
Abstract
Objective:
To describe the rate, timing, and primary diagnosis codes for emergency care visits up to 8 weeks (56 days) after live birth among Medicaid beneficiaries in North Carolina (NC).
Materials and Methods:
Using a linked dataset of Medicaid hospital claims and certificates of live birth, which included Medicaid beneficiaries who had a live-born infant in NC between January 1, 2013, and November 4, 2019, and met inclusion criteria (n = 321,879), we estimated week-specific visit rates for emergency care visits that did not result in hospital admission (outpatient) and those that did (inpatient). We assessed the 10 leading diagnosis code categories for emergency care visits and described the characteristics of people with 0, 1, or ≥2 outpatient emergency care visits.
Results:
One in eight (12.4%) Medicaid beneficiaries had an emergency care visit that did not result in inpatient hospital admission during the first 8 weeks postpartum. Visit rates peaked in postpartum week 2. Diagnosis codes for nonspecific symptoms and substance use were the two leading diagnosis code categories for outpatient emergency care visits. Respiratory concerns and gastrointestinal concerns were the two leading diagnosis code categories for inpatient emergency care visits. Compared with those with zero outpatient emergency care visits, a greater proportion of people with ≥2 visits had less than a high school education, used tobacco during pregnancy, had Medicaid insurance outside of pregnancy, had mental health as a medical comorbidity, and/or had ≥2 medical comorbidities.
Conclusions:
These findings support scheduling health care visits early in the postpartum period, when emergency care visits are most frequent, and point to unmet needs for substance use support.
Introduction
Postpartum emergency care visits may indicate barriers to usual sources of care or that birthing people’s health needs are not being adequately addressed by routine postpartum health services. 1,2 Medicaid is the most frequent payor for maternal and neonatal emergency department (ED) visits, and Medicaid beneficiaries frequently access care through the ED 3,4 ; however, little is known about their patterns of emergency care use in the postpartum period. The postpartum period is a vulnerable time for birthing people, with two-thirds of pregnancy-related deaths occurring 1 day to 1 year postpartum. 5
In North Carolina (NC), nearly half of all births are funded by Medicaid. 6 Generating a better understanding of emergency care use patterns among NC Medicaid beneficiaries in the postpartum period may identify opportunities for improving perinatal systems of care for this population. To guide improvement, we describe the rate timing and primary diagnosis codes for emergency care visits up to 8 weeks (56 days) after live birth among Medicaid beneficiaries in NC.
Materials and Methods
This study was reviewed and approved by the University of North Carolina Office of Human Research Ethics (IRB #20–0640).
Data sources and study population
We constructed a retrospective cohort of pregnant Medicaid beneficiaries in NC using a linked dataset of Medicaid claims and certificates of live birth available from the Community Care of North Carolina. Infant birth certificates were deterministically linked to the mother’s Medicaid claims using a multiple-step strategy using the following match fields: mother’s first and last name, mother’s date of birth, date of infant birth, and county of occurrence. Records were matched sequentially first requiring an exact match on all identifiers and then using a combination of deterministic and probabilistic match criteria for each successive round. The maternal record linkage had a match rate of 95%.
Using the linked data, the Community Care of North Carolina provided an analytic dataset that included hospital claims and infant birth certificates for 380,307 Medicaid beneficiaries without emergency Medicaid who had a live-born infant in NC between January 1, 2013, and November 4, 2019. We identified an additional 76 individuals with emergency Medicaid in the analytic dataset and excluded them from the analysis. We excluded those with emergency Medicaid during the birth hospitalization as they did not have complete Medicaid coverage outside of birth (e.g., for outpatient visits), and we would not be able to capture hospital visits from Medicaid claims during this time. Because many people during this time period lost Medicaid coverage around 60 days postpartum, we also excluded individuals missing data on the months of Medicaid coverage (n = 16,394) and those without Medicaid coverage for at least 8 weeks (56 days) postpartum (n = 26,952) to ensure that we could observe each cohort member for 8 weeks postpartum and capture hospital visits in the Medicaid claims during that time. We also excluded individuals without a birth hospitalization claim (n = 15,006) as information from this claim was necessary for our analyses, including the identification of severe maternal morbidity (SMM). A total of 321,879 postpartum people were included in this analysis.
Measures
Emergency care visit
To identify emergency care visits in our linked dataset, we assessed revenue codes and included those for an unscheduled encounter in the ED (revenue codes 450, 451, 452, 456, and 459) or Obstetric Triage unit (revenue codes 720 and 729) that either resulted in inpatient hospital admission (“inpatient”) or an outpatient visit that did not result in inpatient hospital admission (“outpatient”). Outpatient visits and inpatient visits are exclusive and sum to the total emergency care visits. We used the infant date of birth, as reported on the certificate of live birth, to estimate when the visits occurred postpartum because the dataset did not contain the date of discharge from the birth hospitalization. Emergency care visits were counted through December 31, 2019 to capture visits in the 8 weeks (56 days) postpartum for those who had a live-born infant up to November 4, 2019.
Maternal sociodemographic and pregnancy characteristics
All maternal sociodemographic (age at birth, race and Hispanic ethnicity, education, and area of residence) and pregnancy (prenatal tobacco use, parity [defined as the total number of live births prior to the index birth], multifetal gestation, and trimester of prenatal care initiation) characteristics were obtained from certificates of live birth with the exception of Medicaid type and medical comorbidities at birth hospitalization, which came from Medicaid claims. Using residential county, area of residence was categorized as rural or urban according to the NC Rural Center’s county designation based on population density, with rural counties including those with fewer than 250 persons per square mile. 7 Medical comorbidities were identified from secondary or higher diagnosis codes (up to nine were reported) that were included on the birth hospitalization claim. There were 12 medical comorbidities that were of interest for this analysis, including anemia, asthma, cardiac disease, chronic hypertension, diabetes, HIV, lupus, mental health, obesity, renal disease, seizure disorder, and sickle cell disease. Consistent with federal definitions and reporting, SMM during the birth hospitalization, excluding blood transfusion, was defined using International Classification of Diseases (ICD) diagnosis and procedure codes for 20 indicators in the birth hospitalization claim. 8
Diagnosis codes
The primary ICD-9 and ICD-10 diagnoses codes were abstracted for each emergency care visit and grouped by organ system. Since the transition from ICD-9 to ICD-10 occurred on October 1, 2015, we used ICD-9 diagnosis codes through September 2015 and ICD-10 diagnosis codes from October 2015 through the end of the study period. Nonspecific codes without an indication of organ system were grouped as diagnosis codes for nonspecific symptoms (e.g., nausea, vomiting, unspecified pain, malaise and fatigue, and syncope and collapse) or miscellaneous (e.g., abnormal findings in body fluids, substances, or in specimens, complications of procedures, and encounter for examination and observation), as appropriate. Additional codes without a clear delineation of an organ system included social determinants of health, substance use, and poisoning/adverse effect of medication. All injuries and burns, regardless of location on the body, were classified as injuries. We categorized the diagnosis codes that appeared in the dataset and present these categories and accompanying codes in the Supplementary Appendix Table S1.
Statistical analysis
We estimated week-specific emergency care visit rates (visits per week per 100 people) for outpatient and inpatient visits. These rates were estimated overall and by maternal sociodemographic, pregnancy, and birth characteristics. The 10 leading diagnosis code categories for emergency care visits were assessed overall and by week of visit for both outpatient and inpatient visits. We also assessed the sociodemographic and pregnancy characteristics of people with zero, one, or two or more emergency care visits that did not result in admission. Because these visits did not result in admission, they may not signal a true health care emergency and may indicate that the postpartum person has difficulties accessing consistent and adequate health care. 9
Results
Maternal characteristics and emergency care visits
This cohort included 321,879 postpartum people whose sociodemographic, pregnancy, and birth characteristics are described in Table 1. There were 50,796 outpatient emergency care visits and 5,834 inpatient emergency care visits within 8 weeks postpartum. Outpatient visit rates were highest among postpartum people who experienced SMM during the birth hospitalization, had one or more medical comorbidities, used tobacco during pregnancy, and/or had less than a high school education. Outpatient emergency care visit rates did not vary meaningfully by race/ethnicity or urban versus rural residence. Rates of emergency care visits resulting in admission were higher for people with SMM compared with those without but did not vary considerably by sociodemographic characteristics, pregnancy characteristics, or medical comorbidities (Table 1).
Characteristics of North Carolina Medicaid Beneficiaries Who Had a Live-Born Infant and Postpartum Emergency Care Visit Rates a for the Time Period Following Birth and up to 56 Days After Birth, 2013–2019
Emergency care visits defined according to revenue codes: 450, 451, 452, 456, 459, 720, and 729.
Defined as emergency care visits that do not result in hospital admission.
Defined as emergency care visits that result in hospital admission.
Categorized as rural or urban according to the North Carolina Rural Center’s county designation based on population density with rural counties including those with fewer than 250 persons per square mile (ncruralcenter.org).
Categories are not mutually exclusive.
Defined using International Classification of Diseases diagnosis and procedure codes for 20 indicators in the birth hospitalization claim (https://www.cdc.gov/reproductivehealth/maternalinfanthealth/smm/severe-morbidity-ICD.htm).
The highest rates of both outpatient and inpatient emergency care visits occurred in postpartum week 2 (Fig. 1).
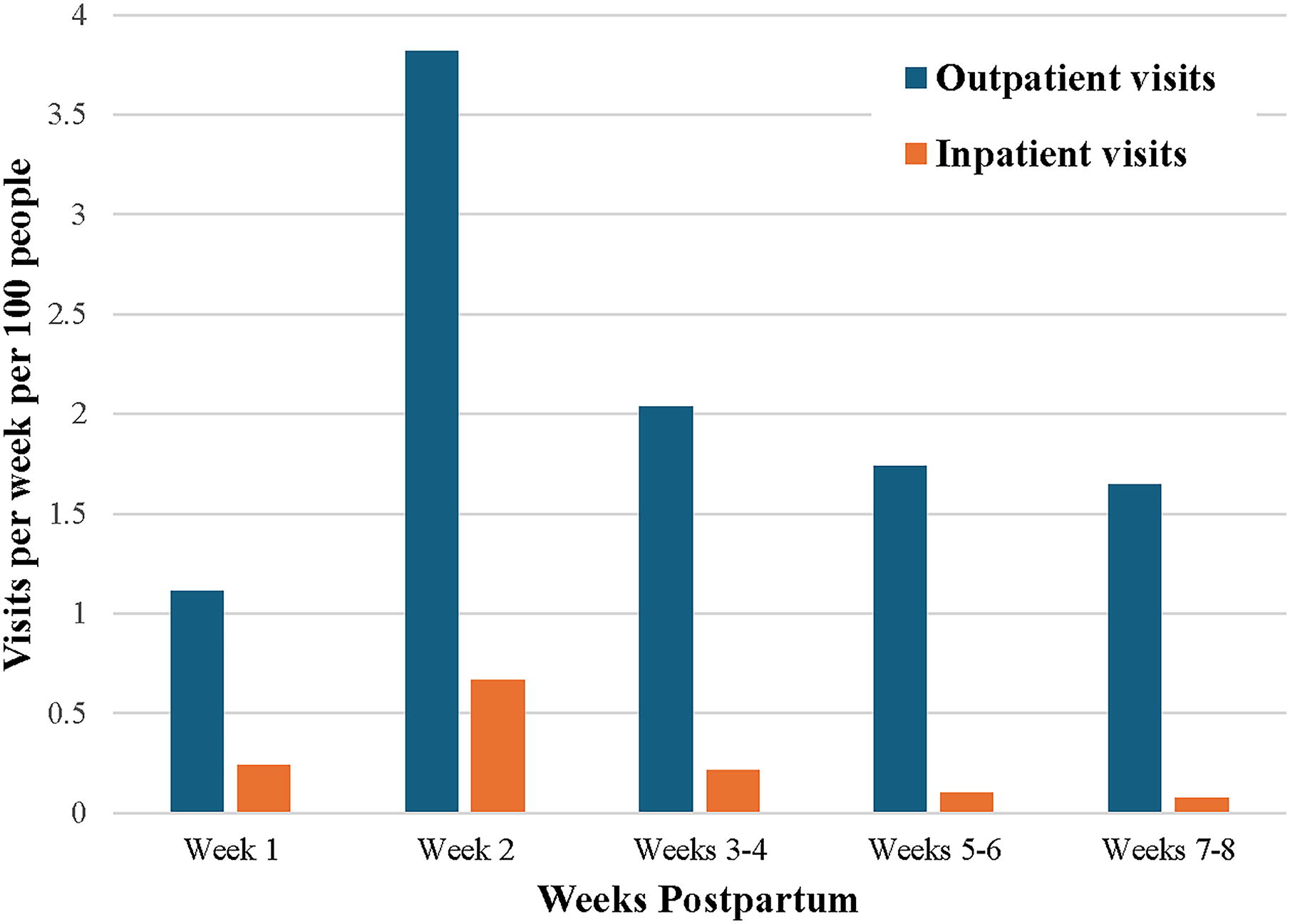
Postpartum emergency care visit rates among North Carolina Medicaid beneficiaries who had a live-born infant between 2013 and 2019. Outpatient visits were defined as emergency care encounters in the emergency department or Obstetric Triage unit that did not result in inpatient admission. Inpatient visits were defined as emergency care encounters in the emergency department or Obstetric Triage unit that did result in inpatient admission.
Diagnosis codes associated with emergency care visits
Diagnosis codes for nonspecific symptoms and substance use were the first and second leading categories for outpatient emergency care visits, respectively (Table 2). Diagnosis codes for nonspecific symptoms was the leading outpatient category through weeks 3–4 postpartum, and substance use was the leading category for weeks 5–6 and 7–8 postpartum.
Ten Leading Diagnosis Code Categories for Postpartum Emergency Care Visits a That Did Not Result in Admission Following Birth and up to 56 Days After Birth, Overall and by Postpartum Week, Among North Carolina Medicaid Beneficiaries Who Had a Live-born Infant, 2013–2019
Diagnosis codes for nonspecific symptoms included primary diagnosis codes for nausea, vomiting, abdominal pain, chest pain, chronic pain, unspecified pain, malaise and fatigue, syncope and collapse, symptoms and signs concerning food and fluid intake, symptoms and signs involving appearance and behavior, insomnia, weakness, and shortness of breath.
Substance use includes primary diagnosis codes for indications such as findings of drugs and other substances, alcohol-related disorders, and opioid-related disorders.
Miscellaneous includes primary diagnosis codes for nonspecific, nonsymptom indications, such as abnormal findings in body fluids, substances, or specimens, complications of procedures, and encounter for examination and observation.
Pregnancy complications include primary diagnosis codes for indications such as ectopic pregnancy, placenta previa, and premature rupture of membranes.
For inpatient emergency care visits, the leading category overall was respiratory and gastrointestinal concerns (Table 3). Pregnant state was the leading inpatient visit category in week 1 postpartum, respiratory concerns was the leading category in week 2 postpartum, and gastrointestinal concerns was the leading category in weeks 3–4, 5–6, and 7–8 postpartum.
Ten Leading Diagnosis Code Categories for Postpartum Emergency Care Visits a Resulting in Admission Following Birth and up to 56 Days After Birth, Overall and by Postpartum Week, Among North Carolina Medicaid Beneficiaries Who Had a Live-born Infant, 2013–2019
Miscellaneous includes primary diagnosis codes for nonspecific, nonsymptom indications, such as abnormal findings in body fluids, substances, or specimens, complications of procedures, and encounter for examination and observation.
Substance use includes primary diagnosis codes for indications such as findings of drugs and other substances, alcohol-related disorders, and opioid-related disorders.
Pregnancy complications include primary diagnosis codes for indications such as ectopic pregnancy, placenta previa, and premature rupture of membranes.
Labor and delivery complications include primary diagnosis codes for indications such as failed induction of labor, labor and delivery complicated by umbilical cord complications, and perineal laceration during delivery.
Maternal and pregnancy characteristics by number of outpatient emergency care visits
In this cohort, 32,433 postpartum people (10.1%) had an outpatient emergency care visit once, and 7,563 people (2.3%) had an outpatient emergency care visit two or more times within 8 weeks postpartum, totaling 12.4% of postpartum people with at least one outpatient emergency care visit (Table 4). Compared with people with zero outpatient emergency care visits, a higher proportion of people with two or more emergency care visits had less than a high school education (29.6% versus 18.6%), used tobacco during pregnancy (27.3% versus 16.2%), had Medicaid insurance outside of pregnancy (59.1% versus 44.0%), had mental health as a medical comorbidity (8.4% versus 4.1%), and/or had two or more medical comorbidities (12.9% versus 6.8%). A greater proportion of people with zero outpatient emergency care visits were college graduates as compared with those with two or more visits (7.8% versus 3.1%).
Characteristics of Medicaid Beneficiaries Who Had a Live-Born Infant by Frequency of Outpatient Emergency Care Visits a Following Birth and up to 56 Days After Birth, North Carolina, 2013–2019
Emergency care visits defined according to revenue codes: 450, 451, 452, 456, 459, 720, and 729.
Defined as emergency care visits that do not result in hospital admission.
Categorized as rural or urban according to the North Carolina Rural Center’s county designation based on population density with rural counties including those with fewer than 250 persons per square mile (ncruralcenter.org).
Categories are not mutually exclusive.
Discussion
In the first 8 weeks postpartum, emergency care visits were common. Emergency care visit rates peaked in postpartum week 2. Diagnosis codes for nonspecific symptoms was the leading diagnosis code category for postpartum emergency care visits that did not result in admission, followed by substance use. For postpartum emergency care visits resulting in inpatient admission, respiratory concerns was the leading diagnosis code category, followed by gastrointestinal concerns.
In this cohort of Medicaid beneficiaries in NC, 12% had an outpatient emergency care visit in the first 8 weeks after birth. This is consistent with a study among births to Maryland Medicaid beneficiaries in which 12% of birthing people had one or more emergency room visits within 8 weeks of birth. 10 Other studies in this literature vary in the length of the postpartum follow-up period, limiting direct comparison of emergency care utilization patterns. In a study of Medicaid beneficiaries authors reported that 35% of mothers had an ED visit within 6 months after birth. 11 Authors of a study using commercial and Medicaid insurance claims in Maryland reported that nearly half of Medicaid beneficiaries utilized the emergency room in the 12 months after birth. 12 An all-payer claims analysis in Maine reported that 44% of people had at least one ED visit in the 24 months after birth. 13
Our results are specific to Medicaid beneficiaries, whose utilization of health care is distinct from other payor groups. A representative survey of postpartum people in six states from January 2021 to March 2022 found that, compared with respondents who had commercial insurance at the time of birth, Medicaid beneficiaries were less likely to have a usual source of care and reported less primary, specialty, and dental care use in the first year after birth. 14 Furthermore, Medicaid is the most frequent payor for maternal and neonatal ED visits. 3 Studies of postpartum emergency care use in different payor groups generally report lower ED utilization than we found: in an all-payor study of ED use at a tertiary care women’s hospital, 5% of women had at least one ED visit within 42 days after birth, and an analysis of births in the Hospital Corporation of America found that 4.2% of women had one or more ED visits in the 42 days after hospital discharge after birth. 15,16 Analyses of postpartum emergency care use in special populations, including people with medically complicated pregnancies and people with mental health conditions, also report high postpartum emergency care utilization. 10,12,17 Among people who gave birth in Maine from 2007 to 2019, ED visits and hospitalizations in the first 2 years after birth were more frequent among women with prenatal depression, hypertensive disorders of pregnancy, and gestational diabetes compared with people without these conditions. 13
In this NC Medicaid population, the highest emergency care visit rates occurred in postpartum week two, which is consistent with the results of other published studies. A study of Medicaid beneficiaries at a regional perinatal center in the Mid-Atlantic reported that, in postpartum week two, the highest number of women had a first ED visit and the highest number of women had a first hospitalization. 11 A multistate analysis of readmissions within the State Inpatient Databases found that ∼90% of all-cause readmissions occurred within the first 30 days and that by day 15, nearly all hypertension, psychiatric disease, and wound infection or breakdown readmissions had occurred. 18 Using data from the Hospital Corporation of America, another study reported that outpatient and inpatient visits peaked in the first week after discharge from the birth hospitalization. 16
We found that substance use was the second most frequent diagnosis code category overall and the leading diagnosis code category in weeks 5–6 and 7–8 for outpatient emergency care visits. One national longitudinal study found that ED utilization for substance use disorder during pregnancy and postpartum that did not result in hospital admission increased substantially from 2006 to 2016 and that Medicaid beneficiaries accounted for a larger proportion of ED visits for substance use disorder compared with other payor groups. 19
In this analysis, respiratory and gastrointestinal concerns were the first and second leading diagnosis code category for emergency care visits resulting in admission in the first 8 weeks after birth. Similarly, gastrointestinal was the leading primary diagnosis for postpartum hospital readmission after a postpartum ED visit within 60 days of birth in a study of 2007–2012 births in California. 20 As expected, the 10 leading diagnosis code categories for emergency care visits resulting in admission more closely reflect the leading causes of pregnancy-related deaths, including mental health conditions and cardiac/coronary conditions, compared with those not resulting in admission. 5
The clinical implications of this study are significant for both the health care system and this patient population. First, emergency care use is frequent in the postpartum period, with the majority of care not resulting in inpatient admission. Outpatient visits were higher among people who were both medically and socially complex, yet inpatient visits only varied by SMM during birth; while inpatient visits indicate acuity, outpatient visits may reflect difficulties accessing timely and effective care in addition to acuity. Utilization of emergency rooms or triage units could compromise the perinatal health care Medicaid beneficiaries receive as they are not seen by their primary providers or clinicians with obstetric expertise and may lose the benefits of care continuity in the postpartum period. Second, the leading diagnosis code categories for emergency care visits may reflect important clinical features as well as emerging concerns for postpartum people. In this analysis, after diagnosis codes for nonspecific symptoms, the most common diagnosis code category for emergency care visits that did not result in inpatient admission was substance use. Mortality due to substance use in pregnant and postpartum persons has increased steadily since 2007. 21 Alongside this national trend, our findings suggest that postpartum people may face complex clinical and social issues, such as substance use disorders, and may benefit from systems that are designed to provide comprehensive clinical care and wraparound services—services that emergency care might not be equipped to provide. Third, the highest rate of emergency care utilization was in the second week postpartum, suggesting that older models of postpartum care, in which individuals are seen ∼4–6 weeks after birth, are insufficient. These findings underscore the importance of recent guidance from the American College of Obstetricians and Gynecologists recommending contact with a maternal care provider within 3 weeks of birth and follow-up with ongoing care as needed. 22 This work can also inform state-specific population health programs such as NC’s Pregnancy Medical Home program. 23
These and other findings on postpartum emergency care utilization help to identify areas in which the postpartum health care system might better meet patient needs. Translating this evidence into targeted improvements in health care systems should be the focus of future research, informed by qualitative studies and community-engaged research. 24 Research and implementation efforts should focus on special populations with overlapping risk factors for postpartum emergency care utilization, including Medicaid beneficiaries with substance use disorders, mental health conditions, and those with medically complicated pregnancies. Future research could explore how having access to a usual source of care impacts postpartum emergency care utilization and how extension of Medicaid coverage beyond the early postpartum period impacts postpartum health care utilization, including emergency care utilization and visits for routine postpartum care. 25
This population-based study includes all NC Medicaid beneficiaries who delivered a live-born infant over a period of 6 years, which is a large sample. The linked dataset used in this analysis allowed us to examine emergency care utilization patterns by sociodemographic and pregnancy characteristics, timing, and primary diagnosis codes, which would not be possible using certificates of live birth or claims data alone. This analysis uses the infant birth date from the certificates of live birth, which is more reliable than obtaining it from claims data. This is especially important because timing is a critical component of this study, and infant birth date was the starting time point for capturing postpartum emergency care visits. The use of claims data allowed for the inclusion of OB Triage visits, which were a frequent source of emergency care in the early postpartum period in our study population that may have otherwise been missed.
Though this study is population based, it includes only Medicaid beneficiaries, whose emergency care use patterns likely differ from those with private insurance and those who are uninsured. Further, the analysis includes only hospital-based emergency care visits, so visits to nonhospital-based emergency care locations (e.g., minute clinics and urgent care centers) are unobserved. Because of this, we may underestimate the use of unscheduled services. Also, our findings regarding primary diagnosis codes for hospital-based visits might not apply to nonhospital-based care. This cohort only included people who had a live birth and did not include those who had a fetal death, which limits our ability to describe postpartum visits for all pregnancies regardless of the outcome. Medicaid claims are used for insurance billing and rely on coding practices, which may vary by setting and portray inaccuracies and inconsistencies due to missed diagnoses and coding errors. For example, 119 postpartum emergency care visits resulting in inpatient admission had a primary diagnosis code of “pregnant state.” Because of these limitations, we may misrepresent the true reason for emergency care visits and likely underestimate the proportion of women who have the selected maternal comorbidities. Results related to diagnosis code categories and medical comorbidities may be affected by these factors. In addition, the transition from ICD-9 to ICD-10 occurred during the study period, which could impact our findings related to primary diagnosis codes for emergency care visits, as well as comorbidities and SMM. We did not have information on patient acuity, and there is no clear or systematic approach to determining the urgency or necessity of these emergency care visits using this claims dataset, which could direct system-level efforts to prevent emergency care visits for health concerns that would be best addressed in other clinical settings. We did not have information on discharge date, so we were unable to account for days when birthing people were staying in the hospital postpartum at which time they would not be at risk for postpartum emergency health care use. In particular, we expect that this limitation reduced the emergency care visit rates reported in week one postpartum.
Conclusions
In this study of emergency care use among Medicaid beneficiaries in NC, emergency care visits were common, yet most did not result in inpatient admission. Emergency care visit rates were highest in the second week postpartum, suggesting the need for postpartum care during this time. Moreover, leading diagnosis code categories associated with emergency care utilization, such as substance use, alongside characteristics of postpartum people with the highest emergency care visit rates, such as tobacco use during pregnancy or the occurrence of SMM, suggest that health care systems ought to better address clinical and social complexities to care for postpartum health needs early, potentially preventing emergency care utilization and improving maternal health outcomes. As such, findings from this study may help identify opportunities for improving perinatal systems of care for Medicaid beneficiaries in NC.
Footnotes
Acknowledgments
The authors thank the University of North Carolina’s Sheps Center for Health Services Research and Milton Molina for database management and analytic support; Jessica Frega from Community Care of North Carolina for assistance with obtaining the linked data; and Mekhala Dissanayake for analytic expertise.
Authors’ Contributions
C.E.B.: Conceptualization, Methodology, Formal Analysis, Writing—Original Draft, Writing—Review and Editing, Visualization C.J.V.: Conceptualization, Methodology, Formal Analysis, Resources, Writing—Original Draft, Writing—Review and Editing, Supervision, Project administration D.M.: Conceptualization, Methodology, Writing—Original Draft, Writing—Review and Editing M.K.M.: Conceptualization, Methodology, Formal Analysis, Resources, Writing—Original Draft, Writing—Review and Editing, Supervision, Project administration, Funding Acquisition.
Author Disclosure Statement
The authors report no conflicts of interest. C.E.B. was supported by an
Disclaimer
The views expressed in this publication are solely the opinions of the authors and do not necessarily reflect the official policies of the U.S. Department of Health and Human Services or the Health Resources and Services Administration, nor does mention of the department or agency names imply endorsement by the U.S. government.
Funding Information
This work was supported by the
Supplementary Material
Supplementary Appendix Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.