
Abstract
Introduction:
Since 2021, state legislative restrictions like Texas Senate Bill 8 (SB8), followed by the U.S. Supreme Court Dobbs v. Jackson Women’s Health Organization (Dobbs) decision, led to a surge of people traveling for abortion care. This study sought to describe the association between changing abortion legislation and appointment wait times for New Mexico residents at the University of New Mexico Center for Reproductive Health (CRH).
Methods:
We performed a retrospective chart review of New Mexico residents scheduling first-trimester abortion appointments at CRH. We compared the time from the initial scheduling call to initial appointment date (wait time) over three periods: pre-SB8 (2020), post-SB8 pre-Dobbs (2021), and post-Dobbs (2022).
Results:
After the Dobbs decision, New Mexico residents waited two weeks longer for abortion appointments and called for appointments over a week earlier in pregnancy on average than in the two previous years. Median wait times for appointments were 5.0 days (interquartile range [IQR]: 4.0) pre-SB8, 4.5 days (IQR: 5.0) post-SB8, and 23.0 days (IQR: 18.0) post-Dobbs.
Conclusion:
New Mexicans encountered a significant increase in first-trimester abortion appointment wait times after the Dobbs decision. This study highlights the importance of maintaining abortion access for state residents during an influx of out-of-state patients. This increase in wait time is especially disruptive in rural and underserved states where residents face significant baseline barriers to medical care.
Introduction
Abortion access in states surrounding New Mexico—a state with few abortion restrictions—has changed dramatically since 2021. After Texas Senate Bill 8 (SB8) was enacted in September 2021, banning abortion after 6 weeks gestation, the number of Texans traveling out of state to obtain abortion care skyrocketed. 1 Immediately after SB8, Oklahoma and New Mexico accepted the largest share of Texas residents traveling for abortions. 1 In May 2022, Oklahoma’s governor signed a law banning abortion outright, eliminating Oklahoma as an access point and increasing the distance Texas residents had to travel to obtain care. 2,3 In June 2022, the U.S. Supreme Court decision in Dobbs v. Jackson Women’s Health Organization (Dobbs) overturned Roe v. Wade; abortion policies and reproductive rights reverted to the states.
In 2021, New Mexico proactively repealed an unenforced 1969 abortion ban to ensure it could not be implemented if Roe were overturned. 4 After Dobbs, many states, including Arizona and Oklahoma, increased abortion restrictions through new and existing laws, while others like New Mexico passed additional protections. 5 These actions solidified New Mexico’s status as a haven state for abortion care; the New Mexico abortion surge after several neighboring states banned abortion was unsurprising. 1
Even with safeguards, obtaining abortion care is challenging for many New Mexico residents. Factors influencing access to care include rural location, poverty, lack of access to insurance, and racial disparities. Rural communities make up two-thirds of New Mexico counties, and 18% of the population lives in poverty; 10.5% are uninsured. 6,7 Poor health outcomes are more common in New Mexico’s diverse communities. 8 Abortion care is not available in over 90% of New Mexico counties, leaving large parts of the state as abortion deserts. 9 Greater distance from an abortion facility is associated with delays in or inability to obtain care. 5
In 2014, three-quarters of people were able to access abortion within one week of calling to make an appointment. 10 Abortion appointment wait time is an important indicator of abortion access. All else being equal, people with shorter wait times can obtain abortions at earlier gestations. These burdens are disproportionately felt by systemically oppressed groups. 11 Abortion beyond the first trimester is not as easily accessible: fewer health centers provide this care, and the logistical and monetary burdens of travel, time off work, and childcare are increased. 12 For all these reasons, timely access to abortion is critical.
This study’s aim was to describe the immediate effects of changing abortion legislation and abortion appointment wait times for New Mexico residents at the University of New Mexico (UNM) Center for Reproductive Health (CRH) in Albuquerque, New Mexico. Additionally, we sought to describe any differences in the gestational duration (GD) at which New Mexicans called to schedule abortion appointments before and after SB8 and Dobbs.
Materials and Methods
Setting and subjects
This retrospective chart review identified New Mexico residents who scheduled abortion appointments in the first trimester at CRH. We excluded those who believed they were beyond 12 weeks GD at the time of their scheduled appointment, those who made appointments for care other than abortion, those whose abortion occurred outside of CRH, and those who were incarcerated or wards of the state. This study was approved by the UNM Human Research Review Committee Institutional Review Board (#23-094).
Study design
The primary study outcome was days of wait time from the initial appointment scheduling call to the initial scheduled appointment date at CRH. Secondary outcomes included GD at which New Mexico residents called to schedule an abortion appointment. We compared three time periods: the 5 months before SB8 (July through November 2020, pre-SB8); the 3 months following the SB8 decision but before Dobbs (September through November 2021, post-SB8); and the 3 months following the Dobbs decision (July through September 2022, post-Dobbs) (Fig. 1). We collected pre-SB8 data from a 5-month period to account for CRH’s baseline relatively low abortion volume during that time, to account for some of the seasonal variation in abortion volume, and to include similar comparison months for the post-SB8 and post-Dobbs groups. We focused on the first 3 months after legislative change to describe the immediate effects on wait time following legislative changes.
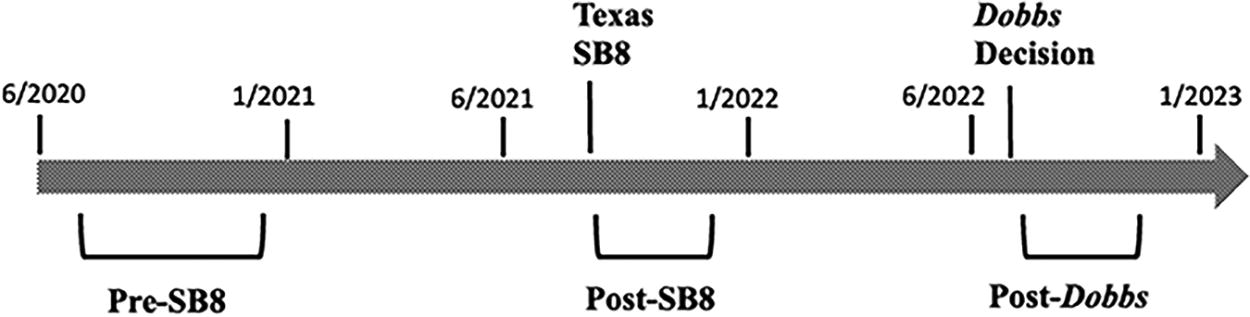
Three data collection periods (pre-SB8, post-SB8, and post-Dobbs) in relation to abortion restrictions. Three time periods were compared: before SB8 (July through November 2020, pre-SB8); after SB8 but before Dobbs (September through November 2021, post-SB8); and after Dobbs (July through September 2022, post-Dobbs). Dobbs, Dobbs v. Jackson Women’s Health Organization; SB8, Texas Senate Bill 8.
Pre-SB8, next-day abortion appointments were typically available at CRH; however, patients reported wait times up to 2 weeks post-SB8 and up to 8 weeks post-Dobbs. For a one-way analysis of variance test with three planned equal-sized groups of n = 50 each, G*Power 3.1.9.6 software indicated that 80% power with α = 0.05 would require a critical effect size of f = 0.256 or larger. Here, f is the ratio between the standard deviation (SD) of the group means, and the common within-group SD. Given our experience indicating very large between-groups variation assuming pre-SB8, post-SB8, and post-Dobbs averages near 2, 14, and 56 days, we estimated a group-means SD of approximately 28 days. With this very large between-groups variation, the planned sample size of n = 150 would be sufficient for the targeted power even if the within-groups variation was implausibly large at up to SD = 109 days (28/109 = 0.256).
Data collection
We used appointment scheduling software and the electronic medical record to identify scheduled abortion appointments for New Mexico residents; we then used quota sampling to select charts to review. We sampled 1–3 records per day of New Mexico residents who scheduled abortion appointments, regardless of appointment attendance. We sampled only first-trimester abortion appointments because CRH made minimal changes to first-trimester scheduling guidelines over the study period. Four chart reviewers (M.M., R.B., B.S., and V.T.) abstracted scheduling, demographic, and GD information from the electronic medical record. We also collected date of initial scheduling call, date of first scheduled appointment, attendance at the appointment, date of rescheduling call, and rescheduled appointment if applicable. We collected information on GD as follows: scheduler-documented GD based on last menstrual period (LMP) at the scheduling call and ultrasound-determined GD at the appointment. All de-identified data were entered into REDCap electronic data capture tool hosted at UNM.
Data analysis
We defined wait time as the time in days from initial appointment scheduling call to the initial scheduled appointment date. We assessed the following variables for confounding: insurance status, race, ethnicity, preferred language, employment, age at time of procedure, number of prior pregnancies, number of prior births, number of prior abortions, ultrasound-based GD, and rural versus urban county of residence based on metropolitan statistical area designation. We handled missing data by exclusion. We considered α = 0.05 statistically significant. We used Chi-square to compare demographic data and Cox regression analysis to assess differences in wait time between periods. We compared GD differences with Kruskal–Wallis and Wilcoxon’s matched-pairs signed-ranks tests as appropriate. We used Stata/SE 17.0 to conduct all data analysis.
Results
Demographic characteristics were similar, with the exception of rural versus urban county of residency, which was significant at p < 0.05 across the three time periods (Table 1) and roughly corresponded to state-level demographics for New Mexico. Of the 150 charts reviewed, the median age was 26; the majority (58%) identified as White Hispanic. Most patients were publicly insured (52%) or self-pay (37%). 44% had a prior birth, and 36% had a prior abortion. Most (93%) spoke English, and 36% were employed full time (all p > 0.05 across periods).
Demographic Characteristics of New Mexico Residents Scheduling Abortion Appointments over 3 Time Periods
Dobbs, Dobbs v. Jackson Women’s Health Organization; SB8, Texas Senate Bill 8.
Median wait times for a scheduled first-trimester abortion appointment were 5.0 days (interquartile range [IQR]: 4.0) pre-SB8, 4.5 days (IQR: 5.0) post-SB8, and 23.0 days (IQR: 18.0) post-Dobbs; p < 0.05 (Fig. 2). Wait times ranged from 0 to 17 days pre-SB8, 0 to 17 days post-SB8, and 0 to 38 days post-Dobbs. After multivariate analysis, these results remained significant after adjusting for ultrasound-based GD (Table 2, Fig. 2). All other potential confounding factors were not significant in the multivariate analysis and were not used in the final model.

Wait time from scheduling call to appointment. Median wait times (in days) for a scheduled first-trimester abortion appointment were 5.0 days (interquartile range [IQR]: 4.0) pre-SB8, 4.5 days (IQR: 5.0) post-SB8, and 23.0 days (IQR: 18.0) post-Dobbs; p < 0.05. IQR, interquartile range.
Wait Time from Call to Appointment Modeling Unadjusted and Adjusted for Ultrasound-Based Gestational Duration
The proportion of New Mexico residents who attended their scheduled abortion appointment (70–75%) was similar across time periods (Table 3; p = 0.84).
Abortion Appointment Attendance
After Dobbs, median GD by reported last menstrual period (LMP) at the time of initial appointment scheduling call was 36.8 (IQR: 19.2) days, compared with 46.0 (IQR: 15.6) days pre-SB8 and 47.1 (IQR: 18.1) days post-SB8; p < 0.05. GD by reported LMP on the appointment date was not significantly different from GD found by ultrasound at any period (pre-SB8 median 49.4 [IQR: 2 18.6] days by LMP versus 49.4 [IQR: 15.4] days by ultrasound; post-SB8 median 50.1 [IQR: 2 15.1] days by LMP versus, 49.7 [IQR: 21.0] days by ultrasound; post-Dobbs median 56.0 [IQR: 21.7] days by LMP versus 56.0 [IQR: 23.8] days by ultrasound) all p < 0.05 (Table 4).
Gestational Duration at the Time of Appointment Scheduling and at the Time of Abortion Appointment
IQR, interquartile range; LMP, last menstrual period.
Discussion
This study suggests that increasing numbers of state-level abortion bans increase appointment wait times and therefore negatively impact abortion access for residents of states where abortion remains legal. In our study, New Mexico residents scheduling first-trimester abortion appointments waited two additional weeks to obtain an appointment in the first 3 months post-Dobbs, compared with before the Dobbs decision. Additionally, New Mexico residents called to schedule abortion appointments approximately 18 days earlier in pregnancy after the Dobbs decision, compared to the prior time period. This increase in wait time may add to existing delays from the many obstacles facing rural and underserved communities in accessing abortion care.
Evidence shows that state-level abortion restrictions delay care, leading to higher rates of second-trimester abortion, greater distances traveled to access abortion care, 13 and increased out-of-state travel. 14 After previous Texas abortion restrictions (many of which were later ruled unconstitutional), the proportion of abortions provided in New Mexico to Texas residents rose from 3% to 14% 15 and the proportion of abortions in the second trimester also significantly increased, from 3% to 26%. 15 Similarly after SB8, the proportion of Texas residents obtaining abortion care at a Colorado clinic rose significantly, from 1% to 17%; that study showed higher odds of all patients having a second-trimester abortion (adjusted odds ratios 2.6 for Texas residents and 1.8 for Colorado residents) compared with pre-SB8. 16 Our study demonstrated similar findings of longer appointment wait times for New Mexicans after the Dobbs decision triggered abortion bans in several states, presumably causing a surge in demand as more people nationwide called CRH to schedule abortion appointments.
Beginning with SB8 and continuing post-Dobbs, the abortion landscape in New Mexico shifted. Because CRH is the referral center in New Mexico for complex patients, appointment expansion efforts focused on second-trimester care. However, it is possible that changes in scheduling, addition of an abortion provider, and increased nursing staff also increased access to first-trimester appointments. Efforts to increase available abortion appointments may have contributed to stable wait times pre-SB8 and post-SB8. Additionally, post-Dobbs, additional clinics opened in New Mexico. These changes lend credibility to our findings as both would likely have reduced first-trimester abortion appointment wait times; the significant increases in wait time we found post-Dobbs occurred despite efforts to increase abortion access.
Our study is the first to show the impact that increasing numbers of state-level restrictive legislation have on residents of abortion-supportive states. In New Mexico, a state with some of the worst health outcomes nationally, the additional access burden for abortion care may expand health inequities that the state has been working for decades to reduce.
This study has several strengths. New Mexico is well-positioned to explore the impacts of restrictive legislation because of its proximity to many states that have banned or severely restricted abortion. Additionally, as a health center that accepts New Mexico Medicaid, which covers abortion care for low-income individuals, CRH likely attracts more New Mexico residents than other local health centers.
This study has several limitations and potential sources of bias. This retrospective review at a single clinic in a single city limits generalizability. During the post-SB8 and post-Dobbs study time periods, CRH increased staff and clinicians to expand clinical capacity, which would increase access and reduce wait times. Additionally, given the timing of these legislative changes, we were imperfectly able to control for any seasonality in abortion demand. Finally, the COVID-19 pandemic overlapped with our study periods; however, CRH provided the same number or slightly more abortions during the COVID-19 pandemic (pre-SB8) as before the pandemic. CRH experienced significant scheduling staff turnover, which affected demographic data input and particularly increased missingness; this may have affected our demographic analysis.
Conclusions
This study found that New Mexico residents called one to two weeks earlier for an abortion appointment and waited approximately 18 days longer for abortion care after the Dobbs decision restricted abortion access in surrounding states. The findings suggest that people living in abortion-supportive states are negatively affected by abortion restrictions. An increase in appointment wait times may be especially disruptive in rural and underserved states where residents face significant baseline barriers to accessing medical care.
Footnotes
Acknowledgment
The authors thank Timothy Petersen for data curation.
Authors’ Contributions
M.M.: Conceptualization, methodology, software, formal analysis, investigation, data curation, writing—original draft preparation, visualization, and funding acquisition. R.B.: Investigation. B.M.: Investigation. L.H.: Conceptualization, validation, writing—review and editing, and supervision. A.T.: Conceptualization, methodology, validation, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the University of New Mexico Department of OB/GYN Henrietta Lacks & Luis B. Curet Grant.