
Abstract
Background:
Postpartum care, including contraception, benefits maternal health and decreases mortality, which increased in the United States with COVID-19. Pandemic disruptions to postpartum health care access in vulnerable populations are not well understood. We utilize electronic health record (EHR) data for prenatal patients (n = 2,265) at six urban Federally Qualified Health Centers (FQHCs) from one year prepandemic (January 1, 2019) through one year after the first stay-at-home orders (“lockdown”) (March 31, 2021).
Objective:
We investigated (1) changes in rates of postpartum visit (PPV) and postpartum contraception receipt in the post-lockdown versus prepandemic periods and (2) characteristics predictive of differential changes in PPV and contraception rates.
Materials and Methods:
Visit and prescription records from EHR were used to classify if patients received PPV and most/moderately effective contraception within 60 days postpartum, analyzed separately and as a composite variable: PPV and contraception, PPV only, or no PPV. Risk differences comparing post-lockdown with pre-COVID-19 pandemic were estimated using binomial regression and generalized logistic regression models adjusted for age, race/ethnicity, language, and clinical site. Effect modification by sociodemographic and clinical covariates was examined.
Results:
Total patient volume fell 21% in the post-lockdown versus pre-COVID-19 period. Rates of PPV decreased in absolute terms by 9.6 (95% confidence interval: −13.6, −5.6) and contraception by 8.1 (−13.3, −2.8) percentage points. After adjustment, PPV and contraception decreased by 9.3 percentage points (−13.1, −5.4), while PPV only was stable (−0.4 [−4.3, 3.6]).
Conclusions:
These findings suggest a substantial impact of the COVID-19 pandemic on postpartum care in FQHCs and community health centers. Supply and demand drivers require further examination to inform strategies to improve postpartum care access and subsequent maternal health outcomes.
Introduction
Short interpregnancy intervals (IPIs), defined as less than 18 months between delivery and conception of the subsequent pregnancy, place birthing persons and infants at higher risk for poor health outcomes including preeclampsia, low birth weight, and perinatal death. 1 Yet, short IPI pregnancies are common. An analysis of National Survey of Family Growth data from 2006 to 2015 found that 36% of women with repeat pregnancies had short IPIs, 40% experienced unintended pregnancies, and the highest rates of unintended pregnancies occurred among those with the shortest IPIs. 2 The American College of Obstetricians and Gynecologists (ACOG) recommends comprehensive postpartum care, delivered at visits during the first 3 weeks after birth and again before 12 weeks postpartum, which provides patients an opportunity to discuss family planning and optimal birth spacing with their provider. 3 Yet an estimated 40% of postpartum individuals in the United States do not attend any postpartum visits (PPVs). 4 This constellation of short IPIs, unintended pregnancies, and missed postpartum care represents an unmet public health need. The COVID-19 pandemic exacerbated systemic barriers and limited access to care, including postpartum care. Short- and long-term effects of the pandemic on postpartum care are not well described.
Unmet needs for contraception are well documented. 5,6 Risk factors/markers for unmet contraception needs in the postpartum period span personal and systemic factors. 5 For those with pregnancy-related Medicaid coverage, accessing transportation to providers who accept Medicaid and lack of provider continuity are common barriers to patients receiving their desired type of contraception. 7 –9
PPVs serve as an opportunity for patients to receive care for pregnancy- or childbirth-related issues, to discuss preventive care including contraception, and to facilitate the transition of care to a primary care provider. 3,9 Systemic and structural barriers to equitable and universal receipt of postpartum care are well documented. 10 A recent systematic review of predictors of postpartum health care use among underserved populations reported significant associations between mothers’ socioeconomic status and postpartum health care use and identified barriers to care including lack of access to transportation and childcare, as well as having a newborn with health issues. 10 In Federally Qualified Health Centers (FQHCs), safety net settings that serve higher proportions of patients of color, those who are low income, and those who are publicly insured, greater parity and fewer prenatal care visits attended have been identified as predictors of PPV nonattendance. 11 Contraception access and uptake may be improved by addressing these risk factors and barriers to PPV attendance, especially among low-income and Medicaid-insured women who receive care at FQHCs.
The COVID-19 pandemic further exacerbated systemic barriers and limited access to care for many postpartum people. One study using data from the first 9 months of the pandemic reported declines in PPV receipt that were largest among non-Hispanic Black women, women ≤19 years old, and those without postpartum insurance. 12 One response to the COVID-19 pandemic was that providers began to offer telemedicine visits. 13 Two studies reported telemedicine increased or maintained PPV attendance early in the pandemic in the context of an academic medical center and an FQHC, respectively 14,15 ; however, according to a national survey of providers, telemedicine has limitations in providing contraception care. 16 These limitations are illustrated in studies reporting associations of telemedicine with a decrease in the use of long-acting reversible contraception (LARC) and receipt of desired sterilization, as these highest efficacy methods require in-person contact. 14,17 Additionally, low-income patients and those covered by Medicaid may experience barriers to accessing telemedicine, which may perpetuate or exacerbate disparities. 18 The extent to which the COVID-19 pandemic produced durable changes in PPV receipt and contraception uptake beyond the early weeks of the pandemic is not known. Reported increases in maternal and infant mortality following the start of the COVID-19 pandemic underscore the urgency of work to improve postpartum care and reduce disparities in access to essential family planning services. 19
The present study harnesses electronic health record (EHR) data from the baseline period of a cluster randomized stepped-wedge trial aimed at increasing postpartum contraception uptake in FQHCs in the United States. The aims of the current study are (1) to examine changes in PPV receipt, contraception uptake, and contraception type by time period with respect to the COVID-19 pandemic lockdown and (2) to identify patient characteristics that predict relatively larger changes in PPV and contraception rates, toward the goal of understanding the impacts of pandemic-related changes in care provision and access that may lead to poor maternal and infant health outcomes and inequity.
Materials and Methods
Population and data source
Five FQHC locations of care and one Community Health Center (hereafter referred to as “clinical sites”) that partner with one national Health Center Controlled Network (HCCN) of nearly 200 safety net clinical sites that contribute to a common data warehouse were included in this study. Clinical sites were participants in the Linking Inter-professional Newborn and Contraception Care (LINCC) trial, a stepped-wedge cluster randomized trial testing a systems-level intervention to increase receipt of postpartum contraception. Clinical sites in the HCCN were eligible for inclusion in the LINCC trial if they met a minimum threshold for volume of pregnant patients, had a staff person willing and available to serve as a clinical champion for the intervention, and agreed to participate. Participating clinical sites were located throughout the United States, with most in Chicago, IL. One LINCC clinical site outside of the continental United States was excluded because it was not comparable with other sites with respect to pre-Covid PPV rates and geographic context; this site serves a rural community, whereas all other sites are located in large urban areas. Clinical sites were assigned letters (A–F) as unique identifiers for this article to protect patient and provider anonymity. Data were obtained from the clinical sites’ EHRs. Data for the current study were from the baseline period of the LINCC trial prior to the implementation of the intervention. The study was initially approved by the institutional review board (IRB) at University of Chicago on January 22, 2019, and transferred to Rush University Medical Center’s IRB on July 8, 2021.
Data management
EHR data including demographics, visit history, diagnosis and procedure codes, and prescribed medications were provided to the study team by the HCCN for prenatal patients with a recorded or estimated delivery date between January 2019 and March 2021. Dates of delivery were only universally available for clinical site D, which uses a different EHR system that includes pregnancy episode data. Delivery dates for patients receiving care at the other five clinical sites (A, B, C, E, and F) were assigned using one of three strategies (applied in sequence): (1) Prenatal patients’ records were matched with infants’ records by home address, telephone number, last name, and/or guarantor listed on the infant’s record. For prenatal patients with a matched infant record (52.6%), the matched infant’s date of birth was assigned as the delivery date; (2) Delivery Current Procedural Terminology (CPT) codes were available in the records of a small subset of prenatal patients (2.8%). When delivery CPT codes were present, the date associated with those codes was assigned as the delivery date; or (3) For patients without a matched infant record or delivery code (44.6%), the delivery date was estimated using coefficients from a linear model predicting the time in days between the last prenatal visit and the delivery date. The model was run on all of the records with known delivery dates identified through strategies 1 and 2 above and included the following independent variables: gestational age at the last prenatal care visit, number of prenatal care visits attended, whether prenatal care was initiated in the first trimester, and indicator variables for the clinical sites. The prediction model achieved an R 2 = 0.65, indicating good model fit. For patients without a matched infant record or delivery code (group 3 above), the coefficients from the model were applied to the data values for the independent variables in the model to predict the number of days between the last prenatal visit and delivery for each observation in group 3. Then, that number was added to the (known) date of the last prenatal visit to generate an estimated date of delivery. This method was an improvement over simply using the estimated date of delivery, which assumes that every patient delivers at 40 weeks gestation.
In addition to delivery dates, Site D provided data about pregnancy losses and pregnancies for which prenatal care was transferred to a different provider due to high-risk status or other reasons. These pregnancies were excluded from the analysis to approximate the population of patients expected to return to that clinic for postpartum care. To mimic this population for the remaining five sites that did not have complete information on losses and transfers, analyses were restricted to patients who had four or more recorded prenatal care visits, the majority of which occurred at that clinical site, and the last of which occurred at or after 24 weeks of gestation. Prenatal appointments that did not continue beyond 24 weeks of gestation were considered likely indicative of a miscarriage or transfer of care. As 24 weeks gestation is the point of infant viability, this cutoff was set to avoid excluding birthing persons who did, in fact, complete their prenatal care at a participating site but delivered early.
Measures
Two main outcomes were examined: receipt of a PPV and receipt of a most or moderately effective method of contraception, each within 60 days postpartum (i.e., within 60 days after the recorded or estimated delivery date). 3,20 PPV was identified in the EHR as having a diagnosis or procedure code documented for routine postpartum care. Contraception was identified as having a prescription, diagnosis, or procedure code for a most/moderately effective form of contraception. 20 Most effective contraception includes sterilization, implants, and intrauterine devices. Moderately effective contraception includes injectables, oral pills, patches, and rings. To account for the inter-relatedness of these two postpartum services, a composite outcome was developed with three levels: PPV and contraception, PPV no contraception, and no PPV. The “No PPV” category is labeled as such because a small number of people in that category had a contraception prescription, but no PPV recorded.
The exposure variable was the timing of delivery with respect to the initial COVID-19 pandemic lockdown. The lockdown period was considered to have begun in March of 2020 21,22 and ended in May 2020. 23,24 Patients who delivered in January through December 2019 were in the pre-COVID cohort because their 60-day postpartum period occurred before the COVID-19 pandemic lockdown, while patients who delivered in April 2020 through March 2021 were in the post-lockdown cohort. Those who delivered in January through March 2020 were excluded from the present analysis as some or all of their 60-day postpartum period occurred during the COVID-19 pandemic lockdown when access to routine care was severely curtailed.
Covariates were included in the analysis if they had a theoretical relationship to both the exposure and outcome and were not in the causal pathway. The covariates examined were age, race/ethnicity, preferred language, receipt of first trimester prenatal care, number of previous pregnancies, chronic and obstetric comorbidities, and clinical site. Chronic conditions from a modified list of chronic comorbidities predictive of severe maternal morbidity 25 were identified using diagnosis codes. These included pulmonary hypertension, chronic renal disease, preexisting bleeding disorder, preexisting cardiac disease, HIV/AIDS, gastrointestinal disease, acute or moderate/severe asthma, connective tissue or autoimmune disease, chronic hypertension, preexisting diabetes, thyrotoxicosis, and body mass index of 40 or higher. Mental health and substance use disorders were analyzed separately from other chronic conditions. Obstetric comorbidities included placenta accreta spectrum, partial or complete placenta previa, preeclampsia with or without severe features, eclampsia, placental abruption, gestational hypertension, and gestational diabetes. 25 No cases of placenta accreta spectrum, pulmonary hypertension, or placental abruption were observed, likely due to the lack of availability of inpatient records for delivery hospitalizations.
Statistical analysis
Descriptive statistics for all outcomes and covariates were calculated by time period (i.e., timing of delivery with respect to the COVID-19 lockdown), and chi-square tests were performed. Crude risk differences (RD) with 95% confidence intervals (CI) were calculated comparing each outcome in the post-lockdown versus pre-COVID periods. Interactions between the exposure and all covariates were explored by calculating stratified RDs and 95% CIs. Adjusted RDs and time-by-covariate interaction p-values for each binary outcome were estimated from multivariable generalized linear regression models with a binomial distribution and identity link. Crude and adjusted RDs for the composite outcome were estimated from multinomial logistic regression models using the margins utility in Stata. Interaction p-values <0.10 were considered statistically significant. Analyses were performed using SAS 9.4 (SAS Institute: Cary, NC) and Stata 17 (StataCorp: College Station, TX).
Results
EHR data from 3,593 prenatal patients at six clinical sites were available. Of those, 1,266 from the pre-COVID-19 period and 999 from the post-lockdown period met the inclusion criteria for this analysis. Overall, there were 21% fewer eligible patients in the post-lockdown period compared with the pre-COVID-19 period. Four of the six sites had large, statistically significant decreases in the number of eligible patients post-lockdown versus pre-COVID, while the other two sites had small, nonsignificant increases in eligible patients over the same time period (Fig. 1). The demographic characteristics of the pre- and post-groups were similar, while rates of the main outcomes and of comorbidities differed (Table 1). Compared with those who delivered pre-COVID-19, the proportions of those in the post-lockdown group with a PPV or contraception by 60 days postpartum were significantly lower. The percentage of people who both attended a PPV and received contraception by 60 days postpartum decreased, while the percentage who attended a PPV but did not receive contraception remained steady, and the percentage who did not attend a PPV increased. The rates of obstetric comorbidities, chronic comorbidities, and mental health/substance use disorders were slightly higher in the post-lockdown period versus pre-COVID-19.
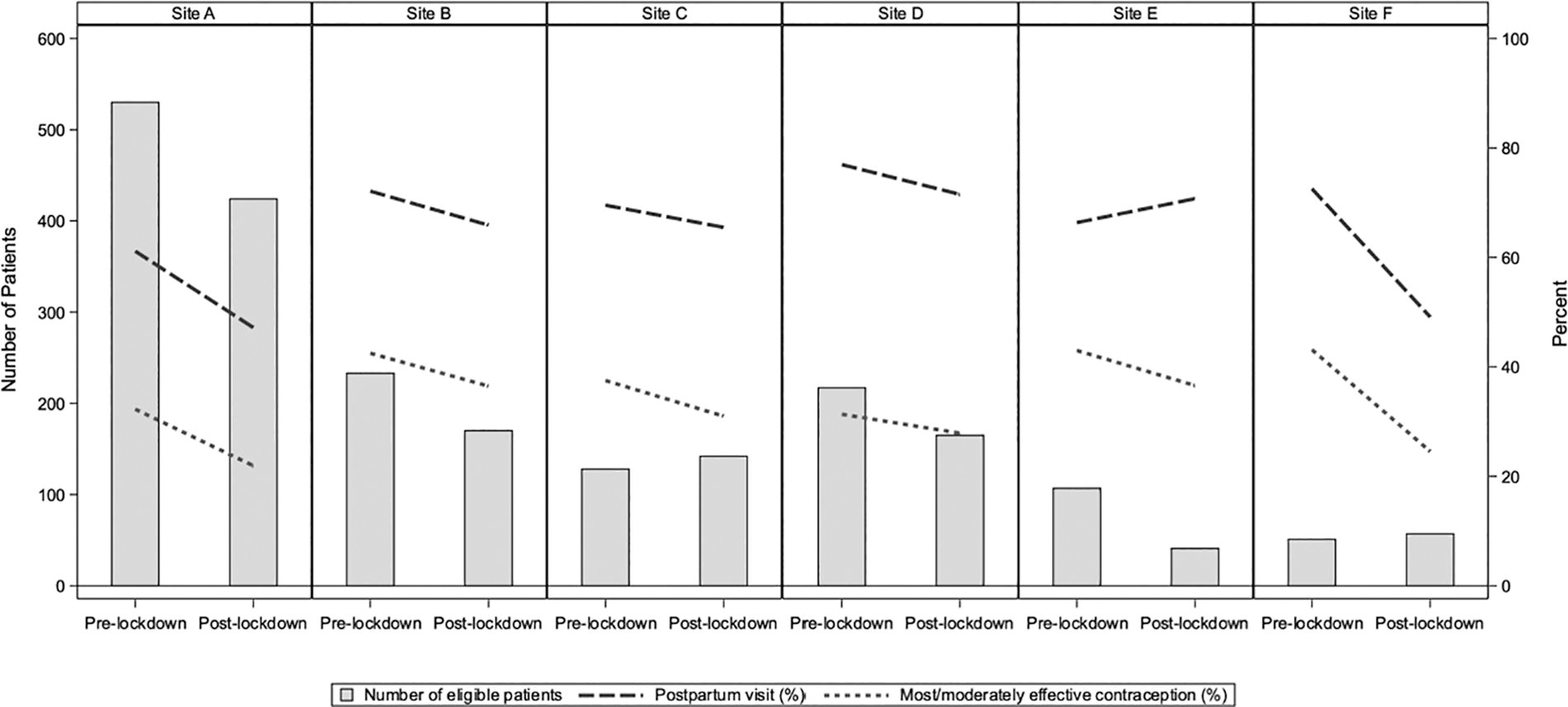
Postpartum visit and most/moderately effective contraception by 60 days postpartum by clinical site and time period with respect to the COVID-19 pandemic.
Characteristics of Eligible Patients and Rates of Postpartum Visit and Contraception by Period with Respect to the COVID-19 Pandemic Stay-at-Home Orders
The pre-COVID-19 period includes pregnant persons who gave birth before January 1, 2020, as their 2-month postpartum date occurred before the United States was under stay-at-home orders due to COVID-19. The lockdown period (excluded from the study) includes pregnant persons who gave birth between January 1, 2020, and March 31, 2020, whose 2-month postpartum date occurred during the months when much of the United States was under stay-at-home orders. The post-lockdown period covers pregnant persons who gave birth on or after April 1, 2020.
p-Values are for the chi-squared statistic comparing pre-COVID-19 with post-lockdown for each covariate.
Postpartum visit and contraception by 60 days postpartum.
Prenatal care information was not available for site “D.”
Obstetric comorbidity includes major pregnancy-related conditions, the most common of which is gestational diabetes. 26
Chronic diseases included pulmonary hypertension, chronic renal disease, preexisting bleeding disorder, preexisting cardiac disease, HIV/AIDS, gastrointestinal disease, acute or moderate/severe asthma, connective tissue or autoimmune disease, chronic hypertension, preexisting diabetes, thyrotoxicosis, and BMI of 40 or higher. 26
BMI, body mass index.
The PPV rate declined by 9.6 percentage points (95% CI: −13.6, −5.6) in the post-lockdown period compared with the pre-COVID-19 period, to 58.1% from 67.6% (Table 2). The change from pre-COVID to post-lockdown in PPV receipt varied most by clinical site, though the interaction p-value was not statistically significant. Clinical sites A and F saw the largest decreases in PPV receipt (Table 2; Fig. 1). Differential changes in PPV rates by sociodemographic and health characteristics were of smaller magnitude, but declines were apparent across nearly all patient subgroups.
Postpartum Visit Rate by 60 Days Postpartum, by Time Period with Respect to the COVID-19 Pandemic and Patient Characteristics
The pre-COVID-19 period includes pregnant persons who gave birth before January 1, 2020, as their 2-month postpartum date occurred before the United States was under stay-at-home orders due to COVID-19. The lockdown period (excluded from the study) includes pregnant persons who gave birth between January 1, 2020, and March 31, 2020, whose 2-month postpartum date occurred during the months when much of the United States was under stay-at-home orders. The post-lockdown period covers pregnant persons who gave birth on or after April 1, 2020.
p-Values (chi-squared) for the interactions between each covariate and period (pre/post-lockdown) did not reach statistical significance.
Non-Hispanic White, Non-Hispanic Asian, multiracial, and other racial/ethnic groups.
Obstetric comorbidity includes major pregnancy-related conditions, the most common of which is gestational diabetes. 26
Chronic diseases included pulmonary hypertension, chronic renal disease, preexisting bleeding disorder, preexisting cardiac disease, HIV/AIDS, gastrointestinal disease, acute or moderate/severe asthma, connective tissue or autoimmune disease, chronic hypertension, preexisting diabetes, thyrotoxicosis, and BMI of 40 or higher. 26
BMI, body mass index; CI, confidence interval; PPV, postpartum visit.
Among patients with a PPV, the percentage who received most/moderately effective contraception within 60 days postpartum decreased from 50.1% to 42.1% after the COVID-19 lockdown (RD: −8.1, 95% CI: −13.3, −2.8) (Table 3). Contraception rates declined at all sites, but the magnitude of the change differed (Table 3; Fig. 1). Pre-COVID-19, having an obstetric comorbidity was associated with higher contraception rates among those who attended a PPV compared with those without an obstetric comorbidity (57.1% versus 49.7%), while post lockdown, those with an obstetric comorbidity had lower contraception rates than those without (30.6% versus 42.1%, time period-by-obstetric comorbidity interaction p-value = 0.052) (Table 3). After adjusting for age, race/ethnicity, preferred language, and clinical site, among those who attended a PPV, persons with obstetric comorbidities experienced a larger decline in postpartum contraception receipt than those without an obstetric comorbidity (interaction p-value = 0.06) (Table 4).
Most/Moderately Effective Contraception Rate by 60 Days Postpartum, by Patient Characteristics and Time Period with Respect to the COVID-19 Pandemic Among Those with a Postpartum Visit by 60 Days Postpartum
The pre-COVID-19 period includes pregnant persons who gave birth before January 1, 2020, as their 2-month postpartum date occurred before the United States was under stay-at-home orders due to COVID-19. The lockdown period (excluded from the study) includes pregnant persons who gave birth between January 1, 2020, and March 31, 2020, whose 2-month postpartum date occurred during the months when much of the United States was under stay-at-home orders. The post-lockdown period covers pregnant persons who gave birth on or after April 1, 2020.
p-Values (chi-squared) for the interaction between each covariate and period (pre/post-lockdown) did not reach statistical significance except where noted.
Non-Hispanic White, Non-Hispanic Asian, multiracial, and other racial/ethnic groups.
Obstetric comorbidity includes major pregnancy-related conditions, the most common of which is gestational diabetes. 26
Chi-squared test p-value <0.1 for the interaction between the covariate and period (pre/post-lockdown).
Chronic diseases included pulmonary hypertension, chronic renal disease, preexisting bleeding disorder, preexisting cardiac disease, HIV/AIDS, gastrointestinal disease, acute or moderate/severe asthma, connective tissue or autoimmune disease, chronic hypertension, preexisting diabetes, thyrotoxicosis, and BMI of 40 or higher. 26
BMI, body mass index; CI, confidence interval.
Risk Differences and 95% Confidence Intervals of Having a Postpartum Visit and Most/Moderately Effective Contraception by Time Period with Respect to the COVID-19 Pandemic Estimated from Binomial Regression Models
By 60 days postpartum.
Most/moderately effective contraception among those with a postpartum visit.
p-Values (chi-squared) for risk difference post-lockdown versus pre-COVID within each stratum from binomial regression models.
Adjusted for age, race/ethnicity, preferred language, and clinical site.
Stratified by obstetric comorbidity (yes/no). Obstetric comorbidity includes major pregnancy-related conditions, the most common of which is gestational diabetes. 26 Interaction p-value for postpartum visit model = 0.66. Interaction p-value for contraception model = 0.06.
CI, confidence interval.
With respect to the composite outcome, the percentage of patients who both attended a PPV and received contraception within 60 days postpartum decreased by 9.5 percentage points (95% CI: −13.2, −5.7) after versus before the COVID-19 lockdown, while the percentage who attended only a PPV remained steady (RD: −0.1, 95% CI: −4.0, 3.8) (Supplementary Table S1). These trends persisted after adjusting for age, race/ethnicity, preferred language, and clinical site (Table 5).
Risk Differences and 95% Confidence Intervals of a Three-Level Composite Postpartum Visit and Contraception Outcome by Time Period with Respect to the COVID-19 Pandemic Estimated from Generalized Logistic Regression Models
By 60 days postpartum.
p-Values (chi-squared) for risk difference post-lockdown versus pre-COVID within each stratum from generalized logistic model with no postpartum visit as the reference.
Adjusted for age, race/ethnicity, preferred language, and clinical site.
CI, confidence interval.
Type of contraception used did not change in the post-lockdown versus the pre-COVID-19 periods among most/moderately effective contraception users (Fig. 2; Supplementary Table S2). Oral contraception, injections, implants, and intrauterine devices were the most common methods, while sterilization, patches, and rings were reported for fewer than 10% of patients in total.
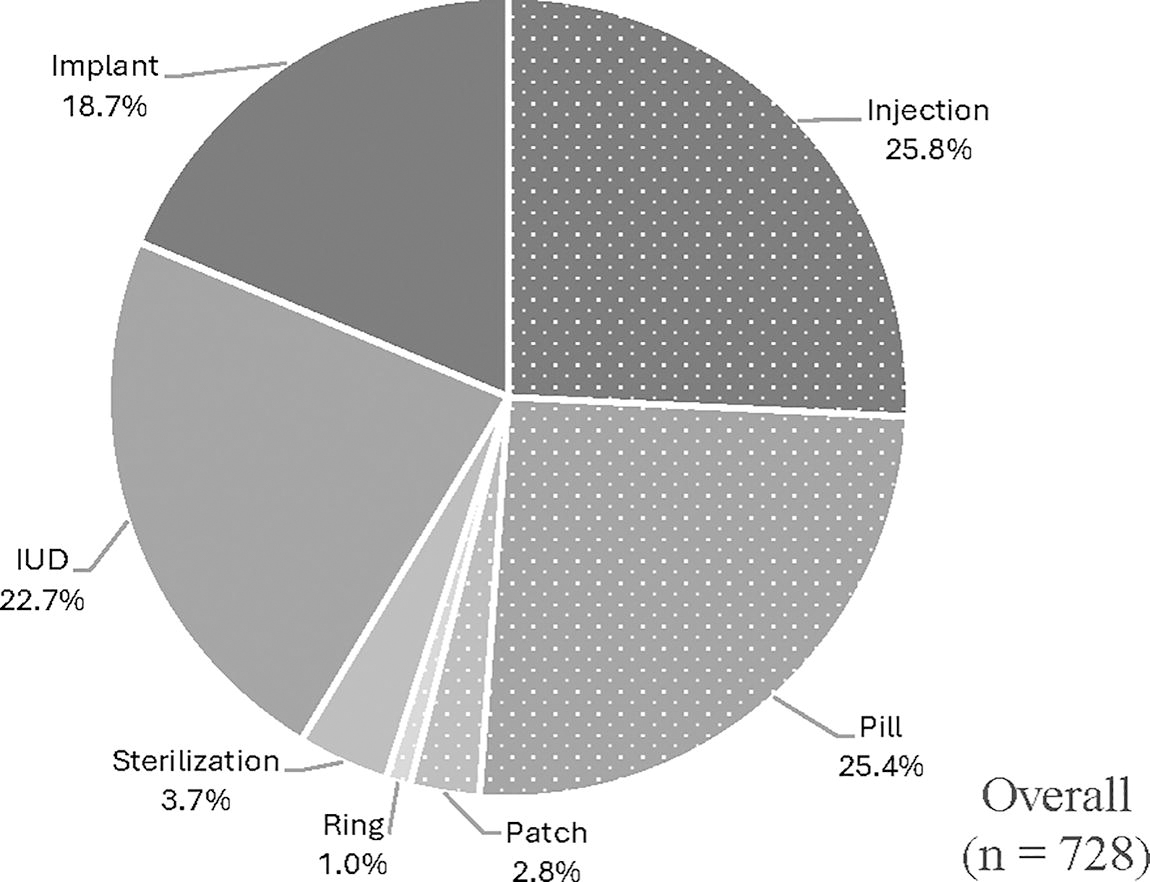
Method of most/moderately effective contraception for those with contraception by 2 months postpartum among patients pre-COVID-19 and post-lockdown (n = 728). Most effective contraception methods are displayed in solid shades of gray (implant, IUD, sterilization). Moderately effective contraception methods are displayed in dotted shades of gray (injection, pill, patch, ring). Chi-squared tests for associations between time-period and contraception method or effectiveness designation were not statistically significant (p-values of 0.25 and 0.32, respectively). Percentage using each contraception method by time-period is shown in Supplementary Table S2. IUD, intrauterine device.
Discussion
This study examined the change in PPV and contraception rates following the first COVID-19 pandemic lockdown among prenatal patients served by FQHCs to understand the potential impact of the COVID-19 pandemic on postpartum care and to identify differential changes by patient characteristics. The proportion of patients who received timely PPV and contraception (within 60 days postpartum) decreased post-lockdown. The magnitude of the declines in postpartum contraception differed by the presence or absence of an obstetric comorbidity (e.g., gestational diabetes), with patients with an obstetric comorbidity seeing larger declines.
The decreases in PPV and contraception post-lockdown observed in this study have not been observed universally in other studies. 14,15,17,26,27 A decreased postpartum contraception rate post-lockdown was reported by at least one large national study, 28 while several studies that reported no decrease in PPV examined only one large medical center and had higher PPV rates pre-COVID-19 than the FQHCs included in this study. 14,17,26,27 However, setting and baseline PPV rates may not explain the discrepancy entirely, as one small study in a New York FQHC, which had low pre-COVID-19 PPV rates, also found no decrease in PPV or contraception rates in a short post-lockdown period (June–August 2020). 15 Most studies attributed the maintenance of or increase in PPV rates to the use of telehealth. 14,15,17,26 In our study, whether a visit was in-person or via telehealth was not clearly indicated in the data. We examined free-text fields and diagnosis and procedure codes for indications of telehealth; however, there was no uniform or consistent way that clinics indicated a visit was virtual, so conclusions about how often telehealth was used for PPV could not be drawn. It is possible that the clinics and/or patients in our study were less able to utilize telehealth compared with the sites in previous studies given telehealth is less accessible to underserved populations who receive care at FQHCs. 29 This could have contributed to the observed lower PPV rates in the post-lockdown period.
The declines in PPV and contraception rates may have been impacted by an increase in the provision of immediate postpartum LARC during the delivery hospitalization. 26,30,31 Though this was not directly observable in the available EHR data for this study, prior studies of postpartum contraception during the COVID-19 pandemic report the same. 26,30,31 Provision of immediate postpartum LARC was encouraged during the COVID-19 pandemic to avert unnecessary in-person PPVs. 26,32,33 This may have been an especially important driver for those with obstetric comorbidities, who tended to shift away from obtaining contraception from the FQHCs and may have been more motivated to secure access to contraception during the delivery hospitalization. For some conditions (hypertension, diabetes, preeclampsia, etc.) that are associated with an increased risk of adverse reactions to some contraceptive methods, LARC may be preferred because combined hormonal contraception is not advised. 34,35 This would be an important issue to disentangle in a future study, as appropriate intervention strategies would depend on whether PPV and contraception declined in the post-COVID-19 period, or whether PPV declined perhaps in part because contraception was more readily accessible during the delivery hospitalization. While this would reflect success in maintaining access to contraception, other goals of the PPV related to screening for postpartum complications and linking patients back to primary and preventative care could be neglected with a shift away from timely PPVs.
The decline in the PPV rate may also be explained by more fragmented care in the post-lockdown period. Anecdotally, clinics experienced workforce shortages during the pandemic, which could contribute to diminished continuity of care postpartum if clinics could not schedule timely appointments or patients found new providers elsewhere. In this study, PPVs at clinical sites other than the location of prenatal care were not captured, which is a limitation as patients can be seen at various clinical sites within an FQHC. Finally, the following factors likely also contributed to declines in PPV and contraception post-lockdown: reduced access to nonemergency care, changes in provider availability due to infections and quarantines, barriers to utilizing telehealth services, patients’ desires to avoid exposure to COVID-19 in public places including health care facilities, financial hardship, emotional and psychological consequences of the pandemic and lockdown, and a reduction in prenatal planning for how/when to obtain postpartum services. 27,29 The higher acuity (i.e., higher rates of chronic and obstetric comorbidities) of eligible patients paired with lower overall PPV rates post-lockdown compared with pre-COVID-19 suggests more complicated cases may have been more likely to receive postpartum care, while healthier patients had lower follow-up or less continuity in postpartum care in the post-lockdown period. Future studies could investigate the forces behind these shifts—whether this filtering or triage was driven by providers, by patients or some combination, and how they affected patient outcomes.
We originally hypothesized that the pandemic would increase disparities in care, such that declines in PPV and contraception rates would be greatest in already underserved populations. However, evidence that declines in either PPV or contraception differed by patient sociodemographic characteristics such as race/ethnicity did not reach statistical significance. Differences by clinical site were more apparent (though not statistically significant), and variability between sites may have obscured differences by patients’ characteristics. Some clinic-level factors that may indicate pandemic-related impacts and adaptations, such as staff turnover rate and availability and uptake of telehealth, were not available in the data for this study. It may be that a larger difference would be observed between more disparate clinic types, for example, between large medical centers and FQHCs, as FQHCs may have had fewer resources available to adapt to providing routine care during and after the COVID-19 lockdown. Notably, FQHCs also tend to serve patient populations that were excessively burdened by COVID-19 infections. 36
There are limitations to what can be concluded from this study. The FQHCs included in this study may not be representative of all FQHCs as they were centered around large urban areas and had demonstrated capacity to participate in an intervention trial. EHR data are not collected primarily for research and can contain incomplete or inaccurate information, which in this study could lead to misclassification of the outcome or the exposure. Furthermore, information about important covariates such as insurance status during the prenatal/postpartum period were unavailable for this retrospective study, since that data field is rewritten every time it changes, with no historical data archived in the database. However, most prenatal patients receiving care at participating sites were covered by Medicaid. Care delivered outside of the participating clinical sites, such as during hospitalizations, was not captured in our study. These limitations of the available data were nondifferential with respect to the exposure (i.e., time period), such that if they introduced bias, it would be toward the null, that is, the results presented here would be conservative. Mostly though, these limitations introduce ambiguity in the interpretation of the changes we observe. Unfortunately, fragmented data systems among FQHCs and community health centers and between FQHCs/community health centers and hospitals are more the norm than the exception. Still, studies using these data sources can improve the representation of underserved and at-risk patients in the literature and can inform future studies and interventions. Other limitations include that patient demographics, such as race/ethnicity, age, language preference, and comorbidities, were closely tied to clinical site, which complicated disentangling differences by patient race/ethnicity and other characteristics from differences by clinical site. Given the nature of antenatal and PPV data, the analysis is conducted at the clinic level rather than at the individual level. For that reason, it is not always possible to distinguish between a change in the burden of a condition (e.g., mental health or OB comorbidity diagnoses) in the underlying population and a change in the proportion or composition of the population represented in the sample of postpartum patients during that study period. Finally, this study examined care within 60 days postpartum and therefore does not address the newest ACOG guidelines to initiate care within 3 weeks or take into account more recent expansions in Medicaid coverage periods, neither of which had been fully implemented during the study period. 3,37 Nevertheless, this study has many strengths. By using data from a HCCN, this study can add the experiences of multiple FQHCs, including those smaller in size, to the literature. Furthermore, using medical record data allowed for assessing associations of comorbidities with care. Finally, by excluding the first months of lockdown, the study highlights longer-term effects of associations of the pandemic on PPV and contraception receipt.
Conclusions
This study found that fewer prenatal patients at the six participating FQHCs received timely PPV and contraception in the year after lockdown compared to before the COVID-19 pandemic. More research is needed to understand the underlying forces driving these changes and how the situation has evolved subsequently. Whether these observed shifts reflect lower rates of postpartum care or disrupted continuity of care, the findings highlight a need for renewed strengthening of postpartum care planning and systems to ensure people have timely access to the services and care they need and desire, including contraception. Emergency planning is also needed to ensure that access to time sensitive preventative care and screenings is maintained especially for underserved populations during disruptions to health care delivery such as those that occurred during the COVID-19 pandemic.
Footnotes
Authors’ Contributions
R.K.C., E.G., R.C., K.R., and S.H.: Conceptualization. R.K.C., E.G., and K.R.: Analysis. R.K.C., E.G., C.B., and K.R.: Writing—original draft. All authors: Writing—review and editing. R.C., S.H., and K.R.: Supervision. R.C., C.B., J.W.G., S.H., and N.M.: Project administration. R.C. and S.H.: Funding acquisition.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This work was supported by National Institutes of Health/National Institute of Child Health and Human Development funding: 5R01HD097171.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.