
Abstract
Background:
Female child welfare-involved youths who are removed from the home are at risk of commercial sexual exploitation of children (CSEC). The aim of this study was to develop a prediction model to identify those at greatest risk of trafficking.
Methods:
Data were from the Florida Department of Children and Families’ Florida Safe Families Network Database. A Cox proportional hazard regression of 60 cases and 3857 controls generated the proposed risk model.
Results:
Factors found to be associated with a higher risk of trafficking were quantified into point scores, generating the Welfare-Involved Female Sexual Exploitation Risk Assessment (WISER) tool with a cutoff of 20 points: first out-of-home placement at ≥15 years of age (11 points); run away from home in past year and age <15 years (40 points) or ≥15 years (16 points); English spoken as other language (14 points); on a psychotropic drug (17 points); congregate first placement (14 points); runaway/abducted status first “placement” (16 points); psychiatric facility experience (9 points); residential facility experience (7 points); and no time in temporary shelter (9 points). Of those who experienced CSEC, 92% had a WISER score above 20.
Discussion:
The WISER tool achieved good discrimination and calibration ability with a receiver operating characteristic for the validation data set of 0.923. The WISER tool can (1) inform risk assessment for CSEC among child welfare-involved females and (2) identify youths at greatest risk before they are harmed by trafficking.
Introduction
Commercial sexual exploitation of children (CSEC) involves sex-related crime in which minors are exploited for the commercial benefit of the perpetrator. 1 Child sex trafficking is a problem across the United States with youths generally at greater risk although estimates of its prevalence among this population are limited by obfuscation secondary to stigma, lack of awareness, and fear. 2,3
At-Risk Populations
CSEC risk factors among youth in the general population
CSEC susceptibility is not equally distributed among U.S. youth, with risk factors existing in the following four tiers: individual, familial, community, and societal. 1 Individual-level risk factors include prior abuse/neglect, homelessness, gender and sexual minority (GSM) youth, history of sexual violence, substance misuse, criminal justice involvement, racial/ethnic minority identification, and child welfare services. On a familial level, intimate partner violence and family instability are included risks. Community-level risk factors include peer CSEC involvement, isolation, gang association, lack of education, poverty, and crime prevalence. On a societal level, we can consider lack of CSEC awareness, societal sexualization, gender biases/violence, and limited resources. 1,4,5
Trafficking risk among child welfare-involved youths
Youths in the child welfare system are at heightened risk for human trafficking. 6,7 These welfare service referrals reflect survivors of serious familial dysfunction and child maltreatment, which can also increase susceptibility to human trafficking. 8 Although little is known about this population, certain risk factors have been identified. 9 First, CSEC-involved youths in the welfare system are more likely to report runaway behavior, externalizing behaviors, and endorse substance use. 9 Second, this population demonstrates “a greater degree of traumatic exposure than the overall child welfare population” and “greater levels of mental and behavioural health problems.” 9 –11 Moreover, by virtue of being in the welfare system, youths at baseline experience resource gaps, lack of connectivity, and living instability. 10
Trafficking risk among child welfare-involved youths “removed from the home”
Some literature has found that child welfare-involved youths have greater rates of housing instability than their counterparts. 12 Children taken out of their homes and placed in nonkinship foster care environments experience more behavioral problems, mental health disorders, and placement disruptions than do children in kinship foster care. 13 These adverse psychological and developmental consequences create and/or exacerbate risk factors for CSEC recruitment. With that said, failed family reunification can be just as detrimental as out-of-home and nonkinship placement. “Repeated returns to one or both biological parents followed by re-entry into out-of-home placement (i.e., failed family reunifications) were associated with youth’s sexual risk behaviours… and the total number of placement transitions youth experienced from the time they entered the child welfare system.” 14 Overall, the evidence suggests that, regardless of housing placement, the mere eviction of youths from their homes represents an unmitigated risk that has traditionally been exploited by the commercial sex industry.
Trafficking risk among child welfare-involved youth: Females
Gibbs et al (2018) found that the greatest risk factor for CSEC among welfare-involved youths was female gender identity. 15 Up to 86.1% of females in the child welfare system reported a human trafficking allegation in their lifetime as opposed to 13.9% of their male counterparts.sss This may be partially explained by findings that—among the population using welfare services—females were more likely to also have risk factors for CSEC recruitment (e.g., sexual abuse, witnessing intimate partner violence, emotional abuse). 16
Harms of CSEC
CSEC-related trauma results in physical and psychological scars that profoundly affect youths’ well-being. A 2017 study by Greenbaum et al. found some of the physical health effects to include “traumatic injury from sexual and physical assault or work-related injury, sexually transmitted infections, non-sexually transmitted infections, chronic untreated medical conditions, pregnancy and related complications, chronic pain, complications of substance abuse, and malnutrition and exhaustion.” 17 They noted the mental health consequences to encompass mood disorders, stress/adjustment disorders, self-harm, PTSD, sleep dysfunction, anxiety, dissociative disorders, and anger management problems. 17
Need for CSEC-targeted prevention tools
The U.S. Federal Strategic Action Plan on Services for Victims of Human Trafficking in the United States 2013–2017 tasked federal governmental agencies that work most closely with the child welfare systems “to improve their understanding of the causes and effective interventions” to prevent CSEC. 18 As child welfare systems operate in resource-constrained environments, it is critical that they be informed with evidence-based tools to help identify those youth at highest risk. To date, there have been no risk-stratification instruments developed. The aim of our study was to develop a prediction model to identify those at greatest risk of CSEC among a known high-risk group: females in the child welfare system who were removed from their homes.
Materials and Methods
Data collection
Secondary analysis was performed of data extracted from the Florida Department of Children and Families’ Florida Safe Families Network database. We included 3917 female (persons assigned female at birth) youth removed from their homes between January 1, 2013, and August 23, 2017, in central Florida. The state of Florida was one of the first to collect trafficking data on youths involved in the child welfare system and thus represents an important source of information to understand trafficking risk among child welfare-involved youth. A youth’s trafficking status had been determined by the DCF screening tool—consistent with trafficking definitions in U.S. law. Details of the tool are described in detail by Landers’ text “Examining Evidence of Reliability and Validity in Florida’s Human Trafficking Screening Tool.” 19 This study was conducted in accordance with ethical standards from the 1964 Declaration of Helsinki and exempt by the Partners Human Research Committee (Protocol #:2016P001399/PHS).
Analysis
We used descriptive statistics to compare the distribution of baseline risk factors for 60 cases and 3857 controls (total = 3917 subjects). We compared distributions between cases and controls for each variable via univariate Cox proportional hazards models adjusted for updated age. As subjects entered the welfare system at different ages and were involved for different time periods, we used time-to-event analyses with Cox proportional hazards model. Time was defined as current age minus age at first placement. Age was used as a time-dependent covariate in the model. Both age and age at first placement were considered risk factors. We fit the Cox model, h(t) = h0(t)exp(β1 x1 + … + βk xk), where the censoring variable was set to 1 for cases and 0 for controls.
We used the forward stepwise selection option with a p value <0.05 to identify significant risk factors. For each risk factor, we multiplied the beta coefficient with 10 and rounded to the nearest integer to obtain the point score (Pk) for each category of a given variable, k = 1, K. Higher point values connote higher risk. To understand the difference between the univariate results and the stepwise results, we performed chi-squared tests for association between each pair of predictor variables. Based on the selected factors, we derived a risk score given by S =
To validate the model, we used the variables identified in Table 2 and split our sample into a derivation subset (two-thirds of our sample, n = 40 cases, 2572 controls) and validation subset (one-third of our sample, n = 20 cases, 1285 controls). We then re-estimated the beta coefficients using the derivation subset and obtained new values for the beta coefficients and point scores for each variable. Point scores from the derivation subset were applied to the validation subset. New values were obtained for the sensitivity and specificity at various cut-points (Table 5). All analyses were performed using SAS Version 9.4.
Results
Table 1 shows descriptive statistics and bivariate analyses for baseline risk factors among cases and controls. CSEC survivors were more likely to be older than 15 years (77%, n = 46) and to be older than 15 at the time of their first welfare placement (38%, n = 23). CSEC survivors were also more likely to have a runaway from home in the past year and to have run away more times than controls in the past year. CSEC was more common among youths whose first placement was a congregate care (i.e., group home) setting (67%, n = 40) and those who had run away or been abducted (10%, n = 6) before their first placement. Youths with multiple placements in the child welfare system (95%, n = 57) or a placement different from family care (e.g., group home, specialized facility) were more likely to experience CSEC. Of note, there was no significant difference between cases versus controls with respect to either race or to estimated median household income.
Descriptive Statistics and Bivariate Analyses for Baseline Risk Factors Among Child Welfare-Involved Females Between January 1, 2013, and August 23, 2017, According to Trafficking Status
Mean (SD), mean (standard deviation); median (IQR), median (interquartile range); n (%), frequency (percentage) of category level.
p-Values calculated from univariate analyses.
Hazard ratio calculated using Cox-proportional hazards model with one risk factor at a time, with no trafficking report as reference and controlling for age <15.
Hazard ratio calculated using Cox-proportional hazards model with one risk factor at a time, with no trafficking report as reference.
Based on zip code of residence before entering the welfare system.
Chi-squared test of independence.
Mantel–Haenszel chi-square.
Fisher’s exact test.
Wilcoxon rank-sum test.
Two-sample t test.
Significant Risk Factors Associated with Risk of Commercial Sexual Exploitation of Children Among Child Welfare-Involved Females Based on Stepwise Regression of Cox-Proportional Hazards Model
Ran away before entry into child welfare system.
ESOL, English spoken as other language.
We developed a Cox-based risk prediction model (Table 3) titled WISER—Welfare-Involved Female Sexual Exploitation Risk Assessment. The distribution of risk scores was similar in the validation data set and the full data set (Fig. 1a and b).
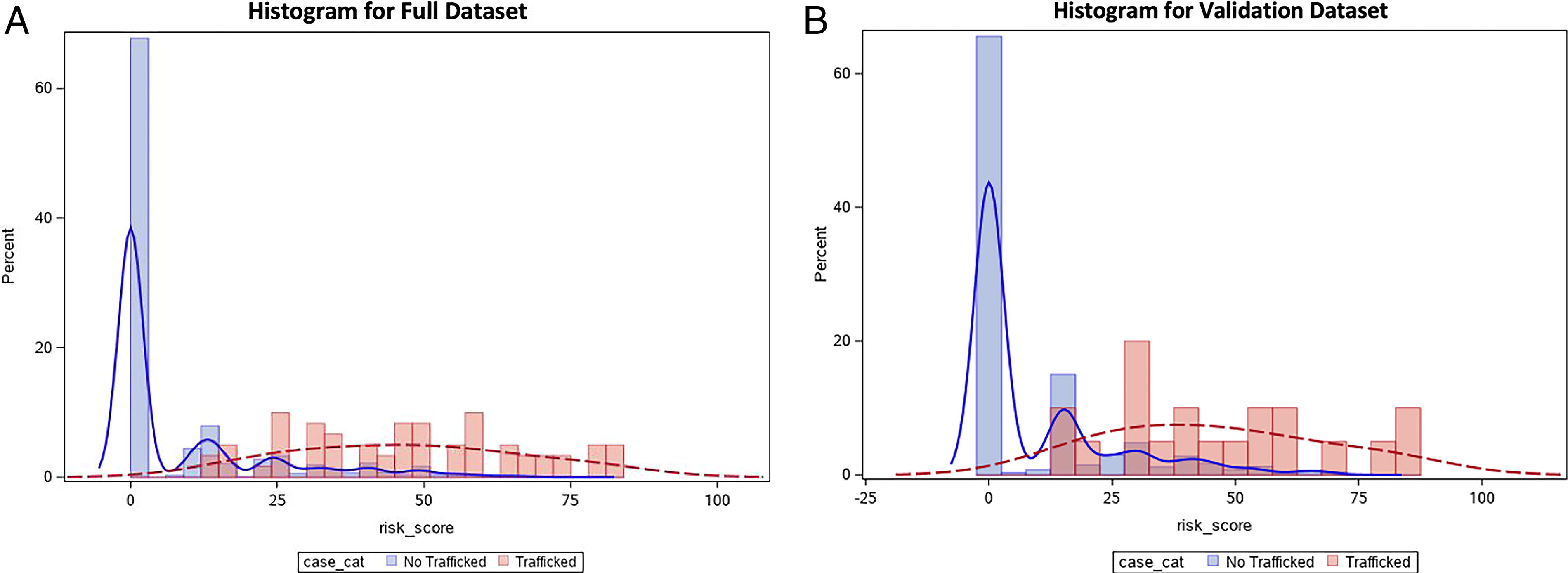
Distribution of risk scores from the Cox-based risk prediction model among child welfare-involved females in the
WISER Tool, Cutoff = 20 Points
ESOL, English spoken as other language; WISER, Welfare-Involved Female Sexual Exploitation Risk Assessment.
None of our cases had a risk score of zero. Up to 92% of cases had a risk score above 20, and 83% of controls had a score below 20 (Tables 4 and 5). Girls in the welfare system younger than 15 and with an episode of running away were found to be at high risk for CSEC with a risk score of 40 points. The specificity of cutoff points was similar between the full data set and validation data set, but the sensitivities decreased slightly in the validation data set (Fig. 2a and b). The area under the receiver operating characteristic (ROC) curve (AUC) for the full data set was 0.943 and for the validation data set was 0.923.

ROC curve demonstrating sensitivities and specificities of cutoff points used by the Cox-based risk prediction model in
Cox-Based Risk Prediction Model for Detection of Commercial Sexual Exploitation of Children Among Child Welfare-Involved Females for Full Data Set and Validation Data Set
Comparing Sensitivity and Specificity of Risk Scores for Commercial Sexual Exploitation of Children Among Child Welfare-Involved Females According to Test Positivity in Full Data Set and in Validation Data Set
Discussion
Our study developed a prediction model to identify those at greatest risk of trafficking in the child welfare system, who were removed from their homes. The WISER tool provides a scoring system to support child welfare and youth-serving organizations identify those at highest CSEC risk. The risk point scores are as follows: first out-of-home placement at ≥15 years of age (11 points); run away from home in past year and age <15 years (40 points) or ≥15 years (16 points); English spoken as other language (12 points); on a psychotropic drug (17 points); congregate first placement (14 points); runaway/abducted status first “placement” (16 points); psychiatric facility experience (9 points); residential facility experience (7 points); and no time in temporary shelter (9 points). It is reasonable to consider female child welfare-involved youth with a score of at least 20 to be at greatest need of trafficking prevention/intervention resources.
Risk factor: First out-of-home placement at ≥15 years of age (11 points)
As this is a vulnerable population driven to underreporting, it is difficult to assess the age of youth entry into CSEC. Our study demonstrates that females placed out-of-home by child welfare at the age of at least 15 years are at increased CSEC risk compared with minors younger than 15 years (11 points). It appears that individuals who enter the welfare system in their late teens are currently at an age that is particularly susceptible, which consequently increases their risk of CSEC recruitment. A recent analysis of victim reports by the Polaris Project elicited the projection that age of CSEC entry was 17 or younger for 44% of survivors and 19 years on average. 20 In addition, youths who enter the welfare system later may exhibit riskier behaviors although without the resources and support cultivated via more longitudinal involvement with welfare. One supporting study showed that youths who were older at the time of first placement were predisposed to adverse consequences, such as exhibiting runaway behavior from foster care. 21 Similarly, an analysis by Villodas et al. assessed children’s long-term placement trajectories after early involvement in the child welfare system and found that children in the unstable trajectory were oldest at initial removal. 22 Our results are consistent with these studies suggesting that older ages at first placement may have challenges navigating welfare, higher risk behaviors, and/or increased CSEC susceptibility by virtue of age alone.
Risk factor: Runaway behavior <15 years (40 points) or ≥15 years (16 points)
Youths younger than 15 who ran away from home in the past year were the subgroup with the highest WISER score (40 points). Moreover, we found a high correlation between the number of days a youth ran away from home and risk of CSEC among both age groups. Runaway behavior is particularly high among minors with repeated removals from the home, placement in group or residential care facilities, lack of kinship placements, and separation from sibling groups. 21 Many of the risk factors that predispose youths to CSEC recruitment (e.g., family/home dysfunction, history of violence/trauma) also contribute to runaway behaviors. For example, The National Longitudinal Study of Adolescent Health (Add Health) demonstrated that youths exposed to more disruption in the family were more likely to run away. 22 Among runaway youths, up to 70% of females and 24% of males have been found to be victims of child sexual abuse and 35% of both genders reported a history of physical abuse. 23,24
The aforementioned Add Health study demonstrated that runaway behavior was more common among adolescents in urban environments that may reflect greater shelter opportunities in population-dense areas. 25 Unfortunately, those opportunities can also serve to increase exposure to traffickers. Running away from home may further leave youths with outstanding needs that expose them to traffickers, peers in CSEC, or the juvenile justice system thereby coupling increased exposure to recruitment efforts with increased need for bare necessities. 26 In fact, 20–30% of youths living on the street are estimated to have run away from foster care or group home placement, and up to 1 in 6 youths may experience CSEC during a runaway episode from care. 27 The dramatically high risk for those running away younger than 15 warrants further study. It is possible these youths have fewer protective factors in their communities (school, family, other adults) than their older counterparts. 28
Unfortunately, runaway behavior may extend beyond the confines of the home and include efforts to escape supports and treatment programs. A qualitative analysis by Sapiro et al. revealed varying interpretations of runaway behavior as “an indication of program failure; a symptom of individual pathology; or a normal aspect of the process of leaving an abusive relationship.” 29 Data from this study, in addition to the literature, compound the association that runaway youths are more likely to be trafficked by virtue of (1) preexisting risk factors responsible for youths leaving home in the first place that are independently associated with susceptibility to CSEC and (2) unstable/unsafe living situations due to runaway status that increase exposure to perpetrators of CSEC.
Risk factor: English spoken as other language (12 points)
Those who spoke English as other language (ESOL) had a WISER score of 12 points. This variable, ESOL, refers to those individuals whose preferred language was not English or not solely English. Many survivors of trafficking are international migrants and/or undocumented laborers with limited English proficiency. 30,31 The European Commission’s “Study on High-Risk Groups for Trafficking in Human Beings” also found children trafficked from foreign countries as less likely to understand the new language and more likely to lose opportunities for escape. 30 For example, minors may perceive traffickers and traffickers’ affiliates as speaking their native language and therefore fear that those interpreters speaking the native language are allying with the trafficker against them. 30 This language barrier can further result in limited awareness of one’s rights, impede access to help/resources, worsen isolation, and exacerbate manipulation. 31
Individuals who speak English as a second language face greater barriers to resources, forms of internalized racism, and overall structural violence that place adolescents of these populations at disproportionately increased CSEC risk.
Epidemiological components of societal racial disparities, such as primary language, are risk factors for CSEC recruitment, particularly because CSEC itself is built upon a foundation of racialized sexual exploitation. Minors of non-Hispanic Black and Hispanic ethnicities have disproportionately higher representation in CSEC. 32 Prior studies have shown that minority subgroups enter the commercial sex industry about 2.5 years younger than their White counterparts, which has been largely attributed to the disadvantages of lower socioeconomic status, economic opportunity, and overrepresentation of CSEC in poverty-stricken communities/homelessness. 33 Once again, the very structural inequalities that marginalized youths of color face simultaneously increase their vulnerability to CSEC exploitation. In her piece, Butler argues that discrepancies of ethnic representation in CSEC stem from systemic factors that include poverty, denial of education/employment opportunities, and uneven access to health/health care. 34 To make matters worse, Hurst argues that structural racism reinforces internalized racism and creates further disparity. 35 “Youth who are part of a marginalized race and who have experienced racism or colourism may have internalized these acts of oppression. Once internalized, these feelings may lower their sense of self-worth thereby making them more susceptible to those who seek to exploit them.” 35
Risk factor: on a psychotropic medication (17 points)
The second highest WISER CSEC score in our study (17 points) among child welfare-involved female youths was being prescription of psychotropic medications by a clinician. Psychotropic drugs are medications used to treat mental health disorders. To our knowledge, this is the first relationship between psychotropic medication and CSEC risk that has been described. In our study, this variable may represent severe and complex trauma experienced by CSEC survivors. 1,4,5 A strong link between childhood trauma and CSEC recruitment has been established. 1,4,5,36 This past psychiatric history of trauma—before recruitment into CSEC—may be responsible for the development of psychiatric issues, exacerbation of preexisting psychiatric issues, and ultimately CSEC recruitment. For example, interpersonal violence has been associated with increased risk of depression, suicide, eating disorders, posttraumatic stress disorder, and substance-use disorder. 37 –40
The compounded psychiatric needs from preexisting trauma may then complicate and jeopardize medical care for youths. Both consequences could ultimately confound screening, evaluation, and treatment of the underlying trauma that later serves to exacerbate patient’s risk of involvement in CSEC. There are several challenges associated with diagnosing PTSD among youths who have a background of extensive complex trauma. Cohen and Scheeringa argue that the following four major problems exist: (1) sensitivity of the diagnosis, (2) children who are symptomatic but do not demonstrate enough symptoms, (3) developmental considerations, and (4) assessment challenges. 41 In their study, Cohen and Scheeringa found that children with long histories of trauma were not being diagnosed with PTSD. This stemmed from the belief that symptoms did not fit PTSD or instead reflected PTSD plus a comorbid disorder (which drove treatment for the comorbid conditions), both of which ultimately undertreated the trauma. They also found that the number of criteria met was more important in the given psychiatric diagnosis than the intensity of symptoms, which drove underdiagnosing. Cohen and Scheeringa identified certain criteria for the PTSD diagnosis (irritability, outbursts of anger, avoidance) that may be affected by child development, which contributed to misdiagnosis. The burden of diagnostic interviews and self-report instruments were oftentimes more difficult for children. Ensuring the accuracy of information sources was more challenging, which allowed for uncertainty. 41
The role of PTSD and prior trauma in a youth’s wellness can be missed when it is not recorded in patient charts and obscured by treatment with a psychotropic medication. Meltzer et al. noted that symptoms of ongoing or preexisting trauma may be misdiagnosed as primarily a mental health disorder (most commonly depression, anxiety, panic disorder) and mistreated with psychotropic medications such as SSRIs. 42 In their study among primary care patients with PTSD, few patients had a PTSD diagnosis recorded in their medical records, but “nearly 50% received MH [mental health] treatment; either an SSRI and/or a visit with MH profession.” 42 Along that same vein, in a 2020 study on trafficked youths, ADHD was found to be highly prevalent. The authors noted that symptoms of ADHD mirror avoidant symptoms of PTSD, but ADHD is more common in the general population. 43 A physician unaware of a patient’s trafficking history may misdiagnose PTSD as ADHD or other diagnoses that present similar to PTSD such as bipolar disorder, conduct disorder, oppositional defiance disorder, and a psychotic disorder. 43 The authors argue that the diagnoses of ADHD, bipolar disorder, conduct disorder, oppositional defiance disorder, and psychotic disorder, all of which may lead to prescription of psychotropic medications, may be misdiagnoses of complex PTSD. 43 There is a susceptibility to misdiagnose trauma for more prevalent primary mental health disorders seen in a given population and mistreat according to that incorrect diagnosis. Our identification of psychotropic drug administration as a significant risk factor and as one of our highest point scores is likely due to mechanisms that underevaluate, underdiagnose, misdiagnose, and mistreat trauma. The unrecognized trauma may then predispose youths to CSEC exploitation.
Risk factor: Psychiatric facility experience (9 points)
Our study found that those had who had spent time in a psychiatric facility were at higher risk of CSEC than their peers with a WISER point score of 9. Psychiatric inpatient hospitalization represents mental health needs of the direst nature. Several studies have already identified a strong need for psychiatric care among victims of CSEC. Depression, anger, anxiety, attachment problems, self-harming behaviors, and mental health disorders are the most common psychiatric diagnoses that have been associated with this population alongside common risk factors that include a history of family dysfunction, sexual abuse, physical abuse, violence with sex, drug/alcohol use, and multiple drug use. 5,44,45 A history of child sexual abuse in particular may significantly affect psychological factors associated with CSEC and exacerbate adverse psychiatric complications caused by involvement with CSEC. 46
The results of this study bolster existing literature on the relationship between mental health difficulties, a history of trauma/abuse, and child sex-trafficking. Specifically, the use of “time spent in a psychiatric facility” as a variable in our study examines mental health challenges that are disruptive enough to require intensive medical intervention, and this variable thereby focuses on the severity of CSEC survivors’ psychiatric needs. In a 2010 retrospective analysis of patients referred for CSEC, 75% to 80% of sex-trafficked youths had established a clinical touchpoint within the last 6 months. 47 This was seen primarily in the emergency department and secondarily in a primary care setting with more than 25% of the chief concerns for these clinical touchpoints involving psychiatric issues. 47 In a 2017 study, most of the youths (66%) referred for CSEC had a previous psychiatric diagnosis and almost half (46%) required psychiatric admission in the year preceding the CSEC referral. 45 These studies establish a baseline need for psychiatric care and mental health services among youths recruited into sex trafficking, a baseline need that is quite significant. Notably, when compared with a control group of nontrafficked children, victims of sex trafficking had longer periods of contact with mental health services, which may have been due to longer duration of mental health difficulties and/or more complex social needs/care coordination. 48
With that said, it is not clear from these findings whether the mental illness correlated with CSEC is a risk factor and/or an adverse complication of CSEC. Moreover, institutional-based care has been the first-line treatment for patients with complex serious emotional, mental, and behavioral needs. Further research is necessary to determine whether causality is inherent in the relationship between CSEC and mental illness as well as what the best approach to rehabilitation for these patients might be.
Risk factor: Runaway/abducted as first “placement” (16 points)
Our analysis showed that when runaway/abduction represented the first moments away from home in child-welfare involvement, there was a WISER score of 16 points. While “runaway” and “abduction,” are clearly two distinct entities, for this category, the data set did not disaggregate them. The association between CSEC risk and runaway status is discussed above in the context of runaway timing and its unique risk relative to age. Many of the risk factors that predispose youths to exploitation by traffickers (e.g., family/home dysfunction, history of violence) also spark runaway behavior. 25 Runaway behavior may reflect “program failure or a normal aspect of the [child’s] process of leaving an abusive relationship.” 29 The National Longitudinal Study of Adolescent Health (Add Health) demonstrated that family structure was a strong predictor of youths running away from home with higher family instability associated with higher runaway behavior. 25 Among runaway youths, up to 70% of females have been found to be victims of child sexual abuse, and 35% of all children reported a history of physical abuse. 23 Running away in itself increases the risk of CSEC, and similarly CSEC increases the risk of runaway behavior. 27 Regarding abduction, there is limited extant research on its intersection with CSEC, while disinformation and sensationalism abound. 49
Risk factor: Type of first placement as congregate (14 points)
In line with these studies, our results also found congregate care and CSEC risk to be strongly associated with a high WISER point value of 14. Our finding is not surprising, given that each of the predictors for congregate care placement simultaneously serves as a risk factor for human trafficking exploitation via unstable access to resources, support, and emotional regulation that cumulatively affect youth wellness. 50 –52 Congregate care is used as a last resort for the placement of youths in out-of-home child welfare services. Youths placed into congregate care are more likely to carry a psychiatric diagnosis and experience worse outcomes than their counterparts—homelessness, unemployment, wellness issues, substance misuse, and altercations with the law. 50,52 First placement in a non-kin home, older age, emotional/behavioral health concerns, ADHD, Black race, and previous psychiatric hospitalizations have all been found predictive for placement into congregate care. 51 Victims of physical abuse and neglect placed into group homes comprise up to 40% of minor arrests in the welfare system, which is a hypothesized interaction of developmental status, peer interactions, and the context of congregate care placement. 53 Youths placed into congregate care strongly voice a desire for better support from care providers to supplement existing family relationships, tools for long-term achievement, emotional regulation guidance, and connectivity to peers. 54 These self-identified needs are derived from disruptions in youths’ environments that interfered with developmental trajectories and affected their well-being. 54 A compromised sense of identity and wellness has been established as CSEC risk factors, which makes this population particularly vulnerable. 54
Risk factor: No time in temporary shelter (9 points)
Having spent no time in temporary shelter was found to have a point value of 9 in our study and was significantly correlated with CSEC victimization (p = 0.017). This finding is counter to existing CSEC and youth risk data and deserves further study. It is also the first time this relationship has been described in the literature. It is possible that runaway youth, or those who are kicked out of the home who can get into an emergency shelter, may have access to supports and resources not available to them if they were alone on the streets. There is a complex relationship between placement in out-of-home care, child maltreatment, and emergency shelter placement. 55 Supportive housing models (emergency shelters) are used by child welfare services to provide short-term care for youths while permanent placements are secured, serving as temporary first placements. 56 Characteristics associated with initial placement in emergency shelter for at least 30 days include older age, dependency, kin with barriers to involvement, and the child welfare agency involved. 56
Risk factor: Residential treatment center experience (7 points)
Time in residential treatment center had the lowest point score of our study (7 points). Residential treatment centers (RTCs) are the highest level of care available for youths in child welfare. 57 The number of youths with preexisting social and emotional disturbances within RTCs has been uptrending, possibly reflecting the reliance on RTCs as long-term care. However, these facilities often lack adequate staff-to-child ratios, defined period for treatment, and drive for permanency planning, all of which affect the quality of these youths’ care. 57 Among youths accessing the highest levels of treatment (RTCs and therapeutic foster care) within child welfare services, a high prevalence of mental and behavioral health disorders (psychotropic/antipsychotic medication, substance misuse, sexual perpetration history, suicidality history, prior hospitalization at psychiatric facilities) was found. 58 The measures of emotional vulnerability are also shared by youths vulnerable to trafficking exploitation. 59 Up to 30% of youths in RTCs are known victims of childhood sexual abuse, 25% by more than one perpetrator, and 70% by a family member. 59 Although RTCs can be beneficial, our findings suggest that without sufficient resources the factors that increase child welfare-involved youths’ likelihood for referral to an RTC also increase their vulnerability to CSEC.
Limitations
This study had several limitations. It is limited in scope to a subgroup of child welfare-involved youth: those assigned female at birth in the state of Florida who were removed from their homes. The validation of the WISER tool was limited by internal validation. Results should be replicated in other data sets, including expansion to other genders, geography, and racial/ethnic identities. Given this was a secondary data analysis, we were limited by the categories and types of data collected by child welfare in the state of Florida at the time. For example, the data set grouped runaway and abducted status together although these are distinct outcomes. Furthermore, gender-diverse experiences and sexual orientation are not captured. There are likely cases of trafficking that were not captured by the implementation process surrounding the CSEC screening tool. Finally, by definition, the risk factors identified connote correlation, not causation.
Conclusion
Eradicating human trafficking requires a public health approach guided by evidenced-based prevention tools. 60 –62 Child welfare-involved youth assigned female at birth are known to be particularly vulnerable to CSEC. The WISER tool provides a scoring system to help child welfare and youth-serving organizational staff identify those at the highest risk of trafficking. Ninety-two percent of child welfare-involved females who were victims of human trafficking had a risk score above 20, while 83% of those who were not victims of human trafficking had a risk score below 20. It is reasonable to consider female youth with a score of 20 or greater to be at greatest need of a higher intensity of supportive resources. The WISER tool can (1) inform risk assessment for CSEC among child welfare-involved females and (2) identify youths at greatest risk before they are harmed by human trafficking.
Footnotes
Authors’ Contributions
H.S. was responsible for conceptualization, data curation, funding acquisition, investigation, methodology, project administration, resources, supervision, writing (original draft preparation), and writing (review and editing). J.P. was responsible for conceptualization, investigation, writing (original draft preparation), and writing (review and editing). R.G. was responsible for conceptualization, data curation, methodology, and writing (review and editing). Y.M. was responsible for formal analysis, methodology, validation, and writing (review and editing). Y.M. was responsible for formal analysis, methodology, validation, and writing (review and editing).
Author Disclosure Statement
The authors have no disclosures or conflicts of interest to discuss.
Funding Information
The authors have no funding sources to report.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.