
Abstract
Background:
Sex-based differences are common among diseases. We aimed to investigate the differences in colonoscopy indications and its findings between males and females.
Methods:
A large, multi-center, cross-sectional, retrospective study included all colonoscopies performed between 2016 and 2021 in seven endoscopy departments. The indications and findings of the procedures were compared between males and females.
Results:
A total of 151,411 (52.6%) women and 136,519 (47.4%) men were included, aged 56.54 ± 12.9 years and 56.59 ± 12.7. Cecal intubation was similar (95.6% vs 95.5%, p = 0.251). More females had excellent or good bowel preparation compared to males (71.4% vs 65.6%). Colonoscopy due to abdominal pain, constipation, diarrhea, and anemia was higher in females compared to males (15% vs 9.9%, 3.9% vs 2.2%, and 7.6% vs 4.9%, p < 0.001, respectively), while positive FOBT, rectal bleeding and post-polypectomy surveillance and screening were more common indications among males (9.5% vs 7.8%, 10.7% vs 7.8%, and 10.8% vs 7.1%, respectively). On colonoscopy, males were found to have significantly higher colorectal cancer and polyps (0.5% vs 0.4% and 35.1% vs 24.6%). Polyp detection rates were lower in females across all indications, whereas diverticulosis rates were higher in males. However, a clinically significant difference regarding diverticulosis was observed only in patients with anemia as the indication.
Conclusions:
Notable differences exist between males and females in terms of the indications and findings on colonoscopy. This highlights the need for identifying the factors contributing to these differences and the developing sex-specific approaches for the diagnosis and management of gastrointestinal diseases.
Introduction
Sex defines the biological or anatomical variance between males and females, whereas gender differentiates the social roles and cultural norms of men and women. Differences between males and females have been described in many diseases and can affect the incidence, presentation, pathophysiology, and prognosis of the illness. These differences between males and females can be attributed to a mix of genetics, hormones, body structure, eating habits, risk factors, and physiological factors. 1 –5
The differences between males and females have been intensively investigated in different fields of medicine. For example, women have a lower risk of developing cardiovascular disease until menopause, and men have a higher incidence of heart attacks or fatal coronary heart disease. 6 Autoimmune diseases such as rheumatoid arthritis or lupus are more common among females, and sex differences are reported in the epidemiology, presentations, and prognosis of patients with autoimmune disease. The increased susceptibility of autoimmune disease could be contributed to by hormonal factors or sex chromosomes. 7 –9 In addition, differences have been reported regarding neurodegenerative diseases, Alzheimer’s disease, Parkinson’s disease, and amyotrophic lateral sclerosis, with Parkinson’s disease being more prevalent in males and Alzheimer’s disease and multiple sclerosis being more common among females. 10,11 Moreover, females are more likely to seek healthcare and adhere to medical advice. 12
With regard to gastrointestinal diseases, females have higher rates of right-sided colorectal cancer (CRC). Since right and left colon cancers differ in their developmental pathways, it has been proposed that hormonal, genetic, and environmental factors contribute to the differences in colorectal cancer between males and females. 13,14
Upper endoscopy is an important diagnostic and therapeutic modality in gastroenterology. A previous study showed significant differences regarding upper endoscopy findings between males and females related to the most common indications. 15
As opposed to upper endoscopy, there is currently only a limited amount of data published regarding the sex differences between males and females undergoing colonoscopy. Thus, the aim of the present study is to investigate the similarities and differences between males and females undergoing colonoscopy in regard to the specific indication for colonoscopy and the abnormal findings during the colonoscopy.
Methods
Study design
This was a large multi-center, cross-sectional, retrospective study of colonoscopies performed between April 03, 2016 and December 31, 2021. The study protocol was approved by the Institutional Helsinki Committee of Assuta Medical Centers (approval number 10–22). Informed consent was waived due to the retrospective, non-interventional study design.
Patients and data collection
Data were collected from seven Assuta Medical Center endoscopy departments located throughout Israel (Beer-Sheva, Ashdod, Raanana, Rishon Lezion, Haifa, Hashalom, and Ramat Hahayal). If a patient underwent multiple colonoscopies during the study period, only the initial index procedure was included. Otherwise, all performed colonoscopies in an outpatient setting were included in the study.
Data were extracted from medical records and electronic charts using the platform “MdClone.” Demographic information, indications for colonoscopy, preparation quality, cecal intubation, and the colonoscopy findings were retrieved for each patient. The colonoscopy indication was reported as one of the following: abdominal pain, positive fecal occult blood test (FOBT), rectal bleeding, change in bowel habits, constipation, diarrhea, weight loss, post-polypectomy surveillance, family history of CRC, family history of colon polyps, anemia, CRC screening, inflammatory bowel disease (IBD) follow-up, after acute diverticulitis, surveillance after surgery, anal complaints, or other. Colonoscopic findings include the following: colorectal cancer, polyp, IBD including Crohn’s disease and ulcerative colitis, diverticulosis, and colonic angiodysplasia. A patient could have more than one indication and multiple colonic findings, which were all included in the analysis. However, the indication for “screening” was considered valid only if it was explicitly documented without any additional reported indications. If other indications, such as anemia or family history of colorectal cancer (CRC), were also noted, the primary indication for the analysis was not considered to be “screening.” This ensures clarity in categorizing the data and helps to avoid misclassification of patients’ indications for colonoscopy. The indications and findings were statistically compared between males and females. Additionally, the polyp detection rate (PDR) was calculated after exclusion of patients with IBD or previous colonic surgery.
In addition, an age-adjusted analysis was performed for colonoscopy findings across different indications, sex and age groups. No significant or clinically meaningful changes were found compared to the analysis of the entire group and presented in the table.
Statistical analysis
Patient characteristics were presented as mean ± SD for continuous variables and as percentages for categorical variables. Categorical variables were compared using the chi-square test. Continuous variables were examined with the student t-test. Non-normally distributed continuous variables were reported as median (IQR) and compared using the Mann Whitney test.
All statistical analyses were performed using IBM SPSS version 26 (Chicago, USA). p-Values less than 0.05 were considered statistically significant; however, a 20% difference between females and males was considered clinically relevant. Moreover, we calculated the adjusted p-value (Bonferroni correction) for multiple comparison/testing.
Results
Patients
A total of 287,930 colonoscopies were included in the study; of these, 151,411 (52.6%) were performed on females and 136,519 (47.4%) on males.
The baseline characteristics of the study groups are summarized in Table 1. The average age among females was 56.54 ± 12.9, and without significant difference compared to males (56.59 ± 12.7, p = 0.289). No significant difference was found regarding the cecum intubation between females and males, but a higher proportion of good or excellent bowel preparation quality was noted among females compared to males (71.4% vs 65.6%).
Baseline Characteristics of the Study Groups
2L polyethylene glycol+Ascorbic acid.
Indications for colonoscopy
The indications for colonoscopy among females and males are presented in Table 2. Clear differences were noted between the sexes.
Indications for Colonoscopy Among Females and Males
The adjusted p-value for multi-testing (Bonferroni correction) for this table is <0.0029.
Statistical significance according to the adjusted p-value of <0.0029.
FOBT, Fecal Occult Blood Test; CRC, Colorectal Cancer; IBD, Inflammatory Bowel Disease.
For example, a higher proportion of women underwent colonoscopy due to abdominal pain (15% vs 9.9%), constipation (3.9% vs 2.2%, p < 0.001), diarrhea (3.2% vs 2.4%, p < 0.001), and anemia (7.6% vs 4.9%, p < 0.001) compared to males. On the other hand, males more commonly underwent colonoscopy due to positive FOBT (9.5% vs 7.8%, p < 0.001), rectal bleeding (10.7% vs 7.8%, p < 0.001) and post-polypectomy surveillance (10.8% vs 7.1%, p < 0.001).
Pathological findings of colonoscopy
The pathological findings of colonoscopy are presented in Table 3. The most common finding was a colon polyp. CRC was diagnosed slightly but statistically significantly more in males, 0.5% vs 0.4% than in females (p = 0.004). In addition, males were more likely to have colon polyps (35.1% vs 24.6%, p < 0.001. Further comparisons were performed focusing on the common colonoscopy indications of abdominal pain, positive FOBT, rectal bleeding, family history of CRC, and CRC screening. The sex-based colonoscopy findings according to these specific indications are summarized in Table 4. In these multiple comparisons, an adjusted p-value of 0.0014 was considered as statistically significant. Overall, the findings on colonoscopy varied according to the specific indication for colonoscopy, with men frequently being more likely to have specific findings than women. For example, in terms of colonoscopy performed due to abdominal pain, males had significantly higher diagnosis of polyps and Crohn’s Disease (CD) (26% vs 19.1%, p < 0.001 and 2.5% vs 1.8%, p < 0.001). For positive FOBT, males had higher diagnosis of polyps (55.4% vs 41.3%, p < 0.001). Males with a family history of CRC or CRC screening as indications were more likely to be diagnosed with polyps and colonic diverticulosis. Despite the higher frequency of anemia as an indication, CRC was significantly more common among males with anemia than females (1.5% vs 0.9%, p < 0.001).
Colonic Findings Among Females and Males
CRC, Colorectal Cancer.
Colonic Findings According to Specific Common Colonoscopy Indications
The adjusted p-value for multi-testing (Bonferroni correction) for this table is <0.0014.
Statistical significance according to the adjusted p-value of <0.0014.
CRC, Colorectal Cancer.
The PDR per indication and sex is demonstrated in Figure 1. This reveals a higher PDR among males compared to females for each indication, with the highest PDR being found when colonoscopy was performed due to positive FOBT.
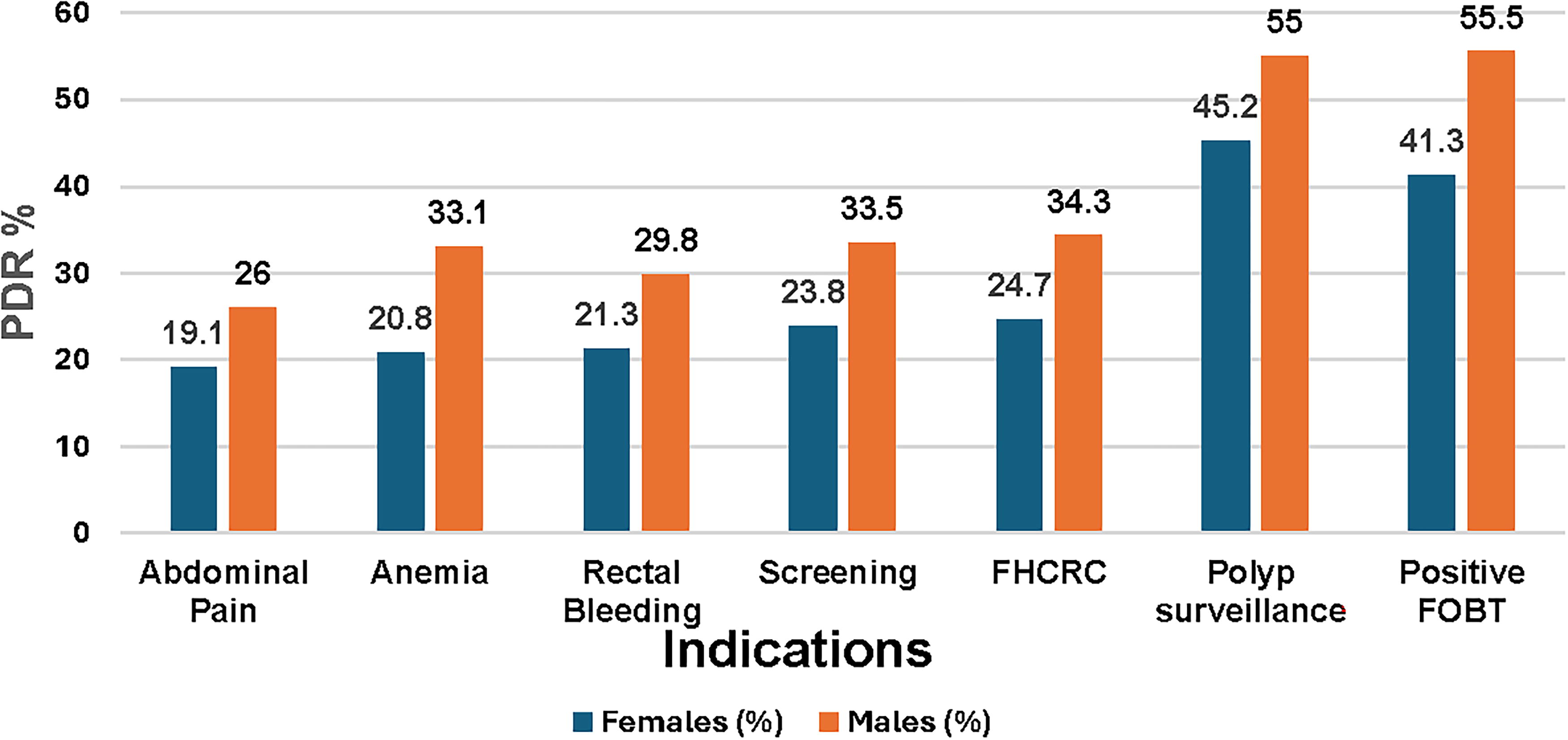
PDR per sex and indication. PDR, polyp detection rate.
Discussion
In the present study, we found significant differences between males and females regarding the indications and findings on colonoscopy.
While abdominal pain, constipation, diarrhea, family history of CRC, and anemia were more common indications for colonoscopy among females, positive FOBT, rectal bleeding, polyp-polypectomy surveillance, and CRC screening were more common among males. Some of these differences in indications can be explained by the fact that functional disorders are more common among females, 16,17 and as a result females had more complaints such as abdominal pain, constipation, and diarrhea. Rectal bleeding as an indication for colonoscopy may be a symptom of hemorrhoids, which is more common among males according to published studies. 18 –20 These differences in the prevalence of hemorrhoids may be explained by differences in body structure and diet habits between males and females, but it’s important to mention that CRC was more often diagnosed in males than females. Polyps’ follow-up as indication for colonoscopy was more common among males in our study and can be expected due to higher polyps’ prevalence among men, including the higher PDR found among males in this study.
The proportion of patients undergoing colonoscopy due to positive FOBT and colonic screening as indications was higher among males compared to females. In general, the adherence to CRC screening is higher among females compared to males. According to the national program for quality indicators in community healthcare, 66.3% of the females (aged 50–74 years) and 64.6% of the males perform CRC screening. 21 Another study also showed higher CRC screening in females (60.9%) compared to males (55.5%), with the gap in screening uptake rate maintained in all age groups. 13 In general, the positivity rate of FOBT is higher among males. 22 Additionally, males had higher rates of rectal bleeding, which could result in a positive FOBT; these factors could explain our findings.
Focusing on the pathological findings of colonoscopy, most of the abnormal findings were more prevalent among males. Again, this may be related to the higher prevalence of functional gastrointestinal disorders in females, in which no significant abnormal finding is noted on colonoscopy.
CRC was slightly but significantly more common among males compared to females undergoing colonoscopy in this study. There is extensive literature showing a higher risk of CRC among males and disparities between males and females. 13,14 In addition, the PDR was found to be higher among males undergoing colonoscopy, with polyps found in 36.6% of all colonoscopies among males compared to 25.4% among females. Previous studies focusing on adenoma detection rate (ADR) have consistently shown higher ADR among males compared to females. 23 –25 Interestingly, the PDR was found to be higher among males compared to females in all indications (abdominal pain, positive FOBT, rectal bleeding, family history of CRC, and CRC screening), with the highest PDR found among males and females undergoing colonoscopy due to positive FOBT (55.4% and 41.3, respectively). Previous studies have reported a higher prevalence of polyps among males. 26 –28 Positive FOBT also had the highest prevalence of CRC and diverticulosis. Regarding bowel preparation, similar to previous studies, we found a higher proportion of males with inadequate bowel preparation compared to females. 29 –32 We have found no difference between males and females in the cecal intubation percentage, while other studies reported female sex to be associated with incomplete colonoscopy. 33 –35
The strength of the study lies in the large number of the included subjects and the multi-center setting, but there are some limitations need to be mentioned: the lack of histopathological, size and location of polyps. Moreover, selection biases due to the outpatient setting could be a limitation of our study.
In summary, to the best of our knowledge, this is the first large database study comparing the indications and findings of colonoscopy between males and females. Understanding these sex-specific differences may be helpful for targeted decision making in terms of prevention, diagnosis, and treatment. However, further studies are required to investigate these differences more thoroughly, with the aim of gaining a better understanding of their pathophysiology. Only then can we recommend practical guidelines and targeted decision-making.
The differences between males and females found in the present study may be of clinical importance in clinical practice in terms of referring patients to colonoscopy and the likelihood of findings abnormalities during colonoscopy.
Conclusions
Significant differences between males and females regarding the indications and pathological findings of colonoscopy were found. This highlights the need for better understanding and identification of the factors contributing to these differences, as well as the development of sex-specific approaches for the diagnosis and management of gastrointestinal diseases.
Footnotes
Authors’ Contributions
All authors have contributed significantly to work and have approved the final version of the article. The article has not been published and is not being considered for publication elsewhere. We transfer the copyright should the article be published. No additional materials will be available to other researchers.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.