
Abstract
Background:
Human papillomavirus (HPV) vaccination during the postpartum period is an opportunity for vaccine eligible individuals to be vaccinated.
Objective:
Identify predictors of vaccine acceptance in the postpartum period among patients aged 18–26.
Study Design:
A retrospective chart review was conducted to evaluate the rate of HPV vaccination to eligible postpartum patients aged 18–26 who delivered between January 2021 and May 2023 at our institution. Clinical and demographic data were extracted. Comparisons were made between fully vaccinated individuals and those who were unvaccinated or incompletely vaccinated. Variables significantly associated with vaccination status or acceptance were included in a multivariable logistic regression model.
Results:
Of the 1,130 patients who met the study inclusion criteria, 42.1% were eligible for postpartum HPV vaccination. The average age was 23 years, the majority White (74.5%), and English speaking (93.1%). Nineteen percent of eligible patients accepted HPV vaccination, with differences between those who accepted or declined the vaccine identified in: preferred language, tobacco use, delivering provider’s specialty, and receiving any vaccination during pregnancy. Spanish-speaking patients had >5× the odds of accepting the vaccine compared with English-speaking patients. Smokers, patients delivered by a family medicine provider, and those who accepted any vaccine during pregnancy had more than twice the odds of receiving the vaccine postpartum.
Conclusion(s):
The postpartum period remains an opportunity to provide HPV vaccination. Our study identified patients less likely to be vaccinated prior to delivery, as well as patients who are more likely to accept vaccinations postpartum.
Introduction
Human papillomavirus (HPV) is the most common sexually transmitted infection and is associated with six different types of cancer. 1 Cervical cancer is the fourth most common cancer in women globally, with over 90% of cases directly associated with persistent infection with high-risk HPV types. 2,3 The HPV vaccine was Food and Drug Administration (FDA) approved in 2006 and is highly efficacious in reducing the incidence of cervical precancerous lesions and cervical cancer. 4 –6 It is currently FDA approved for all genders between the ages of 9–45, and the Advisory Committee on Immunization Practices (ACIP) recommend routine immunization at age 11 or 12 years. 7 –9
Vaccine uptake remains low in the United States, with only 38.6% of individuals ages 9–17 years receiving one or more vaccine doses. 10 Only 21.5% of adults aged 18–26 years had received the recommended number of doses of the vaccine in 2018. 11 To achieve the Healthy People 2030 goal of 80% vaccination completion, increased efforts to encourage adolescent vaccination and catch-up immunization among young adults are warranted.
Pregnant people have been identified as a high-risk population with low rates of vaccination. 12,13 Among cohorts of pregnant patients 18–26 years of age, only 7.5–15.5% of individuals were identified as having been vaccinated against HPV prior to delivery. 12,13 The postpartum period has been suggested as an ideal opportunity to increase HPV vaccination as pregnancy is associated with improved health care continuity and normalization of other routine vaccinations. 14,15 Qualitative studies have demonstrated that patients view postpartum vaccination favorably with high rates of patient acceptance and satisfaction following inpatient vaccination. 16 –18 Nonetheless, prior studies assessing postpartum vaccination programs have reported variable uptake among eligible patients, ranging from 23% to 97%. 12,19 –22 A recent retrospective study of ∼570 postpartum patients examining the outcomes of their routine postpartum vaccination program found that ∼23% of eligible individuals received an inpatient HPV vaccine. 21 This study demonstrated increased rates of vaccine acceptance among Hispanic, Spanish-speaking, and publicly insured individuals, with receipt of care from a certified midwife remaining the only significant predictor of vaccination after adjustment for covariates.
In 2021, our institution introduced a postpartum vaccination quality initiative into routine care to offer HPV immunization for individuals who have not started or completed the series. Existing literature remains limited by the wide range of vaccine uptake, small sample sizes, and resource-intensive program designs such as need for study coordinators or follow-up reminders for vaccines. Additionally, few studies capture a comprehensive list of potential predictors of vaccination which may help inform targeted interventions to increase routine uptake. Our institution averages approximately 2,500 deliveries annually; thus, our quality improvement initiative and data analysis may provide important additional data to bolster understanding of predictors of HPV vaccination. In this study, we sought to evaluate the impact of our HPV vaccination program, present HPV vaccination results for patients in our sample, and identify predictors of vaccine acceptance in the postpartum period among patients aged 18–26.
Materials and Methods
We conducted a retrospective chart review to evaluate the rates of HPV vaccination to eligible postpartum patients aged 18–26 who delivered between January 2021, at the start of our quality improvement initiative, and May 2023 at our institution. Patients older than 26 years were excluded from this study in accordance with the ACIP guidelines for HPV vaccination. This study was determined to be exempt by the Oregon Health and Science University Institutional Review Board.
Quality improvement initiative
Our quality improvement initiative began in 2021 by obstetrics and gynecology (OBGYN) residents. Patients cared for by certified nurse midwife (CNM) or family medicine physicians were not included in this initiative. All pregnant patients are screened for HPV vaccination status and number of prior vaccinations during their initial prenatal visit. The patient is screened again when admitted to the labor and delivery floor, as well as postpartum. Those who have never been vaccinated or are incompletely vaccinated are educated about the vaccine by a health care provider and offered the HPV (9-valent) vaccine in the inpatient setting prior to discharge. They are also scheduled for nursing visits for subsequent vaccinations to complete their vaccination series if needed.
Data collection
Data extracted from the electronic medical record (EMR) included the following: demographic information, health history data, HPV vaccination history, pregnancy/delivery outcomes, and HPV vaccination during the inpatient postpartum stay. Demographic data are routinely collected via patient self-report to clinical staff and documented within their EMR. Data were extracted using structured query language server queries against the Epic enterprise data warehouse database.
Statistical analysis
Patients were first grouped by their vaccination status prior to delivery. These groups were defined as patients who had already completed the HPV vaccination series, those who never started the series, and those who started but did not complete the vaccine series. Demographic and clinical characteristics were compared between vaccination groups. Additionally, vaccine-eligible patients (those who had never received HPV vaccination or had an incomplete vaccination series) were further grouped by whether or not they received HPV vaccination postpartum. Categorical variables were compared across groups using Chi-squared or Fisher’s exact tests, and continuous variables were compared using analysis of variance or t-tests. Following initial comparisons, variables found to have a significant association with vaccination status or acceptance (p-value <0.05) were included in a multivariable logistic regression model. Odds ratios and their 95% confidence intervals are presented in odds ratio plots.
Vaccine acceptance rates were computed quarterly and plotted to check for a temporal pattern in vaccine acceptance since the initiative’s implementation. All analyses were performed and visualizations generated using R Statistical Software. 23
Results
Initial analysis included the patient population prior to delivery. A total of 1,130 patients were included in data collection and met the inclusion criteria for study analysis. Of these, 654 (58%) patients completed the HPV vaccination series prior to delivery, 370 (33%) patients never started the HPV vaccination series before delivery, and 106 (9%) patients started but did not complete the HPV vaccination series before delivery.
The patient demographic and clinical characteristics of all patients are presented in Table 1. The average age of patients was 23 years, and most were White (74.5%), English speaking (93.1%), partnered (50.5%), and nonsmokers (88.4%). Significant associations with predelivery HPV vaccination status were noted for the following independent variables: age, race, preferred language, marital status, tobacco use, having a primary care provider (PCP), parity status, and receipt of a vaccine during pregnancy (including Tdap, Flu, or COVID-19 vaccine).
Comparing Characteristics of Patients by HPV Vaccination Status Before Delivery
p-values from Chi-square, Fisher’s exact test (used when any cell count is <5), and ANOVA.
ANOVA, analysis of variance; HPV, human papillomavirus; NICU, neonatal intensive care unit.
Multivariable logistic regression was performed to explore factors related to predelivery vaccine status (Fig. 1). For this analysis, all vaccine-eligible patients (including those who had never received an HPV vaccination and those with a partially complete series) were compared with those with complete HPV vaccination prior to delivery. Variables found to be significantly associated with vaccination (p-value <0.05) were included as in the model. For every one-year increase in a patient’s age, the odds of a patient being fully vaccinated against HPV decrease by 12%. Compared with White patients, Native Hawaiian/Pacific Islander patients are less likely to have completed the vaccine series prior to delivery. Spanish-speaking patients have 6% the odds of being fully vaccinated compared with English-speaking patients. Single patients have nearly twice the odds of vaccine completion compared with married/partnered patients. Patients with a primary care provider have more than twice the odds of having completed the vaccine series compared with those without a primary care provider. Patients who received a Tdap, Flu, or COVID-19 vaccine in this pregnancy had greater odds of having already completed the vaccine series compared with patients who did not accept vaccines.
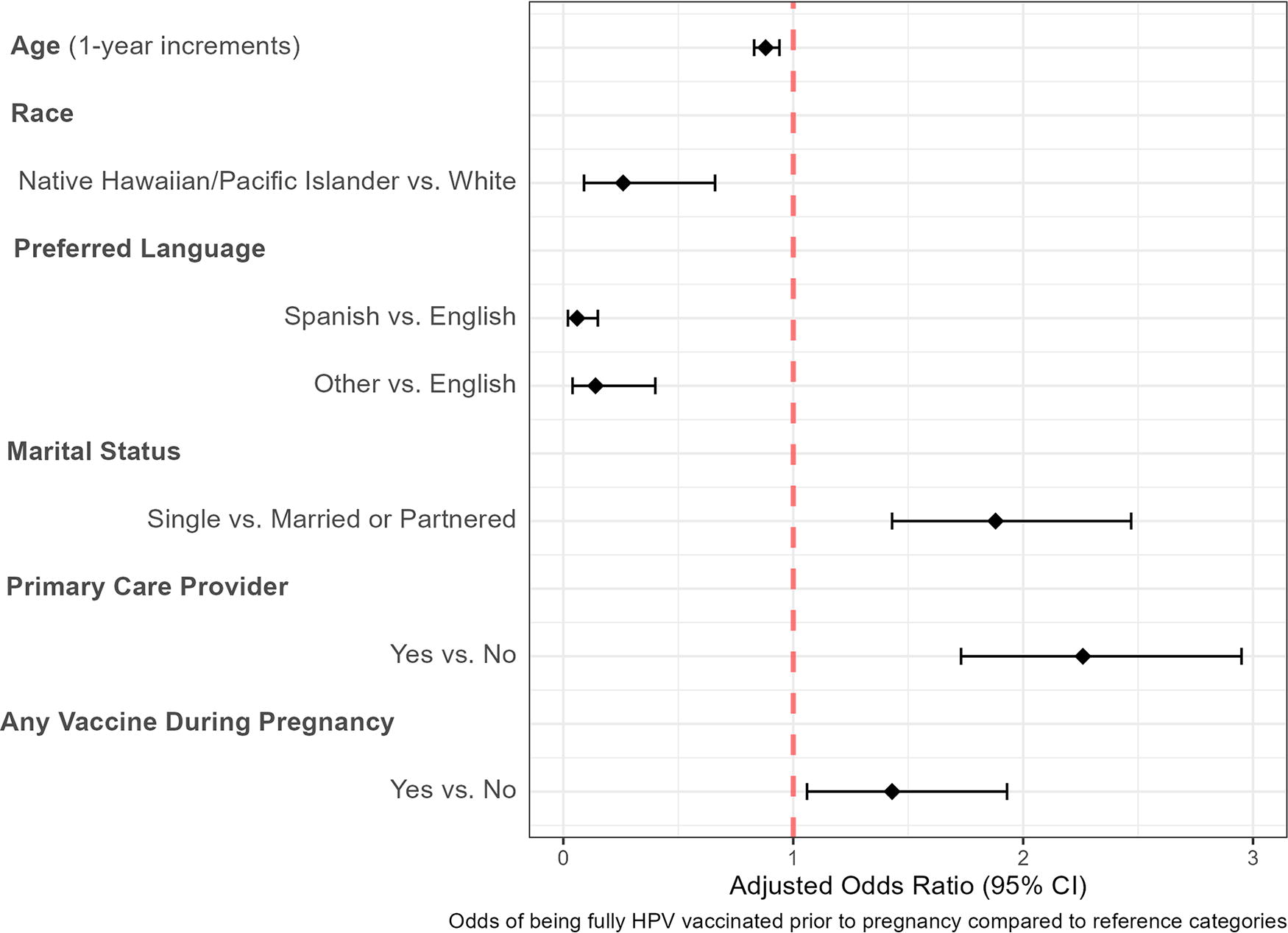
Multivariable analysis between vaccination groups before delivery. Odds ratio plot reviewing odds of being fully vaccinated prior to pregnancy compared to reference groups. Variables included revealed statistically significant difference in being fully vaccinated.
Analysis was then done for vaccine-eligible patients postdelivery. Of the 1,130 patients who were included in this study, 476 (42.1%) were eligible for postpartum HPV vaccination (Table 2). These included patients who had never started the vaccination series and those who started but did not complete the series prior to delivery. Of these eligible patients, 382 patients (81%) declined HPV vaccination postpartum, and 94 (19%) received HPV vaccination postpartum. Of those who received the HPV vaccination postpartum, 69 (73.4%) of these patients had not previously started the HPV vaccination series. Significant differences between these groups were seen in the following independent variables: preferred language, tobacco use, specialty of the delivering provider, and receipt of any vaccination in this pregnancy.
Comparing Characteristics of HPV Vaccine-Eligible Patients by Uptake of Postpartum HPV Vaccination
p-values from Chi-square, Fisher’s exact test (used when any cell count is <5), and Welch’s t-test.
HPV, human papillomavirus; NICU, neonatal intensive care unit.
Multivariable logistic regression analysis was performed using the independent variables that revealed significant difference between the groups who received versus did not receive the HPV vaccination postpartum (Fig. 2). Spanish-speaking patients had more than 5 times the odds of accepting the HPV vaccination postpartum compared with English-speaking patients; however, confidence intervals were wide (2.50–11.27). Smokers and former smokers had more than twice the odds of accepting the HPV vaccination postpartum compared with people who had never smoked. Patients had greater odds of receiving HPV vaccination postpartum if they were delivered by a family medicine provider compared with OBGYN providers, whereas those delivered by CNMs had lower odds of vaccine receipt. Patients who received any vaccination during pregnancy (including COVID-19, influenza, and Tdap vaccination) had more than twice the odds of receiving the HPV vaccination postpartum compared with patients who did not accept vaccines in pregnancy.
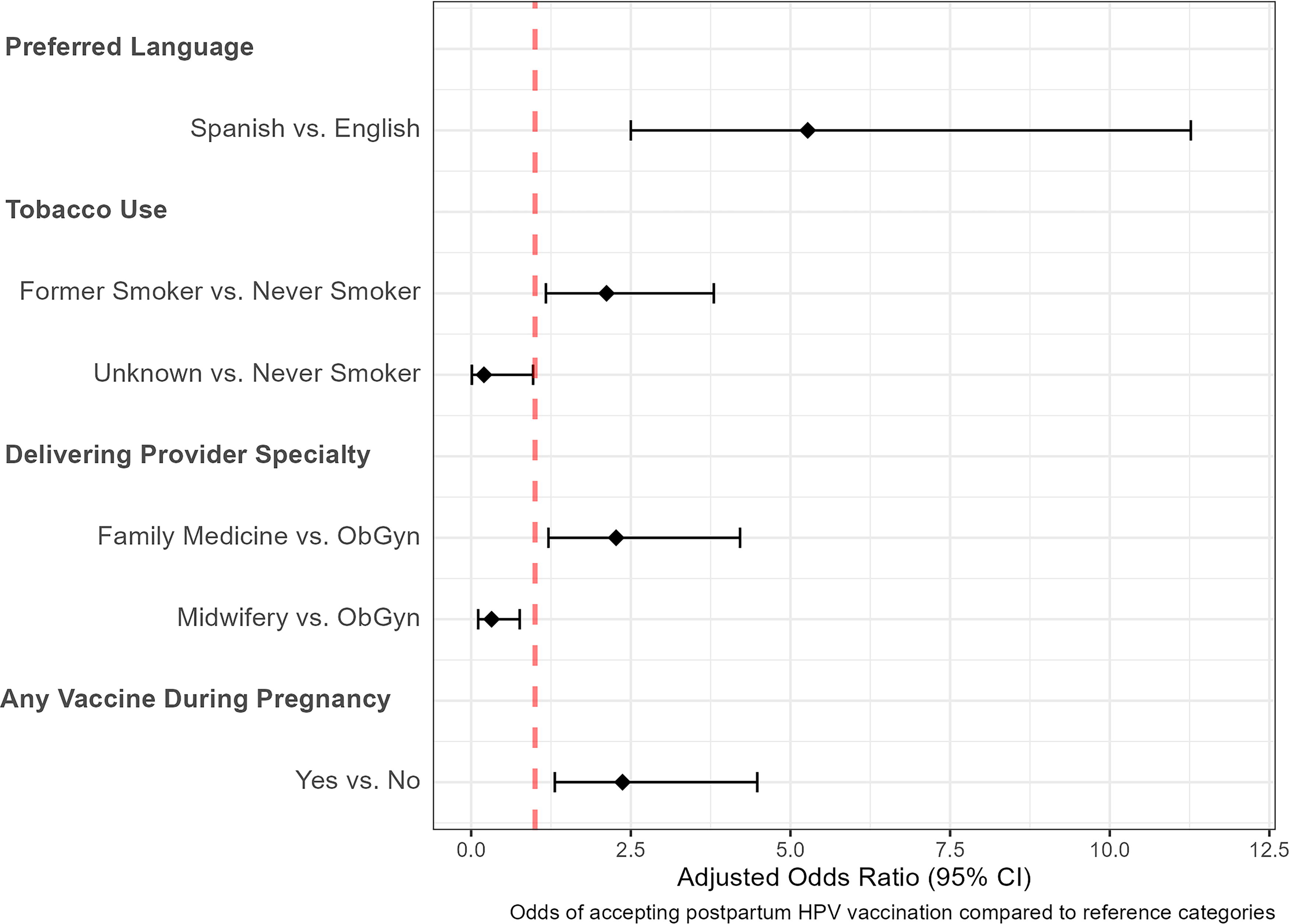
Multivariable analysis between groups by Uptake of Postpartum HPV Vaccination. Odds ratio plot reviewing odds of receiving vaccination after delivery compared to reference groups. Variables depicted had statistically significant difference in being vaccinated postpartum.
Figure 3 shows the quarterly proportion of patients accepting the HPV vaccination postpartum since the start of the quality improvement initiative. The acceptance rate at the start of the initiative in early 2021 was 21.1%, with fluctuation over the study period. Specifically, vaccine acceptance was highest in Q2 of 2021 (36.4%) and lowest in Q1 of 2023 (10.7%). During the study period, vaccine acceptance appeared to fluctuate seasonally, with higher rates of acceptance seen during Quarters 2 and 4 of each year. Overall, there was a slight decrease in vaccine acceptance over the study period, indicating potential implementation fatigue.
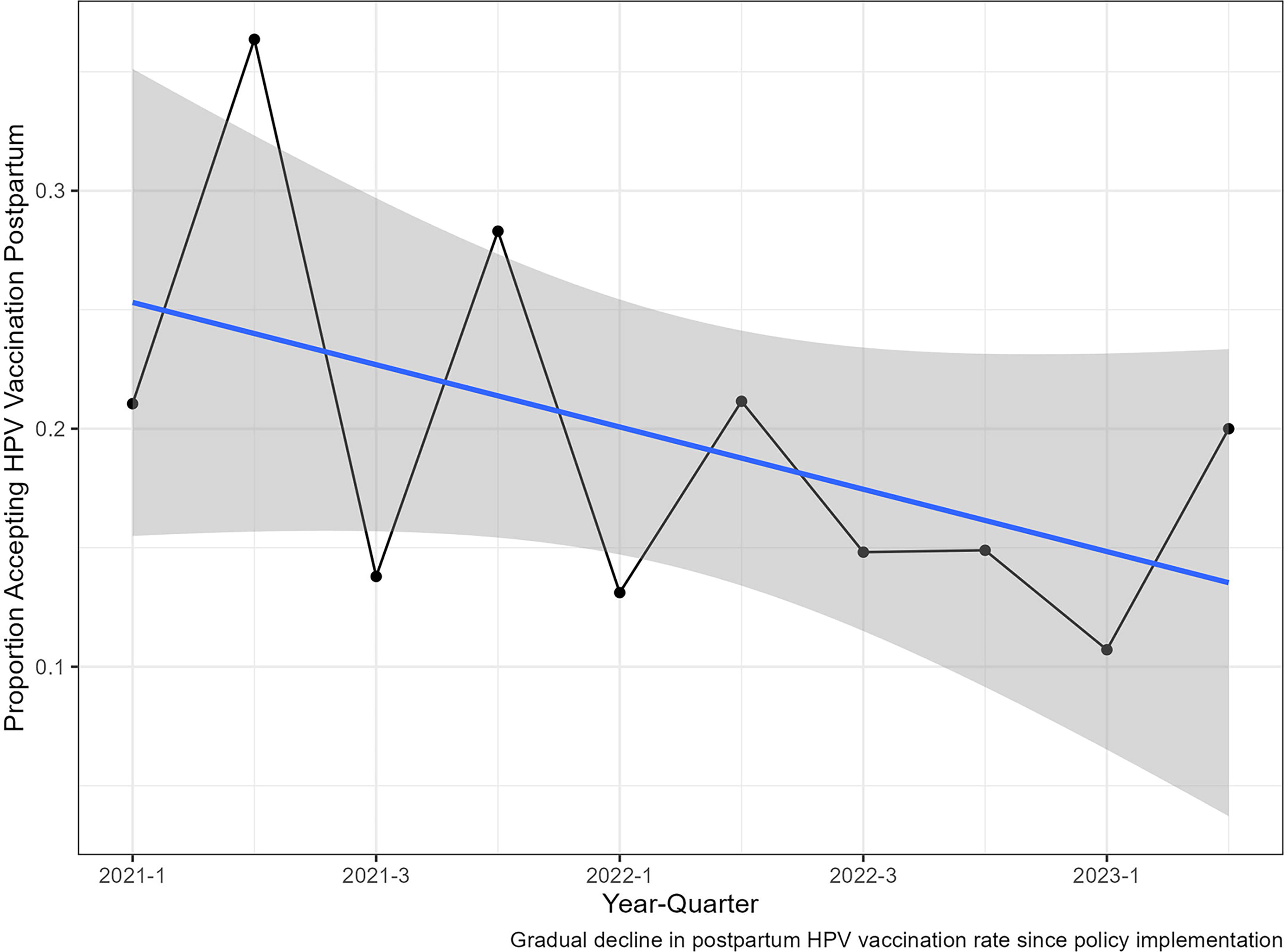
Rate of postpartum HPV vaccination rates per quarter-year. Line graph of vaccine acceptance by quarter, including a linear regression line of best fit with shaded confidence bands. HPV, human papillomavirus.
Discussion
Principal findings
Our study sought to evaluate the impact of our HPV vaccination quality improvement initiative and identify predictors of vaccine acceptance in the postpartum period among patients aged 18–26. Approximately one-fifth of patients who were eligible for the HPV vaccination received at least one vaccination during our study period. We also were able to identify several patterns predictive of receiving and not receiving the vaccination.
Results in the context of what is known
We first sought to understand the predictors of being fully vaccinated, partially vaccinated, or unvaccinated prior to delivery. Compared with White individuals, Native Hawaiian/Pacific Islander individuals were less likely to have been vaccinated. This is consistent with previous literature. 24 –26 Native Hawaiian and Pacific Islander individuals aged 18–24 years had HPV vaccination initiation and completion rates of 17.6% and 7.9%, respectively. 27
Our study adds to the existing literature on postpartum HPV vaccination programs, as summarized in Table 3. Previous research has shown that implementing postpartum vaccination programs leads to an overall increase in HPV vaccine uptake. However, a closer examination of these studies reveals a considerable variation in vaccine uptake rates, from 23.1% to 97.2%, along with varying program designs. The programs that achieved the highest rates of vaccine uptake (67.3–97.2%) employed more resource-intensive strategies, such as dedicated patient coordinators and robust patient reminder systems. 12,19,20 Conversely, initiatives that integrated inpatient postpartum HPV vaccination into routine care or utilized electronic health record prompts reported lower vaccine uptake rates (ranging from 23.1% to 26.5%). 21,22
Summary of Results from Existing Literature
CNM, certified nurse midwife; EMR, electronic medical record; HPV, human papillomavirus; PP, postpartum; L&D, labor and delivery
A similar postpartum vaccination program at a large academic institution was done in 2021. Their intervention included vaccine eligibility confirmation through EMR review on admission to the hospital, vaccine order by postpartum rounding health care provider with subsequent doses ordered outpatient, and update to the patient’s EMR for need for additional vaccinations. They included 569 patients, and their intervention resulted in a vaccine uptake rate of 23.1% among postpartum individuals. 21 Similarly, our study included 1,130 individuals and utilized screening for vaccine eligibility at prenatal visits, admission, and postpartum rounding via EMR review, ordering of vaccine by rounding providers, and scheduling for nursing visits for subsequent vaccine doses. Our intervention demonstrated similar vaccination rates. Altogether, these varying results suggest the role of program design and resource allocation in influencing the degree of postpartum HPV vaccination rates.
Clinical and research implications
In our quality initiative, we found that the following variables were associated with receiving the vaccination postpartum: Spanish-speaking, former smoker, delivery by family medicine provider, and receiving of any other vaccine during pregnancy (e.g., Tdap, influenza, COVID-19). Although non-English-speaking patients were less likely to be vaccinated prior to delivery, they were 5 times more likely to have received the vaccine in the postpartum period compared with English-speaking patients. This may be due to difficulty accessing and receiving high quality health care due to a language barrier. 29,30 However, with hospital birth and inpatient postpartum care, this population that may not routinely have access to health care could receive medical care during their inpatient admission. Our quality initiative was able to successfully target this vaccine-eligible population.
Patients who were former smokers were more than twice as likely to accept the vaccine postpartum compared with never smokers. Guo et al. found that former and never smokers were more likely to have been vaccinated compared with current smokers among adult women aged 20–26 years. 31 Smoking is a well-known cofactor for cervical cancer and HPV mediated precancerous lesions. 32 This finding reveals that an inpatient vaccine catch-up initiative can help to target the patient population at higher risk of developing HPV-mediated diseases.
Patients delivered by a family medicine provider were more than twice as likely to receive the vaccine postpartum compared with patients delivered by OBGYN providers. Unlike OBGYN providers, who often focus on fragmented periods of an individual’s life, family medicine encompasses care of individuals from the “cradle to grave.” Additionally, immunization schedules are a large part of family medicine practice and less of a focus in the OBGYN specialty. Adopting a stronger prevention focused model within the OBGYN specialty to mirror the family medicine specialty may help to increase the success of an HPV vaccination program run by OBGYN providers. Patients delivered by the CNM service had nearly 70% lower odds of receiving the vaccine compared with patients delivered by an OBGYN provider. However, CNM patients were not included in this quality improvement initiative. At our institution, CNM patients make up more than 15% of our deliveries. Thus, there is potential to reach more patients if we expand our program to include CNM providers in ongoing future initiatives.
Patients who accepted vaccines during the current pregnancy (i.e., influenza, Tdap, and COVID-19) were more likely to accept the HPV vaccine postpartum. A UK study investigating the acceptability of antenatal vaccination among patients and providers’ confidence in vaccine recommendations found that the most cited reason for declining antenatal vaccination was concern regarding possible side effects for the fetus and doubts regarding efficacy and necessity of immunization.33 Similar reasons may continue into the postnatal period, such as possible side effects with lactation or doubts in efficacy and necessity. Thus, continued discussion through regular prenatal visits may be a way to address vaccine hesitancy in this population.
Finally, as suspected, intervention fatigue and rates of vaccination declined with time since the start of our intervention in 2021. Currently, this HPV vaccination initiative is run exclusively by OBGYN residents, who have broad responsibilities on the labor and delivery floor. Although postpartum vaccination remains a very important opportunity to increase rates of vaccination, these data are helpful to highlight the need for more sustainable strategies to continue this work. In our program’s current protocol, postpartum nursing staff provide education regarding the MMR (measles, mumps, and rubella) and varicella vaccinations for patients who were deemed nonimmune during their prenatal care. The addition of HPV vaccination to this already-established workflow may be an option to raise the vaccination rates.
Strengths and limitations
Our study does have several strengths. We were able to review the effectiveness of an EMR-based HPV vaccination catch-up initiative at a large academic institution. Our study has the largest sample size in current literature that analyzes the impact of postpartum HPV vaccination. Our study reviewed a large number of variables that may be predictive of vaccine status before and after delivery.
Our study had several limitations. First, our study only included data from a single institution in the Pacific Northwest; thus, it may not be generalizable. Second, we reviewed data across different delivery provider groups, all of whom had different protocols for postpartum patients. Third, this was a retrospective review in which we only reviewed whether patients received or did not receive the HPV vaccination postpartum. We were unable to determine the reasons for why a patient may have accepted or declined a vaccination. Finally, we were unable to further stratify our data of those who completed any additional HPV vaccinations outside of the postpartum inpatient stay and do not have data on vaccine eligible patients who needed to complete the full series outpatient.
Conclusion
Our study shows that 57% of individuals are fully vaccinated before pregnancy, which is less than the CDC Healthy People 2030 goal of 80%. The postpartum period is an opportunity to increase vaccination rates. There have now been two large recent national studies, including ours, that have shown that an HPV vaccination program can achieve an ∼20% vaccination rate in the postpartum setting when using a low-cost, EMR-based intervention. However, this vaccination rate can be increased by providing additional resources such as patient navigators and coordinators who ensure patient follow-up. Our study also revealed risk factors for being incompletely vaccinated before pregnancy and those who are less likely to receive the vaccine postpartum. The fourth trimester is a busy period for many individuals as there are frequent health care visits for lactation consultation and pediatric appointments for the baby; synergizing with these health care providers may help increase HPV vaccination uptake in the broader postpartum period. Future directions will include a prospective mixed methods study to further evaluate the barriers and facilitators to HPV vaccination in the postpartum period.
Footnotes
Acknowledgment
The authors thank Steve Huke (Oregon Health Science University) for his support in collecting and cleaning the data.
Authors’ Contributions
C.G.T.N.: Conceptualization, methodology, investigation, writing—original draft, and project administration. A.M.: Investigation, writing—original draft, and visualization. L.W.: Formal analysis, investigation, data curation, writing—reviewing and editing, and visualization. K.B.: Writing—reviewing and editing. J.C.: Writing—reviewing and editing. K.Y.: Writing—reviewing and editing. A.S.B.: Writing—reviewing and editing and supervision.
Author Disclosure Statement
All authors have no conflicts of interest to disclose.
Funding Information
This study received no funding to disclose.