
Abstract
Background:
People with physical disabilities are at increased risk of adverse perinatal outcomes, including severe maternal morbidity (SMM). Risks may be even greater for disabled people in minoritized racial or ethnic groups, but little is known about this intersection.
Methods:
We analyzed linked hospital discharge and vital records data from California, 2008–2020. We identified physical disabilities using diagnosis codes for maternal congenital anomalies, major injuries, musculoskeletal disorders, or nervous system disorders. We compared birthing persons in five groups (Black and Hispanic with and without physical disabilities, White with physical disabilities) to a reference group of non-Hispanic Whites without disabilities. We used Poisson regression to assess associations with SMM and other outcomes, with and without adjusting for sociodemographic and clinical covariates.
Results:
Disabled Black and Hispanic birthing persons had particularly high relative risks (RRs) of SMM (Black disabled RR = 6.13, 95% confidence interval [CI]: 4.94, 7.61; Hispanic disabled RR = 3.67, 95% CI: 3.29, 4.10) as compared with nondisabled White persons. These risks were greater than those for nondisabled Black (RR = 2.05, 95% CI: 1.99, 2.11), nondisabled Hispanic (RR = 1.36, 95% CI: 1.34, 1.39), and disabled White birthing persons (RR = 2.44, 95% CI: 2.16, 2.77). For most other outcomes, risks were also largest for disabled Black birthing persons, followed by disabled Hispanic birthing persons.
Conclusions:
Black and Hispanic people with physical disabilities are highly likely to experience SMM and are at increased risk for other complications and adverse outcomes. Efforts are needed to understand underlying causes of these disparities and develop policies and practices to eliminate them.
Introduction
Pregnancy and birth have become increasingly common among people with physical disabilities. 1,2 Most of these pregnancies and births proceed without major complications. However, birthing persons with physical disabilities are more likely than those without disabilities to experience pregnancy complications such as gestational diabetes and hypertensive disorders. 3 Moreover, there is growing evidence that people with physical disabilities are at heightened risk of less common but potentially life-threatening complications, collectively known as severe maternal morbidity (SMM). 4 –6
Multiple studies have found that SMM is increasing in the United States, 7 –10 underscoring the importance of identifying and addressing factors contributing to SMM. The burden of SMM is unequally distributed by race and ethnicity, with significantly higher rates in Hispanic and non-Hispanic Black populations compared with non-Hispanic Whites. 7 –12 Risks experienced by Black and Hispanic birthing persons may be even greater when intersecting with physical disability, and vice versa. Disparities in health risks can combine in an additive manner (e.g., in which the total increased risk is the sum of the individual components) but may also combine in unexpected and sometimes synergistic ways for people with multiple marginalized identities. As an example of the former, one study of preconception health found that the risk of obesity among Black women with disabilities was equal to the sum of the risks for Black women without disabilities and White women with disabilities. 13 As yet, however, little is known about SMM and other perinatal complications and adverse outcomes among physically disabled birthing persons in minoritized racial and ethnic groups.
A better understanding of the patterns of risk for potentially life-threatening complications can inform improvements in perinatal care to help address inequities, reduce risks, and manage complications. Therefore, we examined SMM and other perinatal complications—including gestational hypertension, preeclampsia, gestational diabetes, perinatal mental disorders, cesarean delivery, preterm delivery, venous thromboembolism (VTE), chorioamnionitis, and puerperal endometritis—at the intersection of physical disability with minoritized race or ethnicity. We hypothesized that SMM and other complications would be more common among birthing persons with physical disabilities and those in minoritized racial and ethnic groups, compared with non-Hispanic White birthing persons without disabilities. Furthermore, we hypothesized that the combination of physical disability and Black race or Hispanic ethnicity would be associated with greater risk than either characteristic alone.
Materials and Methods
We conducted a retrospective cohort study using linked vital statistics and hospital discharge data from California for the years 2008–2020. Using probabilistic linkage, we linked birth and fetal death certificate data (vital statistics) maintained by the California Department of Public Health to patient discharge data maintained by the Department of Health Care Access and Information. Probabilistic linkage uses a combination of available common data elements present in both datasets, such as neonate’s birth date and gender, birth hospital, birthing patient’s residential zip code, and hospital county. 14 In total, 94.2% of the vital statistics records were successfully linked, and a subset of these records was reviewed manually to verify correct application of the linkage algorithm. See Supplemental Supplementary Table S1 for a comparison of individuals included in the analytic sample with those excluded due to nonlinkage. The linked dataset contained all maternal and neonatal characteristics derived from birth and death certificates, as well as diagnosis and procedure codes recorded using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9; 2008 to October 2015) and International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10; October 2015 to 2020) from hospital discharge records. This study was approved by the Oregon Health & Science University’s Institutional Review Board and the California Health and Human Services Agency’s Committee for the Protection of Human Subjects.
We identified maternal physical disability using ICD-9 and ICD-10 codes associated with physical disability (see Supplemental Supplementary Table S2), as established in previous studies. 4,15 Additionally, we used diagnosis codes from prior research 4,15,16 to identify isolated nonphysical disabilities (hearing, vision, intellectual, and developmental disabilities); if no physical disability was present, records with diagnosis codes for these other disability types were excluded from our analyses. For the remaining records, we created a dichotomous indicator of disability status (physical disability versus no disability).
Race and ethnicity were extracted from vital records data. This study focused on three racial and ethnic groups: Hispanic of any race, non-Hispanic Black, and non-Hispanic White. We created a variable reflecting the intersection of physical disability status with race and ethnicity, including the following six groups: (1) Hispanic with physical disability, (2) non-Hispanic Black with physical disability, (3) non-Hispanic White with physical disability, (4) Hispanic with no disability, (5) non-Hispanic Black with no disability, and (6) non-Hispanic White with no disability.
Our primary outcome of interest was SMM, a composite variable reflecting presence of one or more life-threatening complications such as eclampsia, pulmonary embolism, heart failure, and sepsis. We created our SMM variable using diagnosis and procedure codes specified by the U.S. Centers for Disease Control and Prevention 17 and previously validated in California data. 18 We used length of stay to refine our SMM classification, as recommended in prior research. 19 Deliveries with a length of stay less than the 90th percentile (calculated separately for vaginal, primary cesarean, and repeat cesarean deliveries) were not categorized as SMM unless procedure codes for hysterectomy, blood transfusion, or ventilation were present. 19 Blood transfusion is the most common SMM indicator but can be less severe than other SMM markers, especially in the absence of data on units of blood transfused (what was not available in our data). 18 Therefore, we analyzed two different SMM variables: one that included blood transfusion and one without blood transfusion. Our secondary outcomes included gestational hypertension; preeclampsia; gestational diabetes; mental health disorders complicating pregnancy, childbirth, or the puerperium; cesarean delivery; preterm delivery (<37 weeks); early preterm delivery (<34 weeks); VTE; chorioamnionitis; and puerperal endometritis (see details in Supplemental Supplementary Table S2).
We restricted our analyses to singleton births with gestational ages ranging from 23 to 42 weeks. We calculated prevalence of maternal characteristics and outcomes by the combination of physical disability status and race or ethnicity. We then conducted unadjusted and adjusted modified Poisson regression analyses to obtain relative risks (RRs) and 95% confidence intervals (CIs) for the association of physical disability status and race/ethnicity with SMM and each of our secondary outcomes, using the “non-Hispanic White with no disability” category as the reference group. When considering socially patterned disparities, the unadjusted association will often be of most relevance because it documents the full level of inequity between population groups. In addition, we were interested in the degree to which covariates that differ between population groups may influence the associations. Therefore, we included several sociodemographic and clinical covariates in adjusted models (see Supplementary Table S2 for data sources and codes used to define covariates).
Sociodemographic covariates included maternal age at delivery (<20, 20–34, ≥35), maternal education (high school or less versus at least some college), and insurance (public or private). Maternal health characteristics and pregnancy/delivery characteristics covariates included: chronic hypertension, pre-existing diabetes, body mass index (BMI) (<18.5, 18.5–<25, 25–<30, 30 or higher), smoking during pregnancy (yes/no), diagnosis of substance use disorder (yes/no), parity (primiparous versus multiparous), Kotelchuck index of prenatal care adequacy (inadequate/intermediate versus adequate/adequate plus), 20 and preterm delivery (gestational age less than 37 weeks). Maternal age, education, BMI, insurance type, parity, timing of prenatal care initiation, and year of delivery were included as covariates in all our multivariable regression analyses. We adjusted for maternal health covariates in most analyses; however, we neither included pre-existing diabetes in models of gestational diabetes nor chronic hypertension in models of gestational hypertension. We adjusted for preterm delivery in analyses of postpartum outcomes. To supplement our main analyses, which simultaneously assessed associations of both race/ethnicity and disability with outcomes via confounder-adjusted analyses, we also conducted propensity score-matched multivariable regression analyses. The propensity-matched models compared birthing persons with and without disabilities within each racial and ethnic group, specifically assessing the association between disability and outcomes for each racial and ethnic group separately, matching on a variable that indexes across multiple confounders.
We had a small amount of missing data: maternal age (n = 1), prepregnancy BMI (n = 217,899; 4.7%), insurance (n = 99), parity (n = 2,448, 0.05%), prenatal care initiation (n = 80,567, 1.75%), and smoking during pregnancy (n = 40,923; 0.89%). We addressed missing data by performing multiple imputation using chained equations to generate 20 imputed datasets before conducting regression analyses. Pooled estimates were performed according to Rubin’s rule. 21 Analyses were conducted in Stata (version 17; Stata Corp, College Station, TX).
Results
After excluding multifetal gestations (n = 178,460), gestational ages less than 23 weeks or greater than 42 weeks (n = 19,273), isolated nonphysical disabilities (n = 8,849), and racial and ethnic groups other than Hispanic, non-Hispanic Black, or non-Hispanic White (n = 1,026,756), a total of 4,608,004 births met the criteria for inclusion in our analyses (Fig. 1). Of these, 0.46% (n = 21,166) had diagnoses associated with physical disability. The majority of those with physical disabilities were non-Hispanic White (50.5%; n = 10,685), followed by Hispanic (43.2%; n = 9,142) and Black (6.3%; n = 1,339). This differed from birthing persons without disabilities, of whom more than 60% were Hispanic (n = 2,833,689). In each racial and ethnic group, larger proportions of birthing persons with physical disabilities were at least 35 years of age, had some college education, and had private insurance, as compared with their counterparts without disabilities. Chronic hypertension, diabetes, and substance use were more common among people with disabilities, with particularly high prevalence of hypertension (10.9%) among Black disabled birthing persons (Table 1).
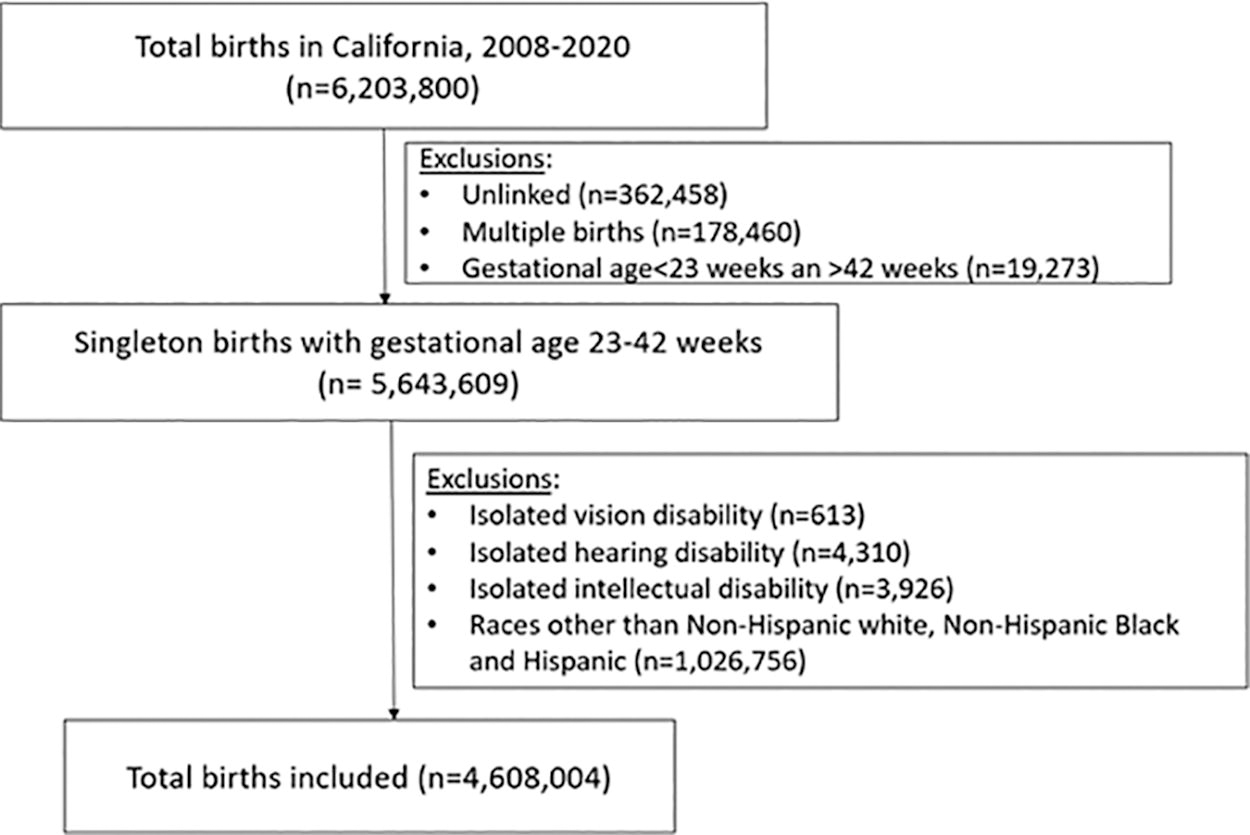
Analytic sample.
Sociodemographic and Clinical Characteristics by Race, Ethnicity, and Disability; California, 2008–2020
Chi-square test.
Percentages add up to more than 100% because some people had more than one type of physical disability.
BMI, body mass index; N/A, not applicable.
Among both disabled and nondisabled birthing patients, SMM was more common for Black and Hispanic birthing persons as compared with their non-Hispanic White counterparts. Differences in SMM between racial and ethnic groups were somewhat larger among birthing persons with physical disabilities than among those without disabilities (Fig. 2). In each racial and ethnic group, deliveries among those with physical disabilities were substantially more likely to have indications of SMM. However, the magnitude of the difference between birthing persons with and without disabilities differed by race and ethnicity. Among non-Hispanic White patients, the proportion of deliveries with SMM was 2.4 times greater for those with versus without physical disabilities (232 per 10,000 versus 95 per 10,000). Among Hispanic birthing patients, the proportion was 2.7 times higher for those with versus without disabilities (349 per 10,000 versus 130 per 10,000); and among non-Hispanic Black patients, SMM was three times as likely to occur in deliveries to those with physical disabilities compared with those without disabilities (583 per 10,000 versus 195 per 10,000) (Fig. 2). Differences between birthing persons with and without physical disabilities were even greater when blood transfusion was excluded from the SMM indicator (Fig. 3).
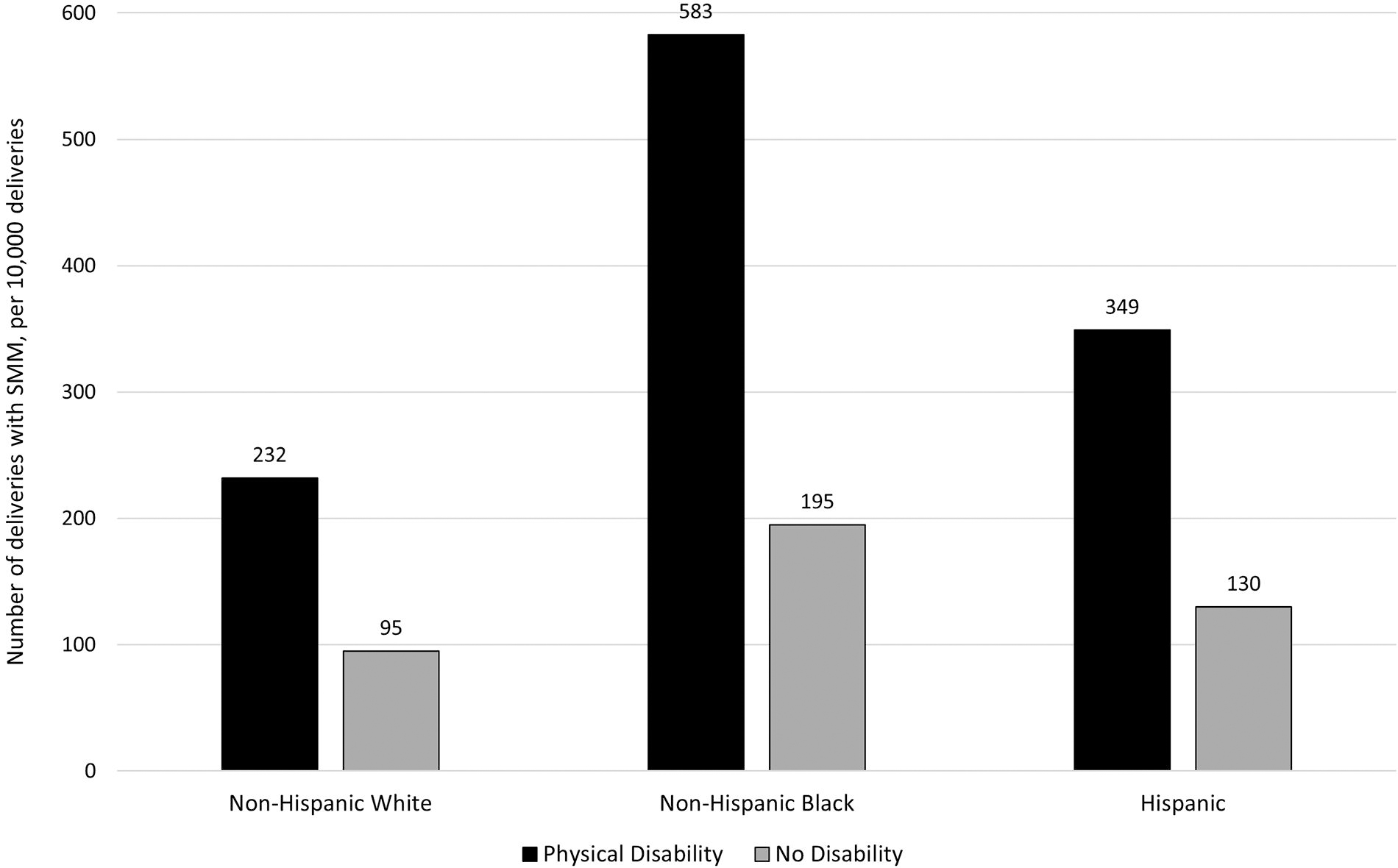
Deliveries per 10,000 with at least one indicator of severe maternal morbidity (SMM), by race, ethnicity, and disability status; California, 2008–2020.
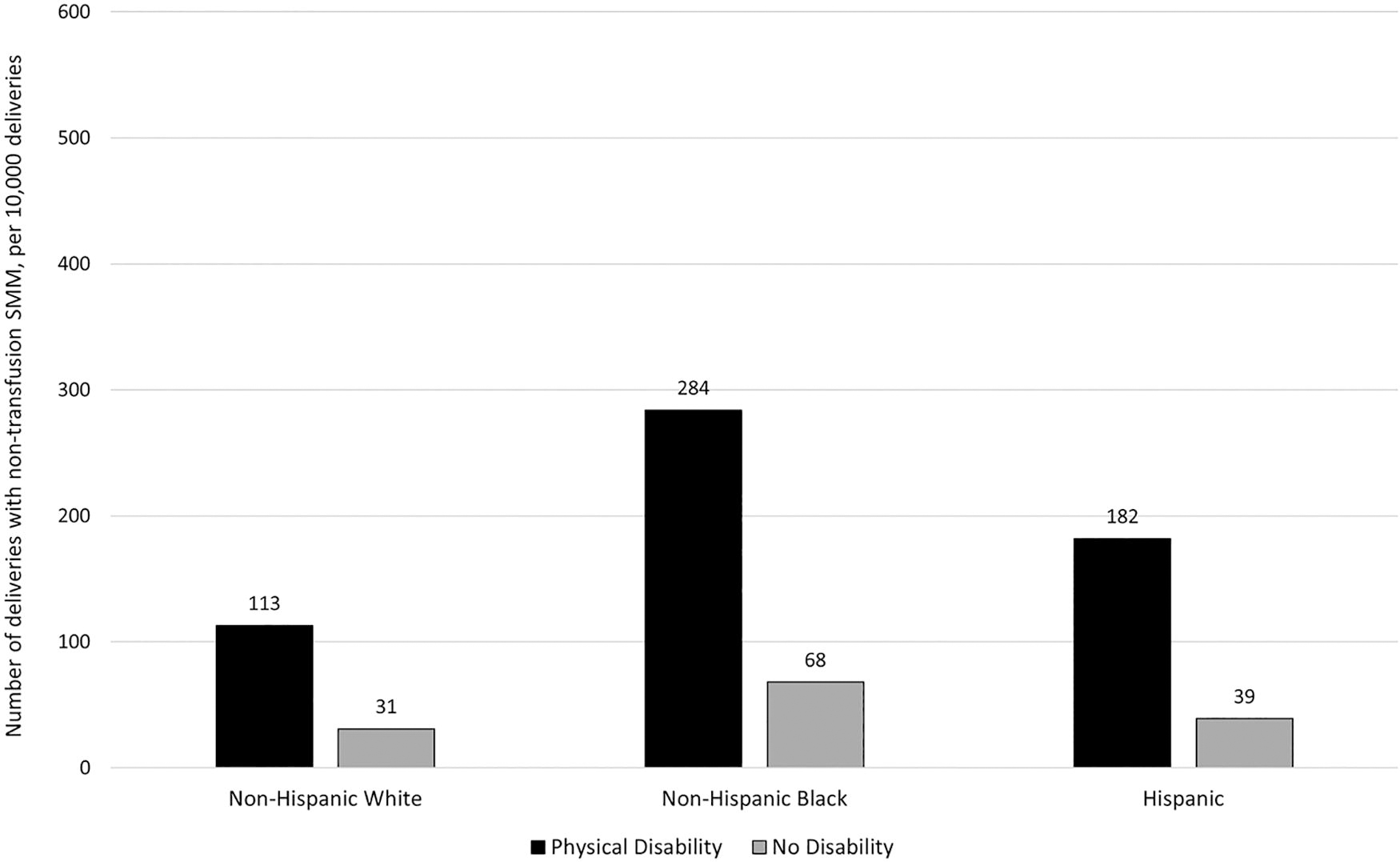
Deliveries per 10,000 with at least one nontransfusion indicator of severe maternal morbidity (SMM), by race, ethnicity, and disability status; California, 2008–2020.
Each of our secondary outcomes was more prevalent among birthing patients with physical disabilities than among those without disabilities in the same racial or ethnic group (Table 2). For most outcomes, prevalence was highest among disabled Black patients, followed by disabled Hispanic patients. However, gestational diabetes was more common among disabled Hispanic patients (12.7%), whereas mental health disorders were most common among disabled White patients (16.8%).
Prevalence of Perinatal Complications and Outcomes by Race, Ethnicity, and Disability Status; California, 2008–2020
Chi-square test.
In our unadjusted regression models, RR of any SMM among Black patients with physical disability was more than six times greater than the risk in the reference group of non-Hispanic White patients without disabilities (RR = 6.13, 95% CI: 4.94, 7.61). Risk of SMM among Hispanic patients with physical disability was approaching four times that of the reference group (RR = 3.67, 95% CI: 3.29, 4.10). Both of these estimates were higher than the RR among non-Hispanic White patients with physical disability (RR = 2.44, 95% CI: 2.16, 2.77). They were also markedly higher than RRs among nondisabled Black patients (RR = 2.05, 95% CI: 1.99, 2.11) and nondisabled Hispanic patients (RR = 1.36, 95% CI: 1.34, 1.39). For disabled Black birthing persons, risk of SMM was substantially larger than the sum of the risks for nondisabled Black and disabled White birthing persons. Similar patterns were apparent for nontransfusion SMM, with risks among disabled birthing persons even more pronounced, particularly for those who were Black or Hispanic (Table 3).
Unadjusted Relative Risks (with 95% Confidence Intervals) of Severe Maternal Morbidity and Other Perinatal Complications by Race, Ethnicity, and Disability Status; California, 2008–2020
SMM, severe maternal morbidity.
Unadjusted RRs for all but two of our secondary outcomes were largest for disabled Black birthing persons (Table 3). Risk of gestational diabetes was highest among disabled Hispanic birthing persons (RR = 1.78, 95% CI: 1.68, 1.88), and risk for mental health disorders was highest among disabled White birthing persons (RR = 2.71, 95% CI: 2.60, 2.82). For several of the complications and outcomes we examined, CIs of the estimates for multiply marginalized birthing persons did not overlap with those for nondisabled people in the same racial or ethnic group or those for disabled non-Hispanic White patients. Specifically, risk estimates for disabled Black patients were higher than (and did not overlap with) those of disabled White patients and nondisabled Black patients for gestational hypertension, preeclampsia, preterm delivery, early preterm delivery, VTE, chorioamnionitis, and puerperal endometritis. Complications and outcomes for which disabled Hispanic birthing persons had higher risk estimates (with nonoverlapping CIs) than disabled White patients or nondisabled Hispanic patients included preeclampsia, gestational diabetes, preterm delivery, early preterm delivery, and chorioamnionitis.
In our multivariable regression models, estimates of SMM risk were somewhat attenuated but still substantial, especially among disabled Black patients (any SMM: adjusted RR [aRR] = 3.70, 95% CI: 2.99, 4.59; nontransfusion SMM: aRR = 4.03, 95% CI: 2.95, 5.49) and disabled Hispanic patients (any SMM: aRR = 2.93, 95% CI: 2.63, 3.26; nontransfusion SMM: aRR = 3.98, 95% CI 3.41, 4.64). Adjusted RRs for our secondary outcomes were largely consistent with those in our unadjusted analyses, although adjusted risk estimates were typically smaller and there was somewhat more overlap among CIs (Table 4). After propensity score matching, Hispanic birthing persons with physical disabilities had significantly lower risk of endometritis than nondisabled Hispanic people (Supplemental Supplementary Table S3). For most other outcomes, disabled persons were at significantly greater risk than those without disabilities in the same racial or ethnic group, even with propensity score matching.
Adjusted Relative Risks (with 95% Confidence Intervals) of Severe Maternal Morbidity and Other Perinatal Complications by Race, Ethnicity, and Disability Status; California, 2008–2020
Adjusted for maternal age, education, insurance, parity, Kotelchuck index, preterm birth, BMI, chronic hypertension, pre-existing diabetes, smoking during pregnancy, and substance use.
Adjusted for maternal age, education, insurance, parity, Kotelchuck index, BMI, pre-existing diabetes, smoking during pregnancy, and substance use.
Adjusted for maternal age, education, insurance, parity, Kotelchuck index, BMI, chronic hypertension, pre-existing diabetes, smoking during pregnancy, and substance use.
Adjusted for maternal age, education, insurance, parity, Kotelchuck index, BMI, chronic hypertension, smoking during pregnancy, and substance use.
SMM, severe maternal morbidity; BMI, body mass index.
Discussion
This study builds on prior research indicating that birthing persons with physical disabilities are at greater risk for perinatal complications than those without disabilities. 3 –6 We found similar patterns of increased risk among physically disabled birthing persons, and we were able to provide further detail by considering the intersection with race and ethnicity. Our findings suggest that disadvantages associated with physical disability and race or ethnicity may be cumulative, leading to exacerbation of perinatal health risks for people with multiple marginalized identities. Disparities between birthing persons with and without disabilities were larger in minoritized racial and ethnic groups, and racial and ethnic disparities were magnified among those with physical disabilities. In particular, we found substantially greater risk of SMM when physical disability and minoritized race or ethnicity were both present. Black and Hispanic birthing persons with physical disabilities had more than six times and nearly four times the risk of SMM, respectively, as nondisabled White birthing persons. Risk was significantly elevated but less pronounced for disabled White birthing persons and nondisabled Black and Hispanic birthing persons.
For disabled Black birthing persons in particular, we found increased risk of SMM above and beyond what would be expected based on risks associated with race alone and disability alone. If added together, the excess risk of SMM we observed for Black versus White birthing persons (among those without disabilities) and the excess risk for disabled versus nondisabled birthing persons (among non-Hispanic White patients) would be notably less than the total excess risk we observed among disabled Black birthing persons. In other words, Black people with physical disabilities appear to experience all the increased risks of SMM associated with both race and disability, plus an additional layer of disparity associated with the intersection of the two. This echoes a pattern first reported decades ago with regard to employment among disabled Black women 22 and suggests that racism and ableism may act synergistically to intensify inequities.
Though not as pronounced as the risk of SMM, findings for many of our secondary outcomes also suggested some compounding of disparities. We found that Black birthing patients with physical disabilities had higher risk of gestational hypertension, preeclampsia, preterm delivery, early preterm delivery, VTE, chorioamnionitis, and puerperal endometritis than White patients with physical disabilities and Black patients without disabilities. Hispanic birthing persons with physical disabilities were at increased risk of preeclampsia, gestational diabetes, preterm delivery, early preterm delivery, and chorioamnionitis compared with non-Hispanic White persons with physical disabilities and Hispanic persons without disabilities. These findings are consistent with and expand on existing literature. For example, prior research has found increased risk of gestational diabetes, preeclampsia, VTE, and preterm birth among women with physical disabilities. 5,6,23,24 Similarly, multiple studies have found increased risk of perinatal complications and adverse outcomes among Black and Hispanic birthing people. 25,26 Our study bridged these two separate bodies of literature by examining disability in combination with race and ethnicity and finding even greater disparities at these intersections.
Our findings point to an urgent need to better understand the underlying causes of SMM and other perinatal complications and develop policies and practices to prevent these complications and eliminate disparities in outcomes. Studies of preconception health among women with disabilities have found greater prevalence of tobacco use, obesity, chronic conditions such as asthma and diabetes, experiences of violence, and inadequate social support as compared with women without disabilities. 13,27 –29 These characteristics and experiences may contribute to increased risk of perinatal complications and adverse outcomes. We were able to adjust for some of these sociodemographic and clinical characteristics in our multivariable analyses, and significant associations of physical disability and race and ethnicity with perinatal complications remained. Further research is needed to examine the role of additional risk factors, including the extent to which differences in perinatal complications and outcomes may be driven by systemic racism and ableism.
The results of our study suggest that, when patients with physical disabilities present for perinatal care, clinicians should be particularly attentive to identifying and treating medical conditions that could contribute to serious complications and adverse outcomes. Such attention is especially warranted for Black and Hispanic birthing persons with physical disabilities. That said, clinicians and patients should not assume that all pregnancies among people with physical disabilities are necessarily high risk. Although RRs were greater for people with physical disabilities—especially those who were Black or Hispanic—compared with non-Hispanic White patients without disabilities, the absolute risk of most of these conditions was still small. However, clinicians do need to be aware of the possible risks and be prepared to address complications promptly if they occur.
The one outcome we examined that was not rare was cesarean delivery, which was utilized in more than 40% of deliveries among disabled people. Although it may be required for some births, cesarean surgery increases risk of complications and makes postpartum recovery more challenging. Prior research suggests that disabled people may be scheduled for cesareans when not medically necessary and without adequate consideration of the possibility for a safe vaginal birth. 30 Clinicians can help address these concerns by discussing delivery options, cesarean indications, and support needs with disabled patients well before their due dates. Support from labor doulas may also be helpful. There is compelling evidence in the general population that doula support can reduce cesarean rates; 31 –33 such support could be especially helpful for disabled people who may need more assistance while laboring. More broadly, delivery teams can facilitate inclusive care by identifying accessibility needs of patients with disabilities and including that information in electronic health records, with alerts to prompt preparation so that accommodations (e.g., sign language interpreter; visit scheduled in room with height-adjustable exam table) are in place for appointments. 34 Relatedly, clinics and health systems should ensure their settings fully comply with the requirements of the Americans with Disabilities Act and federal standards for accessible exam equipment. 35
Our findings also underscore the ongoing need for clinician training in culturally competent and disability competent care. Obstetric clinicians have highlighted the lack of training they received on caring for pregnant people with physical disabilities as a key barrier to providing quality care for this population. 36 Furthermore, clinicians point to a dearth of available evidence and recommendations to guide care of patients with disabilities. 36 Continued research is needed to build a strong evidence base and establish clinical care guidelines for birthing persons with disabilities, especially those in minoritized racial and ethnic groups.
This study has limitations inherent in the nature of the dataset. Our data are from only one state and thus are not representative of the United States as a whole. We were reliant on diagnosis codes for identifying physical disability status, and there is not always a clear link between presence of a diagnosis and the extent to which functioning is impacted. Recent research suggests that diagnosis codes have limited sensitivity and may miss many people with disabilities. 37,38 Moreover, we only had diagnosis codes from the hospital discharge record for the delivery hospitalization, not from birthing patients’ full medical histories. Thus, we likely identified disabilities that were readily apparent and perceived as salient to the course of pregnancy and delivery. Our results may not be generalizable to people with less obvious physical disabilities. Furthermore, it is possible that disabling conditions—especially more minor conditions—are more likely to be coded for some racial and ethnic groups than others, which could introduce selection bias and affect the comparability of physically disabled groups across racial and ethnic categories. Importantly, our data do not allow us to determine the extent to which prenatal care occurred in the context of a known disability, or examine racial and ethnic differences in clinical management of disabilities and assess how these aspects of care may have impacted outcomes.
We had limited cell sizes for examining certain complications, especially VTE. Previous research has found greater risk of VTE in birthing person with physical disabilities compared with those without disabilities. 23,24 Our results suggest that Black birthing persons with physical disabilities may be at particularly high risk of VTE; however, further research is needed with larger samples of disabled Black birthing persons to confirm this finding. Our analyses were also limited by insufficient sample sizes for examining different categories of physical disability by race and ethnicity. Previous research has found that birthing persons with injuries resulting in physical disability (e.g., spinal cord injury) had especially high risk of SMM, whereas the magnitude of risk was lower among those with physical disabilities due to congenital anomalies. 6 Additional research is needed to examine perinatal complications associated with specific physical disabilities as they intersect with race and ethnicity.
Our study also has important strengths. The large size of our dataset was crucial for analysis of rare outcomes among birthing persons with physical disabilities while stratifying by race and ethnicity. Furthermore, our data represent a complete census (not a sample) of inpatient births in California during the study period. Additionally, the use of vital statistics data allowed us to include socioeconomic and health characteristics in our analyses that were not available from hospital discharge records. Our data also allowed us to determine that the disabilities we identified existed at or near the time of delivery.
Conclusions
Pregnancy complications and adverse outcomes are more likely among birthing persons with physical disabilities, especially those who are Black or Hispanic. We found that risk of SMM was substantially higher among Black and Hispanic birthing persons with physical disabilities than among those with any other combination of disability status and race or ethnicity. Our findings highlight the need to address inequities and identify strategies to prevent, identify, and promptly address SMM and other perinatal complications among disabled birthing persons in minoritized racial and ethnic groups.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under award #R01HD105712 and by the National Institute for Disability, Independent Living, and Rehabilitation Research in the Administration for Community Living under award #90DPHF0011. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Administration for Community Living. The funding agencies had no involvement in study design, data analysis, or interpretation.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.