–Infant bonding
Maternal–infant bonding was described in 17% of all entries. Among all entries mentioning bonding (n = 99), 58% reported that breastfeeding inhibited infant bonding versus only 1% enhanced bonding (Fig. 5). One mother stated:
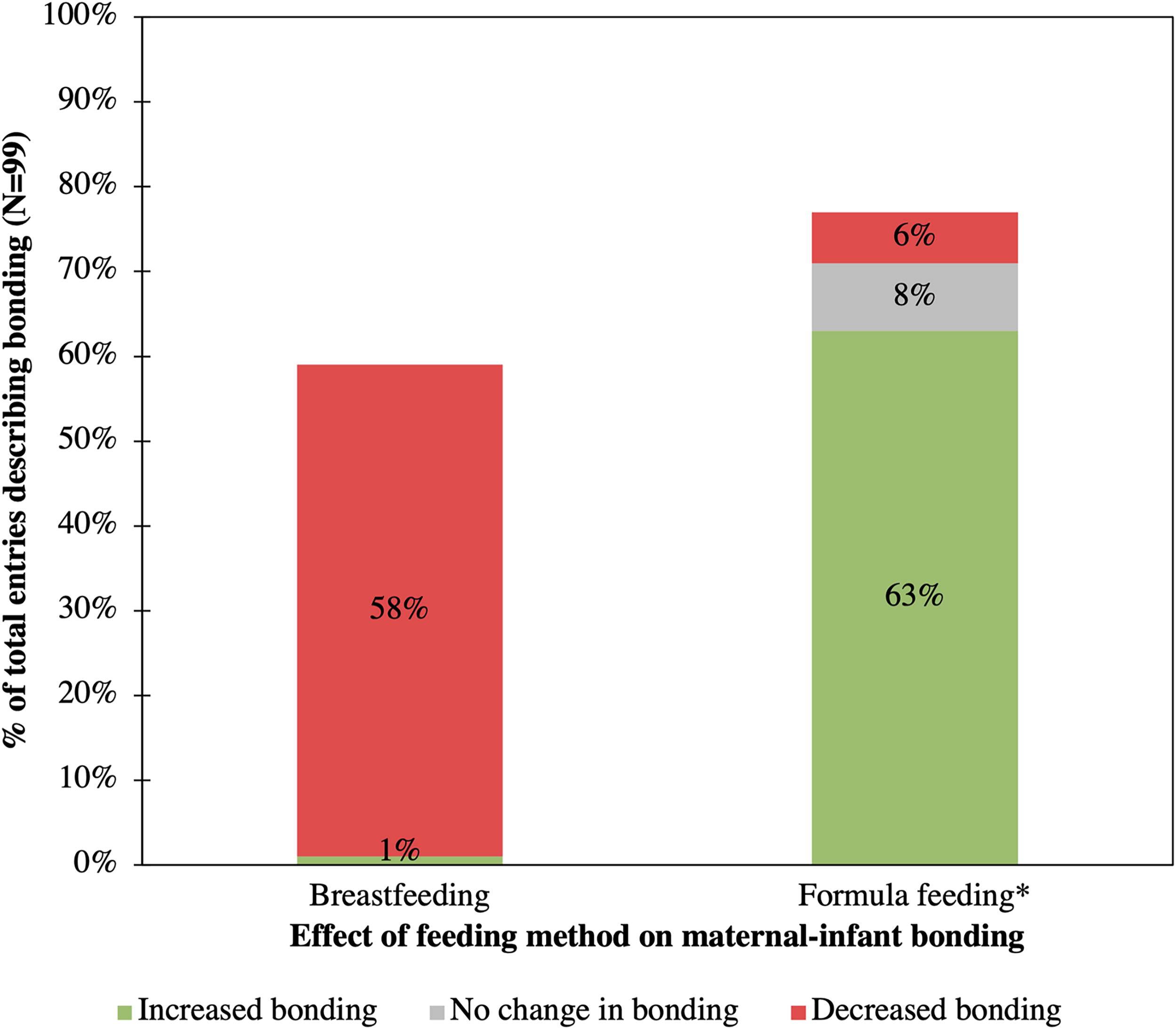
Impact of feeding method on maternal–infant bonding. We compared reported maternal–infant bonding experiences between mothers’ breastfeeding versus formula feeding. The red bar indicates the proportion of mothers whose maternal–infant bonding experiences were inhibited by breastfeeding compared to formula feeding. The green bar indicates the proportion of mothers whose maternal–infant bonding experiences were enhanced by breastfeeding compared to formula feeding. *Indicates after switching from breastfeeding.
“I’m starting to wonder if this is not more damaging to my mental health and to bonding with my son.”
Furthermore, of these 99 entries, 63% reported increased bonding after switching to formula, 8% no change in bonding, and 6% decreased bonding (Fig. 5). Switching to formula had a significant positive impact on the mental health of mothers who faced challenges breastfeeding.
Mothers stated:
“I couldn’t bond with my baby until I stopped breastfeeding.”
“The day I decided to quit pumping and nursing was the day that saved my life.”
Mothers who reported a prior mental health diagnosis, depressive symptoms, or breastfeeding difficulty were no more likely to experience poor bonding associated with breastfeeding than mothers who reported a new mental health diagnosis, other mental health symptoms, or lack of breastfeeding difficulty, respectively. However, investigation of these associations was limited by small sample size (Table 6).
Association Between Maternal Characteristics and Maternal–Infant Bonding
Data are presented as number (percentage), unless otherwise indicated.
Includes bonding inhibited by breastfeeding and/or increased after switching to formula.
Includes bonding enhanced by breastfeeding and/or decreased after switching to formula.
Excludes undefined mental health condition.
Discussion
Principal findings
This study validated the existence of an important subset of women who does not experience the classically described benefits of breastfeeding, instead exhibiting increased depressive and other negative mental health symptoms. Additionally, among this group of women, we noted a high prevalence of maternal–infant bonding difficulties.
Consistent with newer literature, we found that breastfeeding difficulty increases depressive symptomatology. 9 However, depressive symptoms were also reported by those who did not report any breastfeeding challenges, contradicting prior evidence suggesting it is only mothers having difficulty with or unmet expectations regarding breastfeeding in which breastfeeding leads to depression. 21 Furthermore, there may be several other mental health conditions to monitor for in addition to depression—namely, anxiety, PTSD, and DMER. For mothers with negative breastfeeding experiences, bonding was worsened by breastfeeding and improved by switching to formula—raising concern about the generalizability of the notion that breastfeeding stimulates bonding.
This study revealed possible biases in current breastfeeding education and comprehensive information delivery. Mothers reported that health care providers overemphasized well-known benefits of breastfeeding at the expense of information about potential breastfeeding challenges, and alternatives to breastfeeding if such obstacles should arise, leading mothers to feel unprepared for the postpartum period and mistrusting of the health care system. Mothers felt alone in their hardships, thus exacerbating, and in some cases inciting, mental health symptoms. Going forward, we must strike a balance between breastfeeding encouragement and acceptance of other feeding methods in cases where breastfeeding may cause more harm to the mother. Particularly, when caring for new mothers struggling with breastfeeding-related mental health symptoms, cessation of breastfeeding and introduction of formula may serve to repair damaged bonding relationships between mother and baby and improve mothers’ overall mental health. It is also important that we are able to screen for mothers who may be at increased risk for adverse mental health outcomes, using markers and risk factors identified in this study such as preexisting mental health diagnoses, plans to breastfeed, negative preconceptions about formula, or difficulty breastfeeding.
This study highlights the value of using social media to explore highly sensitive health topics. Although patients may be hesitant to volunteer information about their mental health struggles to providers, on Reddit they opened up. Consequently, we were able to gain vital insight about a previously overlooked population that does not benefit in traditional ways from breastfeeding.
Strengths and limitations
These findings are subject to certain limitations. First, maternal mental health diagnoses were based on either self-report or categorization by authors according to symptoms, and thus cannot be verified. Second, the timeframe from postpartum experience to entry varied from days to years later—introducing recall bias. Finally, it is prudent to recognize limitations in the generalizability of qualitative research. The entries of mothers satisfied with their breastfeeding experiences or reporting positive or neutral mental health outcomes would likely not be captured by the combined search terms “breastfeeding” and “depression,” leading to sampling bias and an overrepresentation of mothers with negative experiences and outcomes. It is of note that over eight years, only 94 original posts were recovered using our search criteria, which is encouraging to the authors that the overall proportion of breastfeeding mothers who experience breastfeeding-related depression, or depression in general, is low (though could also reflect fears of stigma). Furthermore, different social media sites may attract mothers with varying breastfeeding “success” rates and demographic risk factors for developing peripartum mental health conditions, and thus our data may not be representative of other platforms or social media as a whole. That being said, the aim of this study was not to dispute established benefits of breastfeeding or draw conclusions about the proportion of mothers whose mental health is negatively impacted by breastfeeding, only to draw attention to a group who is severely struggling and needs additional support.
A major strength of our study was the anonymity inherent in social media sites like Reddit. Women noted that compared to other sites, on Reddit they felt less judged for their decision to not breastfeed, or “failure” to do so. Additionally, individual manual analysis of entries allowed us to integrate context, tone, and implied or nuanced meaning of entries to draw more meaningful inferences from our data. Finally, we were able to analyze every entry that our search terms identified on Reddit (without limiting our retrospective time frame), making our data completely comprehensive and more generalizable. To our knowledge, this is the first study of its kind to examine the relationship between breastfeeding and depression using a social media content analysis.
Conclusions
Breastfeeding difficulty and negative breastfeeding experiences appear to incite and/or enhance PPD and other mental health conditions and impair maternal–infant bonding. Based on our findings, it is likely that damaging societal breastfeeding expectations underlie this relationship. Unfortunately, women facing these struggles report overwhelmingly negative experiences with their health care providers who reinforce internal feelings of failure. It is our responsibility as health care providers to include maternal mental health as a top priority when counseling women about breastfeeding, especially when other sources of nutrition are available to the infant.
Footnotes
Authors’ Contributions
E.A.W.: Conceptualization; Methodology; Formal Analysis; Investigation; Resources; Data Curation; Writing—Original Draft; Writing—Review and Editing; Visualization. A.M.: Conceptualization; Methodology; Writing—Review and Editing. A.L.N.: Conceptualization; Methodology; Resources; Writing—Review and Editing; Supervision.
Author Disclosure Statement
The authors report no conflict of interest.
Funding Information
The authors report no funding for this study.