
Abstract
Introduction:
Toileting behaviors are recognized as potential contributors to lower urinary tract symptoms (LUTS) in women. This study examines the association between toileting behaviors and LUTS among community-dwelling women and whether age modifies these associations.
Methods:
Cross-sectional analyses were conducted using baseline data from a population-based cohort study, RISE FOR HEALTH (RISE). Women completed validated questionnaires assessing toileting behaviors (Toileting Behaviors-Women’s Elimination Behaviors scale) and LUTS (10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index [LURN SI-10]). Toileting behaviors included place preference for voiding, premature voiding, delayed voiding, straining to void, and toileting position. LUTS items included urine storage, emptying, and postmicturition symptoms. Associations were analyzed by proportional odds logistic regression. Analyses were stratified by seven age groupings.
Results:
Data from 2,327 women (mean age 51.1 years, standard deviation = 18.2) were analyzed. Delayed voiding was most strongly associated with the LURN SI-10 composite score (odds ratio [OR] 1.89; 95% confidence interval [CI]: 1.72, 2.09) and urgency incontinence (OR 1.87; 95% CI: 1.66, 2.10). Premature voiding showed the strongest association with urgency (OR 1.82; 95% CI: 1.68, 2.04). Straining was strongly associated with emptying symptoms, including delay before urine starts (OR 2.28; 95% CI: 2.05, 2.54) and slow stream (OR 2.28; 95% CI: 2.05, 2.53). Age modified associations between delayed voiding and LUTS, with strongest associations among 18- to 25 year-old women.
Conclusions:
Premature voiding, delayed voiding, and straining showed the strongest associations with LUTS in this cross-sectional analysis. Longitudinal studies are needed to clarify the directionality of these associations. Educating young women on healthy toileting habits may mitigate potential effects of unhealthy toileting behaviors on bladder health.
Introduction
Lower urinary tract symptoms (LUTS), including urinary urgency, frequency, and urinary incontinence, are common and affect the lives of millions of women of all ages. 1 There is an extensive body of epidemiological literature identifying risk and protective factors for LUTS, particularly incontinence. 1 Several risk factors are well established, including greater age and vaginal parity, as well as chronic health problems such as obesity, diabetes, and neurological conditions. Although the established factors help to identify at-risk populations, many are not modifiable, limiting their usefulness in preventing LUTS.
Less is known about the role of women’s voiding practices that are potentially modifiable and may influence risk of LUTS. Toileting behaviors increasingly are recognized as potential contributors to bladder health. These behaviors involve decisions about when and how often to void, how long to delay voiding (holding), where to void, use of muscular effort to void (straining), and positions assumed to void. 2 Toileting behaviors often are learned in childhood but often change based on observation of others later in life. 3 They may be influenced by social expectations and toileting environments, 4,5 restricted by school and work rules, 4 or adopted in response to existing LUTS. Toileting practices and preferences vary across cultures 6,7 ; for example, sitting toilets are the norm in the United States and in Western cultures, whereas squat toilets are common in other parts of the world. Although U.S. women usually sit down to void at home, when away from home, concerns about cleanliness often prompt women to delay voiding or assume non-sitting voiding positions (e.g., hovering, squatting, standing) to avoid contact with toilet seats. 8
Toileting behaviors can potentially influence the prevalence or worsening of LUTS through various mechanisms. For example, chronic delayed voiding may lead to reduced bladder sensation, bladder hypertrophy, impaired bladder control, 9,10 as well as neural reflex changes that make the bladder more sensitive to stretch, leading to involuntary bladder contractions. 11 When delaying voiding, women may not be able to relax their pelvic floor muscles, leading to bladder emptying symptoms such as urinary hesitancy. A habit of frequent urination (voiding “just in case”) can lead to loss of ability to accommodate increasing urine volumes, resulting in urgency, reduced bladder capacity, and more frequent voiding. 12 Although straining is common in women both with and without LUTS, the timing and degree of straining have been suggested to contribute to LUTS in different ways. Straining at the start of urination, before a bladder contraction occurs, leads to increased pelvic floor activity and development of dysfunctional voiding. It then becomes difficult to properly relax the pelvic floor muscles to void efficiently. 13,14 Habitual straining may weaken or damage pelvic floor muscles and contribute to urinary incontinence over time. In the setting of an underactive bladder or weak bladder contractions, straining may be a compensatory mechanism to initiate and maintain voiding. 15 Both the direction of the relationship between toileting behaviors and bladder symptoms and the causal mechanisms remain poorly understood. A first step in understanding the potential impact of toileting behaviors and the mechanisms through which they lead to LUTS is to identify associations between them.
There is limited research examining women’s specific toileting behaviors in relation to LUTS. 16 In one study, a community-based sample of primarily White and college-educated adult women (n = 6,695) was electronically recruited from a national research registry to complete validated questionnaires assessing toileting behaviors and urinary symptoms. Participants reporting bladder problems on the Patient Perception of Bladder Condition questionnaire and overactive bladder symptoms on the International Consultation on Incontinence Questionnaire—Overactive Bladder module were more likely to report delayed voiding, straining to void, premature (or convenience) voiding, and altered voiding position (hovering, squatting). 17 Similarly, in a sample of 316 adult women, significant associations were found between several LUTS and premature voiding, delayed voiding, straining to void, and non-sitting voiding positions when away from home. 18 Other studies have reported similar relationships between various toileting behaviors and LUTS in selected populations, including older women, 19 physicians and medical students, 20 nurses and advanced practice providers, 21 –24 teachers, 25 pregnant women, 26 nonpregnant women working in academic medical centers, 27 and full-time working women in various occupations. 28 These smaller studies with specific populations offer some insight into the associations between toileting behaviors and LUTS, but larger studies with more heterogeneous samples of women would offer the opportunity to generalize findings and consider population based interventions.
We analyzed data from RISE, a large, regionally representative study of women residing in the United States, conducted by the Prevention of Lower Urinary Tract Symptoms (PLUS) Research Consortium. Our approach was informed by the PLUS conceptual framework, 29 which examines behavior and biology within a social ecological context, including the idea that bladder health may be shaped by cumulative experiences and behaviors across the life course. We describe (1) the association between toileting behaviors (place preference, premature voiding, delayed voiding, straining, and non-sitting toilet position) and specific LUTS and a LUTS composite score and (2) if and how age modifies associations between toileting behaviors and LUTS. We hypothesized that specific toileting behaviors (premature and delayed voiding) would be most strongly associated with storage LUTS of urgency and incontinence and that straining would be most strongly associated with emptying LUTS (e.g., slow urine stream). Based on the life course concept of cumulative risk, we hypothesized that the association between toileting behaviors and LUTS would strengthen and with age.
Methods
Study population and design
RISE is an ongoing institutional review board–approved cohort study of adult women, designed to inform factors that contribute to bladder health and prevent LUTS across the life course. The RISE study methods and recruitment have been described previously. 30 Eligible RISE participants were 18 years of age or older, born as female or identified as a woman, and were community-dwelling (non-institutionalized) living in 50 counties surrounding the eight PLUS recruitment sites (University of Alabama, Loyola University Chicago, University of California San Diego, University of Michigan, University of Minnesota, University of Pennsylvania, Washington University, Yale University). 30 Baseline data were collected between May 2022 and December 2023. Participants completed two 30-minute baseline surveys (electronic or mailed paper) separated by a mean of 2.0 weeks (standard deviation [SD] 2.7). LUTS and toileting behavior items were assessed in the first and second baseline surveys, respectively. The response rate to the first baseline survey was 7.9% among invitations sent to valid mailing addresses, and the retention rate for the second baseline survey was 79.4%. The present analysis was limited to cisgender women who provided complete information on both the toileting behaviors and LUTS questionnaires. Excluded were women with incomplete surveys (n = 884) and women who were pregnant (n = 31) or had medical conditions that could affect bladder function or toileting (multiple sclerosis [n = 20], brain or spinal cord injury [n = 36], spina bifida [n = 4], genitourinary cancers [n = 5], neurogenic bladder [n = 19], cystectomy [n = 1], and current, prolonged or intermittent catheter use [n = 14]).
Measures
Toileting behaviors were assessed using the Toileting Behaviors-Women’s Elimination Behaviors scale (TB-WEB). 31 Validated in women 18 years of age and older, 24,31,32 the TB-WEB consists of items in five domains designed to measure women’s toileting behaviors when at home and while away from home. Domains include place preference for voiding, premature voiding, delayed voiding, straining, and toileting position at home and away from home. 31 A 5-point Likert scale was used to assess the frequency of each behavior (1 = Never, 2 = Rarely, 3 = Sometimes, 4 = Often, 5 = Always). Domain scores for the first four toileting behaviors were calculated by averaging responses across domain items. Toileting position away from home was assessed through four questions regarding the frequency of each of four toileting positions (sit, crouch, squat, stand) on a 5-point scale. Toileting position away from home was categorized as “Sit” if the highest value when comparing the four positions was for sitting, and the value was “Often” or “Always”; “Mixed” if the highest value endorsed was the same for sitting as for another position 18 ; and “Other” when a position other than sitting had the highest value.
LUTS were assessed using the 10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index (LURN SI-10). 33 This instrument was designed to measure the presence and frequency of 10 LUTS over a 7-day recall period, including daytime urinary frequency, nighttime urinary frequency, urgency, urgency urinary incontinence (UUI), stress urinary incontinence (SUI), hesitancy or delay before urine starts, slow or weak urinary stream, dribbling after urination, and pain or discomfort with bladder filling. A 5-point Likert scale was used to assess the frequency of LUTS (0 = Never, 1 = Rarely, 2 = About half the time, 3 = Most of the time, 4 = All of the time). Frequencies of urination were examined as categorical for daytime voiding frequency (less than 3 times, 4–7 times, 8–10 times, 11 or more times/day) and nighttime voiding frequency (0, 1 time, 2–3 times, more than 3 times/night). The total LURN SI-10 score reflects the summed responses for each of the 10 LUTS items (range: 0–38), with higher scores indicating a greater number and frequency of LUTS.
Statistical analyses
We calculated the mean and standard deviation of four of the TB-WEB domain scores (place preference for voiding, premature voiding, delayed voiding, straining to void). The means and standard deviations for these domains are shown, as well as the number and percentage of participants who reported different toilet positions by response options for each LURN SI-10 item and by quartile of the LURN SI-10 total score. Differences in the distribution of TB-WEB scores by LUTS items were evaluated using Kruskal–Wallis tests (preference for voiding, premature voiding, delayed voiding, straining to void) and chi-square tests (toilet position away from home). Proportional odds logistic regression models were used to estimate associations between TB-WEB scores and LUTS, adjusted for age category of participants. Age categories (18–25, 26–34, 35–44, 45–54, 55–64, 65–74, and 75+ years) were delineated by the PLUS Consortium to reflect both biological events and social ecological contexts related to the lower urinary tract across the female life course. 29 To examine whether associations between toileting habits and LUTS varied by age, analyses stratified by age category also were performed.
Results
Population
The study population consisted of 2,327 cisgender women, mean age 51.1 years (SD 18.2, range 18–101 years). Of the 3,341 participants recruited for RISE, 884 were excluded for incomplete surveys, and an additional 130 were excluded due to pregnancy (n = 31) or medical conditions that could affect bladder function or toileting (n = 99). Participants self-reported their ethnic and racial background in the following categories: 62.9% Non-Hispanic White, 14.5% Hispanic, any race, 12.2% Non-Hispanic Black, 5.0% Non-Hispanic Asian, 3.2% another racial identity, and 2.1% multiple racial identities. Over 45% of the sample were employed full-time, 14.1% were employed part-time, and 90.3% of the sample had an annual household income above the federal poverty line. With respect to factors that may affect toileting behaviors, 4.5% required assistance to use the toilet (see Supplementary Table S1).
Toileting behaviors and LUTS
Tables 1 and 2 show distributions of TB-WEB domain scores by responses to each LURN SI-10 item and by quartiles of the LURN SI-10 composite score. Mean scores for the place preference domain were the highest and corresponded to a value between “sometimes” and “often,” those for delayed voiding corresponded to values between “rarely” and “sometimes,” and those for premature voiding and straining corresponded to values close to “rarely.” Almost all TB-WEB domain scores were associated with higher frequency of LUTS and greater LURN SI-10 scores. Associations between toilet position away from home and most LURN SI-10 items were null (Table 2) with one exception: “Other” toilet position besides sitting when away from home was associated with infrequent daytime urination (≤3 times/day).
Distributions of TB-WEB Behavioral Domain Scores by LURN-10 Individual Items and Composite Score a
TB-WEB domain scores in this table are continuous. Means and standard deviations are shown. A 5-point Likert scale (1–5) was used to assess frequency of each toileting behavior; domain scores were calculated by averaging responses across each domain.
The distribution of a given TB-WEB behavioral domain differed across levels of an individual LURN-10 item or quartiles of the LURN-10 composite score at p < 0.0001.
p < 0.01.
p < 0.001.
LURN-10, 10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index; M, mean; SD, standard deviation; TB-WEB, Toileting Behaviors-Women’s Elimination Behaviors scale.
Distribution of Women Endorsing Specific TB-WEB Toileting Positions a by LURN SI-10 Individual Items and Composite Score
All values are row percentages.
LURN-10, 10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index; TB-WEB, Toileting Behaviors-Women’s Elimination Behaviors scale.
Table 3 shows age-adjusted associations between the TB-WEB domain scores and select LURN SI-10 items of greatest clinical importance (urgency and UUI) due to their high prevalence and those with a strong theoretical association with certain toileting behaviors (delay before urine starts and slow or weak stream). The LURN SI-10 score is included as a measure of symptom burden. Delayed voiding and premature voiding showed the strongest associations with storage symptoms of urgency and UUI, whereas straining showed the strongest association with emptying symptoms. For example, each 1-unit increase in the delayed voiding composite score was associated with 87% greater odds of UUI. Straining was associated with twice the odds of having a delay before urine starts and of having a slow or weak stream.
Proportional Odds Logistic Regressions of Select LURN-10 Items on TB-WEB Domain Scores, Adjusted for Age a
Statistically significant findings (p < 0.05) are bolded.
With the exception of toileting position when away from home, TB-WEB domain scores are continuous. TB-WEB domain scores were entered in separate regression analyses, adjusting for age.
CI, confidence interval; LURN-10, 10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index; OR, odds ratio; TB-WEB, Toileting Behaviors-Women’s Elimination Behaviors scale.
Age-adjusted associations between the TB-WEB behavioral domain scores and LURN SI-10 composite score quartiles are shown in Table 3. Place preference for voiding, premature voiding, delaying voiding, and straining were all associated with a greater likelihood of reporting worse LUTS (i.e., a greater number of LUTS and worse LUTS), as indicated by quartile group. The toileting behavior with the greatest effect on the LURN SI-10 composite score was delayed voiding (odds ratio [OR] 1.98; 95% confidence interval [CI]: 1.72, 2.09).
With few exceptions, associations between toileting behaviors and voiding frequency (daytime and nocturia) were generally weaker than the associations between toileting behaviors and other LUTS (Supplementary Table S4). A notable exception was the strong association between premature voiding and voiding 11 or more times versus 4–7 times per day (OR 2.25; 95% CI: 1.79, 2.83) and nocturia 3 or more times versus 0 (OR 2.10; 95% CI: 1.68, 2.62).
Similar to unadjusted analyses, toileting behaviors (place preference, premature voiding, delayed voiding, straining) were associated with worse LUTS in adjusted analyses, with the exception of toilet position away from home. Associations between TB-WEB domain scores and all LURN SI-10 items are shown in Supplementary Tables S2, S3 and S4.
Delayed voiding and premature voiding were both associated with various LURN SI-10 symptoms (Table 3 and Supplementary Tables S2 and S3). The overlap between the two groups was small: of the 30% of women who reported delayed voiding “Often” or “Always,” only 15% of that group reported premature voiding “Often” or “Always.”
Age, toileting behaviors, and LUTS
To determine if one or more age-groups had a greater tendency toward LUTS based on their toileting behaviors, potential interactions between age and TB-WEB domains were examined. Most interaction effects were nonsignificant. However, significant (p ≤ 0.05) and borderline significant (p ≤ 0.1) interactions between age and delayed voiding were observed in relation to several LURN SI-10 items and the LURN SI-10 composite score quartile (Supplementary Appendix Tables A1, A2).
Across all age-groups, delayed voiding was significantly associated with urgency, UUI, delay before urine starts, and a weak stream (Table 4). The ORs for women in the youngest 18- to 25-year age-group were highest across all LUTS outcomes (Supplementary Appendix Tables A1, A2) and suggest that women in this age-group who delay voiding are at least twice as likely to experience symptoms. The OR for UUI for the youngest women was 5.97 (95% CI: 3.21, 11.10), indicating that younger women who engage in delayed voiding were nearly 6 times more likely to experience UUI than those who do not delay voiding. The strength of the association between delayed voiding and storage LUTS of urgency and UUI gradually decreased across age-groups as shown in Table 4. Forest plots in Figure 1 show a trend of decreasing ORs with increasing age for several LUTS outcomes, suggesting that the impact of delayed voiding may attenuate with age. The LURN SI-10 composite score showed the strongest association with delayed voiding in younger women (OR 2.91; 95% CI: 2.09, 4.05). The association weakened between ages 26 and 54 years and strengthened somewhat between ages 55 and 74 years as shown in Figure 1. With the exception of urgency, UUI and stress incontinence with cough laugh or sneeze, other LUTS and the LURN SI-10 composite score were not significantly associated with delayed voiding in the oldest age group (Supplementary Appendix Tables A1, A2 and A3).
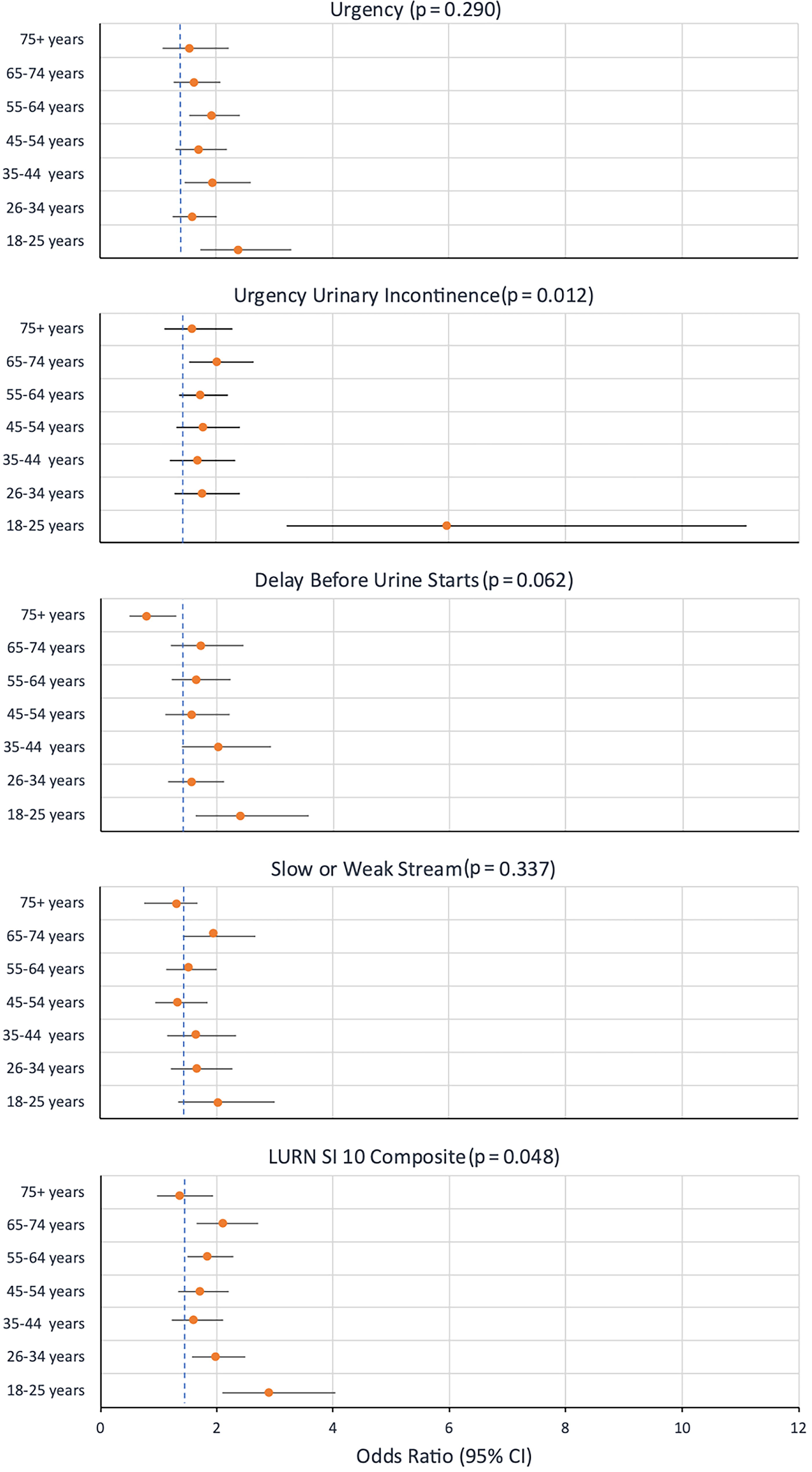
Age-specific associations between delayed voiding and select LUTS: Odds ratios (95% CI) and interaction p-values across select LURN SI-10 outcomes and composite score. CI, confidence interval; LURN SI-10, 10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index; LUTS, lower urinary tract symptoms.
Proportional Odds Logistic Regressions of Select LURN-10 Items on the TB-WEB Domain Score, Delayed Voiding Toileting Behavior, Within Age-Group a
Statistically significant findings (p < 0.05) are bolded.
Interaction effect (p-value) between age and delayed voiding on select LURN SI-10 outcomes and composite score, significant findings are bolded, where p-value <0.05.
CI, confidence interval; LURN SI-10, 10-item Lower Urinary Tract Dysfunction Research Network—Symptom Index; OR, odds ratio; TB-WEB, Toileting Behaviors-Women’s Elimination Behaviors scale.
Discussion
This analysis examined associations between toileting behaviors and LUTS in a large, population-based sample of U.S. cisgender adult women. Four toileting behaviors (place preference for voiding, premature voiding, delayed voiding, and straining) were consistently associated with different types of LUTS and a higher LURN SI-10 composite score. Premature voiding and delayed voiding behaviors were both associated with the greatest odds of storage LUTS. Only a small portion of women endorsed both of these seemingly contradictory behaviors on a habitual basis, suggesting that each behavior poses risk, potentially through different mechanisms, and raises the need for further research to clarify these behaviors in this subset of women. Straining was associated with the greatest odds of bladder emptying symptoms. Similar to a study by Wan and colleagues, 23 our research found that toileting position away from home was less consistently associated with LUTS.
Similar to other studies, the place preference mean score was high 17,18,20,34 ; however, its association with LUTS was weaker than for other toileting behavior domains. In our sample, within the place preference domain, a highly endorsed item was “When I use public toilets, I worry about how clean they are.” We speculate that while their “worry” may be high, thoughts of worry may not be associated with a habitual behavior.
An unexpected finding was that women in the youngest age-group who delayed voiding had the highest odds of reporting specific LUTS, compared with women in their age-group who did not delay voiding. The effect size for UUI (OR 5.97) stands out as particularly high. The reasons for this finding are unclear, as the mechanisms linking delayed voiding to such a high risk for LUTS in young women remain unknown. Our result suggests a particular vulnerability in young women to this symptom. Other studies have identified high levels of delayed voiding in young women. In a study of young women, mean age of 21.6 years, avoidance of public toilets, and delayed voiding were common behaviors and were significantly related to the presence of LUTS. 34 Additionally, a large study of young female nurses (mean age 31 years) demonstrated that more than half experienced LUTS, with delayed voiding being the most common unhealthy toileting behavior. 21,22 Further research is needed to explore whether behavioral or contextual factors unique to this age-group may influence these associations. If longitudinal research shows that delayed voiding is associated with LUTS, young women may be a population of interest for education and interventions aimed at preventing delayed voiding and promoting healthy toileting behaviors.
The direction of association between toileting behaviors and LUTS cannot be determined through this cross-sectional study design. Long-standing toileting habits may contribute to the development of LUTS through various mechanisms. For example, a habit of premature voiding may lead to loss of ability to accommodate increasing volumes of urine, which, over time, may lead to decreased functional bladder capacity, resulting in increased urgency and more frequent voiding. 11 Habitually delaying voiding may lead to impaired bladder sensation, bladder overactivity, and altered bladder compliance. 9,10 Habitually straining to urinate, particularly without a detrusor contraction, can stress the pelvic floor muscles potentially leading to weakness, pelvic floor dysfunction, and SUI. 13,35 On the contrary, women with existing LUTS may adopt certain toileting behaviors to manage symptoms, and some associations may be bidirectional. The high ORs for the association between bladder emptying symptoms and straining may reflect a bidirectional relationship and the creation of the feedback loop that increases both the toileting behavior and the symptom. For example, straining in the absence of LUTS over time may lead to pelvic floor dysfunction increasing the risk for emptying LUTS. As symptoms worsen, the need for straining to empty becomes greater. Longitudinal studies are needed to explore the directionality of associations between toileting behaviors and LUTS.
Previous studies have demonstrated that certain voiding behaviors can be situational. For example, delayed voiding may occur in occupational settings due to job demands, 17,18 in spaces where women avoid unclean bathrooms, 36 or in situations of real or perceived limitations. 4,8 Teaching women to delay voiding, referred to as bladder training with urge suppression, is utilized widely as a treatment strategy in women with overactive bladder (OAB) and UUI to decrease leakage episodes and urgency symptoms. 37,38 Future studies of the association between toileting behavior and LUTS should examine the context of these behaviors. Ecological momentary assessment (EMA), a method involving real-time monitoring and tracking of behaviors in individuals’ natural environments, 39 could be a useful tool for such investigations. Using EMA around toileting decisions could help researchers study how external factors such as physical environment, location, and social context impact toileting behaviors. 40,41
In previous research, women have expressed a desire and need for information about the bladder to anticipate what can go wrong with the bladder and what they can do to prevent or mitigate bladder problems over the life course. 42,43 To develop effective educational interventions and public health messaging for preventing LUTS in women, further research is needed to guide content that promotes bladder health, including healthy toileting behaviors.
Study strengths and limitations
Study strengths include a large heterogenous sample of women with ages spanning the life course and sociodemographic characteristics that reflect the diversity of the U.S. population. More older women and a broader age range of women are represented than in other similar studies. 5,17 Deliberate measures were taken to promote the participation of women who mirrored the U.S. population with respect to racial identity and Hispanic ethnicity. Validated questionnaires were used to measure toileting behaviors and LUTS.
Our study may have attracted more women with bladder health concerns who opted to participate and remain in the study because of their own experience and interest in the topic. Mitigating this concern is the comparable prevalence of LUTS observed in the RISE sample 44 to that and other population-based studies of women. 45,46 The response rate to the RISE survey was low (7.9%) although consistent with other cold mailed surveys. 47 Methodologic studies indicate that even significant declines in response rates have little effect on final sample estimates, suggesting that nonresponse bias is not directly correlated with nonresponse rate. 48 Other limitations of this study include a low response rate from individuals with less than a college degree and lower incomes. The generalizability of these findings is limited to similar toilet-based cultures.
The cross-sectional nature of this study does not allow us to determine if toileting behaviors cause symptoms, if symptoms lead women to engage in various toileting behaviors, or if both directions of causality exist.
Key contextual factors that may influence toileting behaviors were not included in this study. These include characteristics of the toilet environment such as cleanliness, privacy, safety, and availability of supplies to support hygiene 5,38 ; employment status; rules or policies that restrict toilet access either at work or in public spaces; and cultural norms that may impact toileting behaviors. 6,7 The PLUS Consortium plans to conduct analyses exploring the association of toilet access and the toilet environment on toileting behaviors and LUTS, as well as longitudinal studies exploring the trajectory of LUTS and the relationship between toileting behaviors and LUTS. The present study serves as a starting point for future study.
Conclusions
This analysis found that four toileting behaviors (place preference for voiding, premature voiding, delayed voiding, and straining) were significantly associated with LUTS in cisgender women. The strongest associations were between behaviors of premature voiding and delayed voiding and storage LUTS and between straining and LUTS related to bladder emptying. Associations between delayed voiding and LUTS were strongest among young women, suggesting opportunities for specific education around the risks of delayed voiding, and in clinical settings screening women for this particular behavior. Longitudinal studies are needed to investigate whether these findings reflect the effects of toileting behaviors on the development of LUTS, behavioral adaptations to LUTS, or both. Recognizing that there are important contextual factors that may promote or constrain women’s choices around voiding, research is also needed to evaluate potential environmental, social, and cultural barriers to healthy toileting behaviors. Additional research is needed to identify how toileting behaviors may impact voiding and bladder health in populations underrepresented in this study.
Footnotes
Disclaimer
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH).
Authors’ Contributions
Conceptualization, A.B., S.S.B., K.L.B., M.H.P., A.L.S., S.S., J.F.W., and D.K.N.; Data curation, G.M.; Formal analyses, G.M.; Funding acquisition, The Prevention of Lower Urinary Tract Symptoms (PLUS) Research Consortium; Investigation, G.M., A.L.S., and S.S.; Methodology, A.B., S.S.B., K.L.B., G.M., J.F.W., and D.K.N.; Project administration, A.B. and D.K.N.; Software, G.M.; Validation, G.M.; Visualization, A.B., S.S.B., and G.M.; Writing — original draft, A.B., S.S.B., K.L.B., T.H.L., A.L.S., S.S., and B.R.W.; Writing — review & editing, A.B., S.S.B., K.L.B., S.D.C., S.G., A.S.J., L.K.L., D.Y.L., T.H.L., M.G.M., M.H.P., D.R.-P., A.L.S., S.S., B.R.W., J.F.W., and D.K.N.
Author Disclosure Statement
There are no reported financial conflicts directly related to this work.
Funding Information
This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) at the NIH by cooperative agreements (grants U24DK106786, U01 DK106853, U01 DK106858, U01 DK106898, U01 DK106893, U01 DK106827, U01 DK106908, U01 DK106892, U01 DK126045). Additional funding was received from National Institute on Aging, NIH Office of Research on Women’s Health.
PLUS Research Consortium
Research Centers and Investigators
Loyola University Chicago–Maywood, IL (U01DK106898)
Multi-Principal Investigators: Linda Brubaker, MD; Colleen Fitzgerald, MD, MS
Investigators: Marian Acevedo-Alvarez, MD; Cecilia T. Hardacker, MSN, RN, CNL; Jeni Hebert-Beirne, PhD, MPH
Northwestern University–Chicago IL (U01DK126045)
Multi-Principal Investigators: James W. Griffith, PhD; Kimberly Sue Kenton, MD; Melissa Simon, MD, MPH
Investigators: Oluwateniola Brown, MD; Julia Geynisman-Tan, MD; Margaret G Mueller, MD
University of Alabama at Birmingham–Birmingham, AL (U01DK106858)
Multi-Principal Investigators: Alayne D. Markland, DO, MSc; Camille P. Vaughan, MD, MS
Investigators: Tamera Coyne-Beasley, MD, MPH, FAAP, FSAHM; Kathryn L. Burgio, PhD; Cora E. Lewis, MD, MSPH; Gerald McGwin, Jr., MS, PhD; Beverly Rosa Williams, PhD
University of California San Diego–La Jolla, CA (U01DK106827)
Principal Investigator: Emily S. Lukacz, MD; D. Yvette LaCoursiere, MD, MPH
Investigators: Sheila Gahagan, MD, MPH; Jesse Nodora, DrPH
University of Michigan–Ann Arbor, MI (U01DK106893)
Principal Investigator: Lisa Kane Low, PhD, CNM, FACNM, FAAN
Investigators: Janis M. Miller, PhD, APRN, FAAN; Abby Smith, PhD
University of Minnesota (Scientific and Data Coordinating Center)–Minneapolis MN (U24DK106786)
Multi-Principal Investigators: Gerald McGwin, Jr., MS, PhD; Kyle D. Rudser, PhD
Investigators: Sonya S. Brady, PhD; Cynthia S. Fok, MD, MPH; Bernard L. Harlow, PhD; Peter Scal, PhD; Todd Rockwood, PhD
University of Pennsylvania–Philadelphia, PA (U01DK106892)
Multi-Principal Investigators: Diane K. Newman, DNP; Ariana L. Smith, MD
Investigators: Amanda Berry, PhD, MSN, CRNP; Andrea Bilger, MPH; Terri H. Lipman, PhD; Heather Klusaritz, PhD, MSW; Ann E. Stapleton, PhD; Jean F. Wyman, MD, PhD
Washington University in St. Louis–Saint Louis, MO (U01DK106853)
Principal Investigator: Siobhan Sutcliffe, PhD, ScM, MHS
Investigators: Aimee S. James, PhD, MPH; Jerry L. Lowder, MD, MSc; Melanie R. Meister, MD, MSCI
Yale University–New Haven, CT (U01DK106908)
Principal Investigator: Leslie M. Rickey, MD, MPH
Investigators: Deepa R. Camenga, MD, MHS; Shayna D. Cunningham, PhD, MHS
Steering Committee Chair: Linda Brubaker, MD. UCSD, San Diego. (January 2021– present)
NIH Program Office: National Institute of Diabetes and Digestive and Kidney Diseases, Division of Kidney, Urologic, and Hematologic Diseases, Bethesda, MD
NIH Project Scientist: Jenna Norton, PhD, MPH.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Appendix Table A1
Supplementary Appendix Table A2
Supplementary Appendix Table A3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.