
Abstract
Background:
Pregnancy anxiety increases the risk of preterm birth but less is known about the impacts on glucose intolerance during pregnancy, such as gestational diabetes mellitus (GDM). The present study examined the relationship between pregnancy anxiety and the risk of GDM in a prospective cohort Centering and Racial Disparities (CRADLE) study of racially diverse pregnant women in the United States.
Methods:
This is a prospective analysis among racially diverse pregnant women in the United States who enrolled in the CRADLE study. Pregnancy anxiety was assessed twice using the Pregnancy-Specific Anxiety Scale (PSAS): the baseline survey at <20 gestational weeks (GW) and the second survey at >30 GW. GDM was screened at 24–30 GW and diagnosed based on the Carpenter and Coustan criteria. The associations of baseline PSAS score (>9 [median] versus ≤9) and PSAS score change with GDM risk were estimated using multivariable logistic regressions with adjustment for potential confounders.
Results:
Among a total of 2,310 women (40.74% Black, 20.91% Hispanic), 154 (6.67%) developed GDM. No association was found between baseline PSAS and GDM (adjusted odds ratio [OR]: 0.99; 95% confidence interval [CI]: 0.70–1.42) after adjusting for confounders. Individuals with an increased PSAS during pregnancy had 52% higher GDM risk (adjusted OR: 1.52, 95% CI: 1.04–2.23) compared with those with no change or decreased scores.
Conclusions:
Pregnant individuals who increased their pregnancy-specific anxiety level during pregnancy had a higher risk of developing GDM.
Clinical Trials Registration Identifier:
NCT02640638. Registered with ClinicalTrials.gov December 29, 2015. Study recruitment began February 24, 2016.
URL of ClincialTrials.gov registration site: https://clinicaltrials.gov/ct2/show/NCT02640638?term=NCT02640638&draw=2&rank=1
Introduction
Pregnancy-specific anxiety, characterized by pregnancy-specific concerns such as fetal health, fetal loss, and newborn care, is common during pregnancy, affecting 22.9% of pregnant individuals. 1 Previous research has shown that pregnancy-specific anxiety increases the risk of preterm birth and poor child development. 2,3 However, less is known about the impact of pregnancy-specific anxiety on metabolic complications such as gestational diabetes mellitus (GDM).
GDM, defined as glucose intolerance with first onset in pregnancy, is one of the most common pregnancy complications and has profound adverse health impacts on both pregnant individuals and their offspring. 4 People with GDM have an increased risk of preeclampsia, cesarean delivery, shoulder dystocia, as well as an increased lifetime risk of type 2 diabetes and other cardiometabolic disorders. Additionally, their offspring are at an increased risk for macrosomia, neonatal hypoglycemia, being large for gestational age, and future type 2 diabetes. 4 –6
GDM has multiple risk factors, including genetic, maternal age, race, lifestyle, 7 and psychological factors. 8 Growing evidence has suggested that psychosocial factors such as stress, trait anxiety, and depressive symptoms are important risk factors for developing GDM and calls for more research in this area. 9,10 A recent study in China reported that pregnancy-specific anxiety was associated with 56% higher odds of GDM 11 ; however, the anxiety was only measured once at early pregnancy [i.e., 8–14 gestational weeks (GW)] and using an instrument which was not designed to capture pregnancy-specific anxiety. In addition, the relationship of pregnancy-specific anxiety and GDM has not been widely examined in other populations. Therefore, we aimed to examine whether pregnancy-specific anxiety is associated with GDM risk among racially diverse pregnant individuals in the United States.
Materials and Methods
Study population
This study included pregnant individuals who participated in the Centering and Racial Disparities (CRADLE) study, a randomized controlled trial that compared a group-based model of prenatal care with the traditional individual prenatal care among 2,348 pregnant individuals aged 14–45 years in Greenville, South Carolina, between February 2016 and March 2020. 12 –14 This study was jointly reviewed and approved by IRBs of Prisma Health, Clemson University, and University of California at Los Angeles. The exclusion criteria of the CRADLE study included medical complications (pregestational diabetes, severe chronic hypertension, active pulmonary tuberculosis, massive morbid obesity, or severe psychiatric illness), multiple gestation, lethal fetal anomalies, and low literacy. There were three interview data collection periods in the CRADLE study: (1) during the second trimester (baseline visit between 8 and 23 GW), (2) during the third trimester (>30 GW), and (3) postpartum data collection. In the current study, we combined those who received group and individual prenatal care and analyzed data as a cohort study. There was no difference in GDM incidence between the two prenatal care groups in the CRADLE study. In the present study, we further excluded participants who had missing information on pregnancy-specific anxiety at baseline visit (n = 38). Therefore, a total of 2,310 women were included in the study analytic sample.
Pregnancy anxiety
We assessed pregnancy-specific anxiety using the Pregnancy-Specific Anxiety Scale (PSAS) in the second trimester (baseline <20 GW) and the third trimester (>30 GW). PSAS was developed from a factor analysis of a larger pool of items focusing on pregnancy-specific affective states by Dunkel-Schetter et al. 15 The PSAS included four anxiety-related adjectives (anxiety, concerned, afraid, and panicky) to describe a pregnant individual’s feelings about pregnancy. Previous studies have reported the associations between PSAS and preterm birth 16 or shorter gestation. 17 In the questionnaire, an individual was asked to select one of the five frequencies of feelings (never, rarely, sometimes, often, and always) for the question: “In the past week, how often have you felt (adjectives listed above) about being pregnant…”. Giving the scores 1 to never, 2 to rarely, 3 to sometimes, 4 to often, and 5 to always, the summation scores of all four questions is the individual’s PSAS. The maximum score of PSAS is 20, with the higher scores indicating greater anxiety levels. 2,17
In the present study, we used both the second trimester (baseline) PSAS and the change in PSAS (PSAS change) as the exposures. Because there is no clinical cut-off point of PSAS, we use the PSAS median score of all the participants in this study (PSAS = 9) as the cut-off point to divide our participants into high and low PSAS groups. PSAS change was defined as the difference between PSAS measured in the third trimester and the second trimester (baseline). Increased anxiety was defined as any increase of PSAS from the second trimester to the third trimester, while no change/decreased anxiety was defined as the same or any decrease of PSAS from the second trimester to the third trimester.
Outcome measurement
The participants were screened for GDM between 24 and 30 GW with the two-step approach. First, the 50-g oral glucose challenge test (OGCT) was performed. Those who had OGCT results >200 mg/dL were considered diagnostic for GDM. If OGCT results were 140–200 mg/dL, participants were given another 100 g, 3-hour oral glucose tolerance test (OGTT). GDM was diagnosed if participants had two elevated values from the OGTT results (i.e., fasting ≥95, 1 hour ≥180, 2 hours ≥155, or 3 hours ≥140 mg/dL) according to the Carpenter and Coustan criteria. 18
Confounding factors
In the present study, we controlled the following confounding factors based on the data from the baseline visit: age (continuous variable), prenatal care group (individual care or group care), body mass index (continuous variable), smoking during pregnancy (yes, no, prefer not to answer or missing), drinking during pregnancy (yes, no, prefer not to answer or missing), marijuana use during pregnancy (yes, no, prefer not to answer or missing), race and ethnicity (Black, Hispanic, White, Other Race), marital status (married, other relationship, prefer not to answer or missing), education level (below high school, high school or greater, other/prefer not to answer or missing), employment status (full time, part time, unemployed, prefer not to answer or missing), and household income (<$10,000, $10,000–$20,000, >$20,000, don’t know/not sure, prefer not to answer or missing).
Statistical analysis
We categorized the second trimester (baseline) PSAS as high versus low (by median) and PSAS change as increased anxiety versus no change/decreased anxiety. In the descriptive analysis, we used the Student’s t test and chi-squared test to compare the basic characteristics between those who had low second trimester (baseline) PSAS and those who had high second trimester PSAS.
We applied multivariable logistic regression to estimate odds ratios (ORs) and 95% confidence intervals (CIs) of the associations between pregnancy anxiety (both baseline and change PSAS) and GDM risk, adjusting for confounding factors listed above. Among the 2,310 participants, 1,877 had two PSAS scores available, allowing us to measure change data. We also conducted three sensitivity analyses. First, among the 1,877 participants with PSAS change data, 1,730 (94.7%) participants had their third trimester PSAS measurements after their glucose tolerance screenings, indicating the majority of participants knew their GDM status prior to their third trimester PSAS measurements. Therefore, we conducted a sensitivity analysis that was stratified by the availability of participants’ glucose tolerance screenings prior to their third trimester PSAS measurements. There were 51 participants who did not have second survey dates (third trimester PSAS measurement dates) so the relationship between the PSAS score and GDM screening was not possible to calculate. The analytic sample sizes are shown in Figure 1. Second, we observed a total of 170 participants had their GDM screenings before 24 GW, and 55 of them were diagnosed with GDM. Thus, we further conducted a sensitivity analysis for the association between PSAS and GDM by excluding women who had GDM screenings before 24 GW and were diagnosed with GDM. Third, considering we used PSAS = 9 as the cut-off point for high and low PSAS groups at baseline, we also applied 9 as the cut-off point for PSAS change and divided the participants into four groups: (1) baseline ≤9 and follow-up ≤9 (continuously low anxiety), (2) baseline ≤9 and follow-up >9 (increased anxiety), (3) baseline >9 and follow-up ≤9 (decreased anxiety), (4) baseline >9 and follow-up >9 (continuously high anxiety).
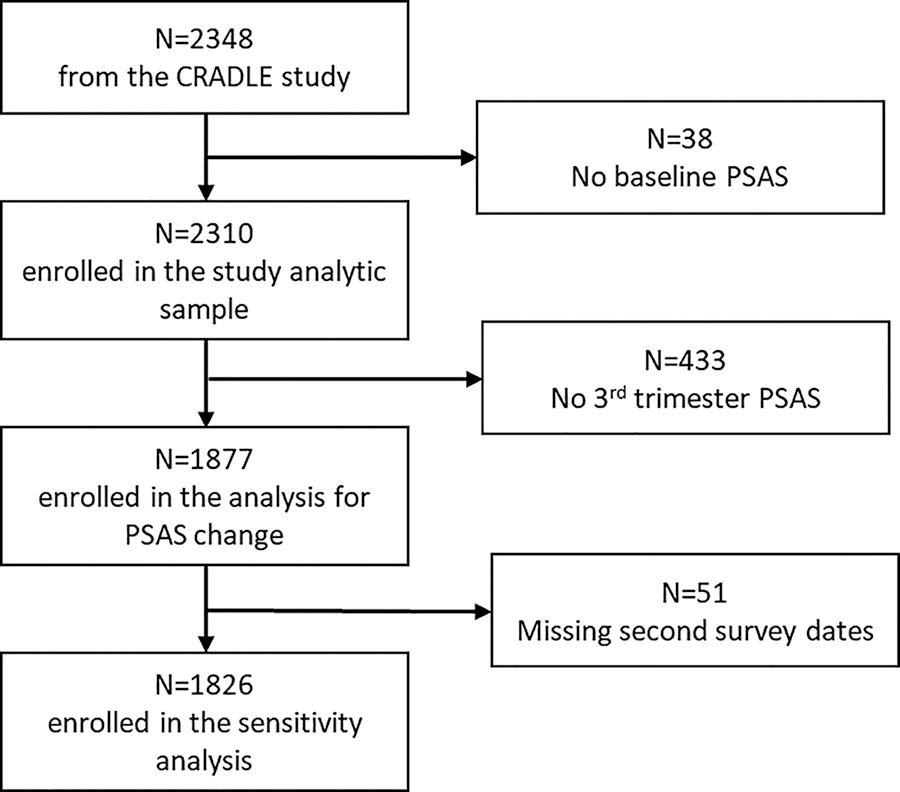
Flow chart for the study sample.
All statistical tests were two-tailed, and p values <0.05 were taken to indicate statistical significance. All the analyses were performed using SAS 9.4 software (SAS Institute, Inc., Cary, NC).
Results
Among all 2,310 pregnant participants (40.74% Black, 37.06% White, 20.91% Hispanic, and 1.29% other race and ethnicity), 154 (6.67%) developed GDM. The mean second trimester (baseline) PSAS was 9.33 (median = 9). The distribution of second trimester PSAS is shown in Figure 2.

Bar chart and boxplot for baseline Pregnancy-Specific Anxiety Scale (PSAS).
Compared with participants with low second trimester (baseline) anxiety, those with high anxiety were more likely to be of Black race, smoke tobacco and marijuana during pregnancy, be employed outside the home, and more likely to have higher education levels, lower household income, and less likely to be married (Table 1).
Baseline Characteristics of Participants According to Pregnancy-Specific Anxiety Scale Groups
PSAS, Pregnancy-Specific Anxiety Scale; SD, standard deviation.
Compared with participants with low second trimester (baseline) PSAS score, the OR of having GDM for participants with high PSAS was 0.99 (95% CI: 0.70–1.42) after adjusting for confounders. Among 1,877 participants with PSAS change data, 810 (43.15%) increased PSAS during pregnancy. The maximum PSAS increasing score was 16. Compared with participants with no change/decreased PSAS, participants with increased PSAS were 52% more likely to develop GDM (adjusted OR: 1.52, 95% CI: 1.04–2.23) (Table 2).
The Associations Between Pregnancy-Specific Anxiety Scale and Gestational Diabetes Mellitus
Adjusted for age, race, prenatal care type, marital status, education level, working status, household income, body mass index, and smoking, drinking, and marijuana use status after pregnancy.
CI, confidence interval; GDM, gestational diabetes mellitus; OR, odds ratio.
In our sensitivity analyses, we first divided the participants based on whether their glucose tolerance screenings were performed prior to their third trimester PSAS measurements. For those who had glucose tolerance screenings before third trimester PSAS measurements (n = 1,730), participants with increased PSAS were 54% more likely to develop GDM (adjusted OR: 1.54, 95% CI: 1.02–2.32). For those who had glucose tolerance screenings after the third trimester PSAS measurements (n = 96), increased PSAS was also associated with a greater risk of developing GDM (adjusted OR = 3.28, 95% CI: 0.49–21.99), although the association was not statistically significant, which is likely due to the small sample size (Fig. 3). On the other hand, when we excluded participants who had GDM screenings before 24 GW and were diagnosed with GDM (Supplementary Table S1), or divided the participants into four groups based on their second trimester and third trimester PSAS score, using 9 as the cut-off point (Supplementary Table S2), the results were similar to our main finding: increasing PSAS was associated with high odds of developing GDM.
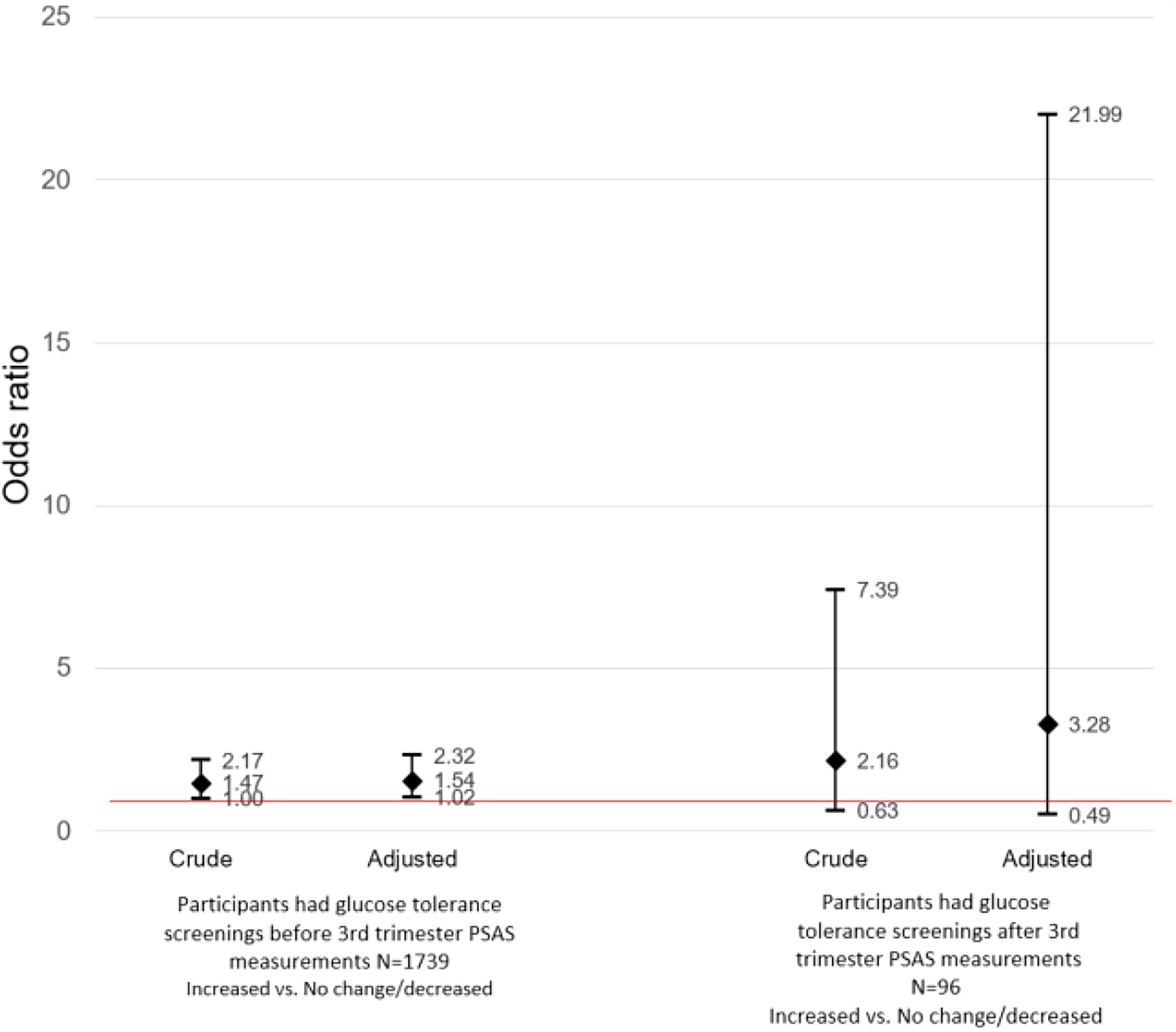
Sensitivity analysis based on participants’ glucose tolerance screenings prior to their third trimester PSAS measurements for the association between PSAS and gestational diabetes mellitus.
Discussion
In this large study of racially diverse pregnant individuals in the United States, we found participants with increasing pregnancy-specific anxiety had a 52% elevated risk of GDM compared with their counterparts with no change or decreasing anxiety.
Our results from a U.S. population are in the same line with the previous studies by Tang et al. among Chinese population and Thiele et al. among Canadians, 19 but not with a study in Australia conducted by Pathirana et al. 20 In Tang et al.’s study, they found that individuals experiencing anxiety symptoms during pregnancy had a higher incidence of GDM as compared with pregnant individuals without anxiety symptoms (OR = 1.56, 95% CI: 1.01–2.36). Compared with Tang’s study using Self-Rating Anxiety Scale, which measures general anxiety, 11 our study used PSAS, which was developed and validated specifically for pregnancy-specific anxiety. We acknowledged that there are different methods to measure pregnancy-specific anxiety, with each having its own advantages and limitations and was developed in various racial and ethnic groups and languages. 21 The PSAS that we applied in our study was developed and validated in the United States. 17 More importantly, as Tang’s study measured anxiety only one time during early pregnancy (i.e., 8–14 GW), our study measured PSAS twice, which enabled us to capture the anxiety levels in the middle and late phases of pregnancy. Although there is no defined minimum clinically important difference for PSAS, our study found a higher risk of GDM among those whose PSAS increased any level from the second to third trimesters. The results indicate the importance of monitoring pregnancy anxiety status change during pregnancy and emphasize the necessity of developing clinical criteria of minimum clinically important difference for PSAS. We believe that changes in the anxiety level during middle and late pregnancy can capture pregnancy-specific anxiety more accurately (compared with the baseline anxiety, which is inclined to reflect general anxiety) and is more likely to be a risk factor of pregnancy-related outcomes, such as GDM. Similar results were also observed in Thiele’s population-based retrospective cohort study using data from all singleton births in British Columbia, Canada. They reported higher odds of developing GDM among those diagnosed with antenatal depression or anxiety compared with their counterparts. 19 While the results of our study and their study were similar, our study specifically focused on pregnancy anxiety, without combining depression and anxiety as the exposure because anxiety and depression, despite having high rate of co-occurrence, are two distinct mental health conditions. 22 Our findings provide specific evidence for the potential adverse influence of pregnancy anxiety on GDM. Additionally, we used a questionnaire, rather than a clinical diagnosis, to measure pregnancy anxiety. This approach allowed us to monitor pregnancy anxiety in all participants, including those who may not have been clinically diagnosed with anxiety but still experienced high levels of pregnancy anxiety or vice versa. On the other hand, a recent prospective cohort study from a socioeconomically disadvantaged community in Australia conducted by Pathirana et al. did not observe an association between early gestation anxiety and GDM. 20 They measured antenatal anxiety in the first trimester using State and Trait Anxiety Score-6, a general anxiety questionnaire. As Pathirana et al.’s study only focused on socioeconomically disadvantaged populations, the different findings between Pathirana et al.’s study and our study might be a hint for the potential effect modification of socioeconomic status. Further studies about the role of socioeconomic status on the association between pregnancy anxiety and GDM are needed.
Although the mechanistic involvement of pregnancy-specific anxiety and GDM is still not fully understood, one possible mechanism for the linkage between pregnancy-specific anxiety and GDM may be due to the physiological responses of the hypothalamic–pituitary–adrenal (HPA) axis. 10,23 The release of both cortisol and arginine vasopressin is stimulated by anxiety. Cortisol and arginine vasopressin can antagonize insulin action, increase insulin resistance, and suppress insulin secretion in pancreatic beta cells, contributing to elevated blood glucose levels and potentially diabetes. 24,25 In addition, individuals with anxiety are more likely to increase an appetite and even increase the consumption for high-sugar and high-fat foods. These negative behavioral changes due to anxiety may also increase the risk of developing GDM. 25,26
The majority of our participants had their second PSAS measurements after GDM screenings, indicating that most of the participants knew their GDM status before their second PSAS measurements. This may raise the concern of reverse causality bias. However, in our sensitivity analysis based on whether participants’ glucose tolerance screenings prior to their third trimester PSAS measurements, we found positive associations between increasing PSAS and GDM risk no matter the timelines of GDM screenings and PSAS measurements. Interestingly, the effect size among those who had glucose tolerance screenings after their third trimester PSAS measurements (knew their GDM status after their third trimester PSAS measurements) was larger than the effect size among those who had glucose tolerance screenings before their third trimester PSAS measurements (knew their GDM status before their third trimester PSAS measurements). The point estimates among those who knew their GDM status before their third trimester PSAS measurements were significant. Although knowing the outcome (GDM) before full exposure measurement (PSAS change) may raise the issue of temporality for causal inference, the results still enhance the evidence for the “association” between pregnancy-specific anxiety and GDM risk. On the other hand, although the point estimates were not significant for those who knew their GDM status after their third trimester PSAS measurements due to the small sample size, a stronger effect size among this group may provide a hint for the hypothesis that pregnancy-specific anxiety could be a potential risk factor that leads to GDM. Further studies on the causal relationship between pregnancy-specific anxiety and the risk of GDM are warranted.
Conclusions
In conclusion, we observed a higher risk of GDM among pregnant individuals who increased their pregnancy-specific anxiety from second to third trimesters. Further studies regarding the mechanisms of anxiety on GDM are warranted to confirm our results.
Footnotes
Acknowledgments
The authors thank the research team in the Department of Obstetrics and Gynecology at Prisma Health for their dedication to the management and implementation of the study. We also thank Dr. Christine Dunkel-Schetter for providing suggestions for the abstract. We thank all the participants for participating in this clinical trial.
Access to Data and Data Analysis
The corresponding author had full access to all the data in the study, took responsibility for the integrity of the data and the accuracy of the data analysis, and had final responsibility for the decision to submit for publication.
Data Sharing
Deidentified study data will be available publicly on the NICHD/DASH Data and Specimen Hub (![]() ) in October 2026, five years after study completion. Prior to that time, researchers with a methodologically sound proposal can direct inquiries to
) in October 2026, five years after study completion. Prior to that time, researchers with a methodologically sound proposal can direct inquiries to
Ethics Statement
This study was jointly reviewed and approved by IRBs of the Greenville Health System, Clemson University, and University of California at Los Angeles, with IRB file number: Pro000043994. All the study participants signed a written consent form before they were enrolled in the study. The consenting form had been approved by the IRB of Greenville Health System.
Authors’ Contributions
L.C., C.-T.H., and S.S. designed the study. C.-T.H. drafted the article and analyzed the data. S.S. conducted a literature review. L.Z., J.B., and A.C. provided the major comments and edited the article. L.C., A.C., J.B., and L.Z. conducted the data collection and data cleaning. L.C. and A.C. obtained the funding and supervised the study. All authors revised and edited the article. All authors read and approved the final article.
Author Disclosure Statement
No potential conflicts of interest relevant to this article were reported.
Funding Information
Research reported in this publication was supported by the U.S. Department of Health and Human Services through the National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health, and Human Development under award number
Supplementary Material
Supplementary Tables S1
Supplementary Tables S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.