
Abstract
Background:
The United States is proposing to ban menthol cigarettes. Our objective is to examine the extent of menthol smoking among pregnant women and its association with their health.
Methods:
Nationally representative study of 14,226 pregnant women aged 18–44 years using the 2004–2022 National Survey on Drug Use and Health. Multivariate regressions estimate the association between menthol smoking and emergency department (ED) and office visits, poor health, mental health, and smoking cessation.
Results:
In total, 7.0% of pregnant women smoked menthol cigarettes, 7.3% smoked nonmenthol, 11.0% recently quit, and 74.7% were nonsmoking. Lesbian/gay/bisexual women had the highest rates: 18.6% menthol and 11.0% nonmenthol. In the third trimester, 10.4% of Black women smoked menthol and 0.6% smoked nonmenthol (p < 0.01), whereas 5.4% of White women smoked menthol and 8.6% smoked nonmenthol (p < 0.01). From 2004 to 2022, maternal smoking decreased from 16.3% to 5.1%. However, the percentage of pregnant smoking women using menthol increased from 47.0% to 60.1%, with the largest increase among Hispanic women from 43.4% to 78.8% (p < 0.05), compared with a rate of 96.1% among Black women and 49.0% for White women. Pregnant women smoking menthol had 1.6 ED annual visits compared with 1.2 ED visits (p < 0.05) for nonmenthol and 0.6 ED visits (p < 0.05) among the nonsmoking. Among those smoking menthol, 73.7% reported mental health issues compared with 64.4% for nonmenthol.
Conclusions:
Women who smoke menthols report worse health compared with those smoking nonmenthol. Policies designed to reduce menthol smoking would improve maternal health, especially for minoritized women and those at higher risk for poor birthing outcomes.
Introduction
The European Union, United Kingdom, Canada, and more than 170 U.S. localities such as Massachusetts, California, and Minneapolis–St. Paul, have banned menthol cigarettes. In October 2023, the Food and Drug Administration submitted its final proposal for banning menthol cigarettes to the White House. 1,2 A recent meta-analysis of 16 studies across Canada, the US, EU, and Brazil estimated that 24% of those smoking menthol cigarettes quit smoking after a menthol ban, while 50% switched to nonmenthol cigarettes, 2% switched to other flavored tobacco products, and 24% continued smoking menthol cigarettes. 3
Very little is known about the impact of menthol bans on maternal smoking and outcomes. However, the potential benefit is likely immense. A federal ban could potentially improve infant outcomes and racial health disparities. At least 5%–8% of preterm deliveries, 13%–19% of term low birth weight deliveries, 23%–34% of sudden infant death syndrome deaths, and 5%–7% of preterm-related deaths are attributable to maternal smoking. 4 We also know that even quitting smoking in the second trimester can still be highly beneficial. Compared with mothers who smoked during their entire pregnancy, those who smoked in the first trimester and then quit smoking in the second or third trimesters had a 30% reduced risk of infant all-cause death and a 36% reduced risk of sudden unexpected infant death. 5 However, very little is known about maternal smoking and the health outcomes of the mother. In this paper, we will examine the outcomes of the mother.
Smoking during pregnancy has declined substantially. A 2023 CDC report shows that from 2016 to 2022, the percentage of mothers who smoked cigarettes during pregnancy fell by 49%, from 7.2% to 3.7%. 6,7 Despite this decline, significant racial disparities in infant birth outcomes persist. For example, between 1995 and 2020, there was a constant gap of approximately 10 percentage points between Black and White infant mortality in preterm births (31.1 versus 21.8 deaths per 1,000 preterm births, respectively). 5 A major exacerbating factor is that Black adults who smoke are almost three times more likely than White adults who smoke to use menthol cigarettes, which are more challenging to quit. 1,2,8 Among daily smoking adults, Black adults smoking menthol have 53% lower odds of quitting compared with Black adults smoking nonmenthol cigarettes, whereas White adults smoking menthol have 22% lower odds of quitting compared with White adults smoking nonmenthol. 9
The tobacco industry began branding menthol cigarettes for Black Americans after a 1953 survey showed that 5% of Black Americans preferred the menthol brand Kool compared with 2% of White Americans. For the next several decades, tobacco companies engaged in the “Menthol Wars,” vying for dominance in predominantly Black inner-city neighborhoods with menthol cigarette billboards while street vans distributed millions of free packs. Advertising campaigns in Ebony and Jet magazines and Black community newspapers appealed particularly to young Black women and teens. 10 –12 This marketing was combined with economic promotions. The highest quartile of neighborhoods with Black residents has 80% higher odds of price promotions for Newport menthol cigarettes than the lowest quartile. 13 In 2019, the industry spent $5.7 billion on price discounts paid to retailers and wholesalers to reduce the price of cigarettes to consumers. 14 Even with the recent 2022 ban on menthol in California, the industry is now introducing “nonmenthol” cigarettes by replacing menthol with a synthetic cooling agent (WS-3), mimicking the effect of menthol cigarettes. 15 –17
A ban on menthol cigarettes and synthetic menthol substitutes could potentially help Black adults quit smoking. Recent research estimates that a menthol ban would decrease smoking prevalence among Black adults by 25%, saving 6,400 Black lives a year. 18 A ban in New York City is estimated to reduced heart attacks in Black women by 8%. 19 These bans might also help Black pregnant women, who have a high rate of menthol use. 20 Currently, very little is known about the extent to which menthol cigarettes are smoked during pregnancy, especially by Black and other minoritized women. In this paper, we report on national trends in maternal smoking from 2004 to 2022, with an emphasis on understanding differences in smoking menthol and nonmenthol cigarettes and the decision to quit smoking, as well as the association between smoking during pregnancy and the health of women.
Methods
We use the 2004–2022 National Survey on Drug Use and Health (NSDUH), which provides nationally representative data on the use of tobacco, alcohol, and drugs; substance use disorders; mental health issues; and receipt of substance use and mental health treatment among the civilian, noninstitutionalized population aged 12 or older in the United States. We show the periods 2004–2019 and 2020–2022 separately, as recommended by the NSDUH because 2020–2022 respondents were not surveyed in person during the pandemic. We focus on adult pregnant women aged 18–44 years, totaling 14,226 women. We categorize women into four smoking groups: menthol cigarette smoking, nonmenthol cigarette smoking, recently quit” smoking, and nonsmoking.
Smoking is defined as having smoked cigarettes in the last 30 days, with menthol coded positive if menthol cigarettes were smoked the most in the past 30 days. “Recently quit” was flagged if the woman quit smoking in the past 12 months (and for at least the last 30 days). Nonsmoking women are those who have not smoked cigarettes in the previous 12 months. Although 1.2% of these nonsmoking pregnant women vaped during the last 30 days, we still categorize them as nonsmoking for cigarettes.
Outcomes
We examine the association between these four smoking categories and the following outcomes. General current physical health self-rated by the woman as excellent, very good, good, fair, or poor. Mental health is also self-rated, answering the question “Do you have any mental or emotional difficulties?” The number of chronic conditions out of a possible ten: high blood pressure, heart conditions, diabetes, Chronic Obstructive Pulmonary Disease, asthma, cirrhosis of the liver, hepatitis B, kidney disease, cancer, and obesity. The number of emergency department (ED) visits, inpatient admissions, and office visits over the past 12 months. Response to a question regarding whether a health professional discussed smoking or advised the person to quit smoking any time over the past 12 months, compared with no discussion or advising. The responses involve either continuing to smoke menthol or nonmenthol cigarettes or quitting.
We present nonrisk-adjusted outcomes in the paper. However, we also risk-adjust outcomes in the supplemental appendix. Covariates include six age categories, race and ethnicity, marriage, education level, income quartiles, publicly insured, uninsured anytime, and year dummy variables. Outcomes 1 and 2 (poor health and mental health, respectively) are risk-adjusted using logit regressions. For outcomes 3 and 4, we estimate the risk-adjusted relationship between the four smoking categories, the number of chronic conditions, and the number of ED and office visits using a zero-inflated Poisson count model. For outcome 5 (cessation advice), we use multivariate logit with three response values: continue to smoke menthol, continue to smoke nonmenthol cigarettes, or quit. We also examine the four smoking categories of pregnant women by race and ethnicity and by sexual identity. Race, ethnicity, and sexual identity data were collected from the database; women were identified as non-Hispanic Black, Hispanic, non-Hispanic White, or other (including Native American, Asian, and multi-race). In 2015–2022, women also self-identified as (1) lesbian, gay, or bisexual (LGB) or (2) heterosexual. This study was approved by the institutional review board of the Agency for Healthcare Research and Quality and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. All two-sided p values are generated from linear regression analyses using Stata/MP, version 18 (StataCorp). All p values account for the complex survey design.
Results
Outcomes
Table 1 presents descriptive statistics for pregnant women during our study period, 2004–2019. In total, 75.7% of pregnant women had not smoked in the past 12 months, 11.0% recently quit smoking, and 14.3% were still smoking (an average of 23 out of 30 days), with nearly half (7%) smoking menthol. Those smoking menthols had a higher number of ED visits in the last 12 months than those smoking nonmenthol (1.6 versus 1.2 visits, respectively, p = 0.02). This number of visits was almost three times the 0.6 ED visits for nonsmoking pregnant women. Those smoking menthol also had more inpatient admissions than those smoking nonmenthol (0.6 versus 0.4, p = 0.10). However, they did not differ in the number of office visits (4.5 versus 4.9, p = 0.53). We find similar results in Table 2 when we risk-adjusted for age, race, and socioeconomics. The regressions for Table 2 are shown in Supplementary Table SA1.
Descriptive Statistics for Pregnant Women Aged 18–44 Years: 2004–2019
Note: 95% confidence intervals in parentheses.
** (*) Differs compared with nonmenthol smoking women at p ≤ 0.05 (p ≤ 0.10). Smoking is in the last 30 days. Recently quit is during the last 12 months but more than 30 days ago. Nonsmoking is not smoking over the last 12 months. Lesbian/gay/bisexual status and chronic conditions are for 2015–2019. Office visits are for 2013–2019. Emergency department, inpatient, and office visits are for the last 12 months.
The Estimated Association Between Smoking and Emergency Department and Office Visits for Pregnant Women Aged 18–44 Years: 2015–2019
N = 3,536 pregnant women aged 18–44 years. Smoking in the last 30 days. Zero-inflated Poisson estimates of the number of emergency department and office visits in the last 12 months. Regressions shown in Supplementary Table SA1. Ninety-five percent confidence intervals in parentheses. Source: National Survey of Drug Use and Health. Differs from menthol.
p < 0.01.
p < 0.05.
Those smoking menthol had a higher rate of reporting poor health than did those using nonmenthol (1.4% versus 0.4%, p = 0.056). However, when risk-adjusted, in Supplementary Table SA2, those smoking nonmenthol had 5% lower odds of having poor health than those smoking menthol, but this effect was not significant. Moreover, those using menthol had a higher rate of mental health problems than those using nonmenthol in Table 1 (73.7% versus 64.4%, p = 0.10). In Supplementary Table SA2, those using nonmenthol had 38% lower odds of mental health problems than did those smoking menthol (p = 0.08). Those smoking menthols were more likely than those smoking nonmenthols to be single (76.8% versus 66%), Black (25% vs 1.8%), and LGB adults (18.5% versus 10.5%; p < 0.05). The number of chronic conditions did not vary between menthol and nonmenthol smoking pregnant women (See Supplementary Table SA3).
Disparities
In Figure 1, for the years 2004–2019, we see that maternal menthol smoking rates were higher for Black women than for White women, at 12.2% versus 7.2% (p < 0.05). Furthermore, only 9.5% of pregnant Black women quit smoking over the past year, compared with 12.3% of pregnant White women (p < 0.05). Hispanic women were the only race/ethnicity whose quit rate exceeded their smoking rate, 9.3% versus 5.9%. In terms of sexual identity, from 2015 to 2019, 18.6% of LGB pregnant women smoked menthol cigarettes compared with 7.3% of heterosexual pregnant women (p < 0.05). However, LGB women also had a higher quit rate than heterosexual pregnant women (15.4% versus 5.9%; p < 0.05).
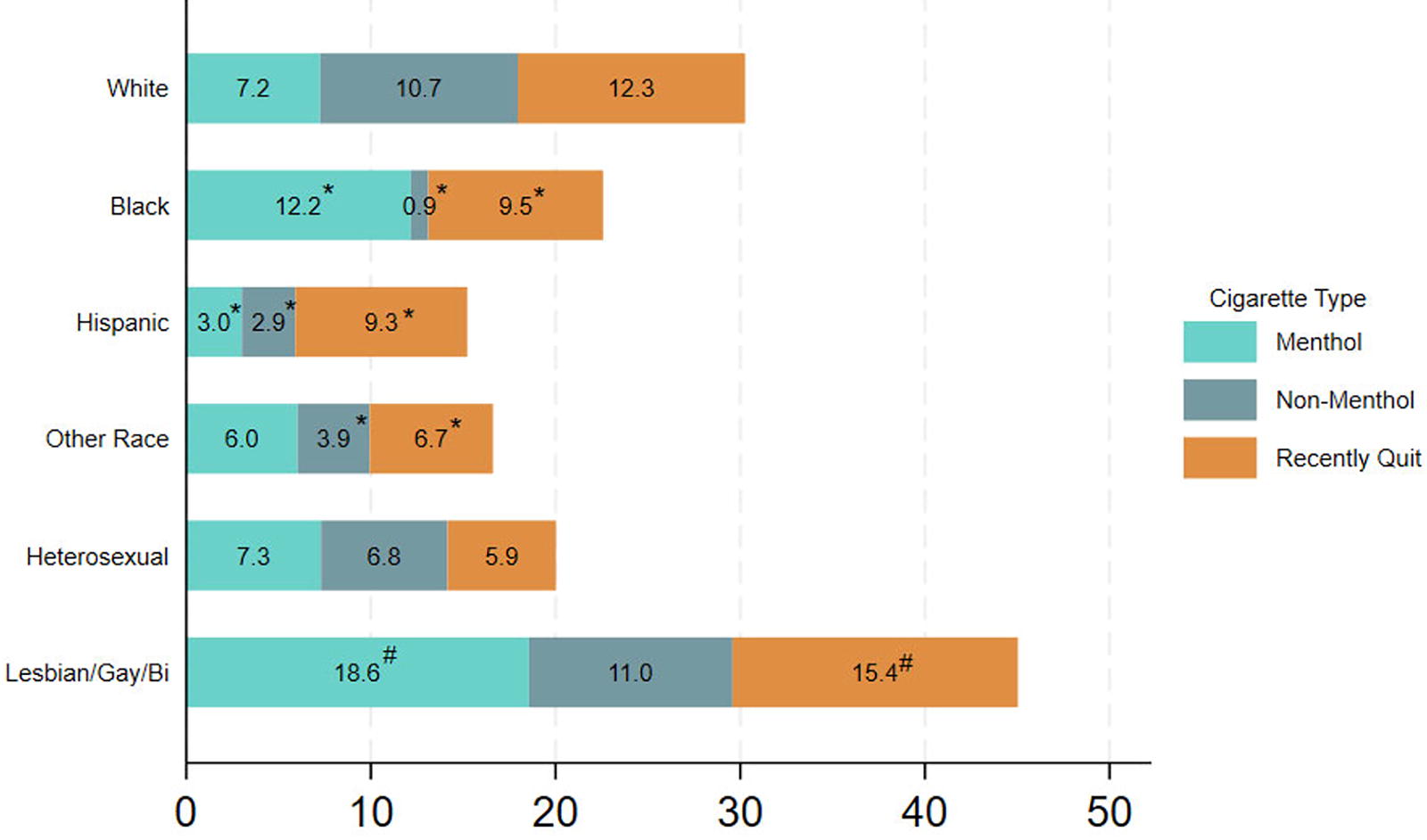
The percentage of pregnant women who smoked menthol versus nonmenthol cigarettes or recently quit, by race, ethnicity, and sexual identity: 2004–2019. N = 12,453 pregnant women aged 18–44 years. Percentage who smoked within the last 30 days or recently quit in the last 12 months but more than 30 days ago. Sexual identity defined for 2015–2019. *Smoking or quit rate differs from the White adult rates at p < 0.05. #Lesbian/gay/bisexual smoking or quit rate differs from the heterosexual rates at p < 0.05. Source: Authors’ calculations using the National Survey on Drug Use and Health.
Third-trimester smoking is the most harmful for the baby. 21 There is a large racial disparity in third-trimester smoking. As shown in Supplementary Figure SA1, 9.8% of Black pregnant women smoked menthol and 0.8% smoked nonmenthol (p < 0.01) during the third trimester, 2.0% of Hispanic pregnant women smoked menthol and 1.8% smoked nonmenthol (p = 0.7), and 3.7% of Other race pregnant women smoked menthol and 4.8% smoked nonmenthol (p = 0.9). In contrast, 5.3% of White women smoked menthol and 9.0% smoked nonmenthol (p < 0.01) in the third trimester.
Trends
Overall, from 2004 to 2022, the maternal smoking rate decreased by 69%, from 16.3% to 5.1%. In Figure 2, we bundle years (e.g., 2004–2009 versus 2020–2022) to have enough sample size by trimester of pregnancy. The “all” columns give the average rates over all three trimesters. By combining menthol and nonmenthol rates in the “all” columns, we see that from 2004–2009 to 2020–2022, the percentage of pregnant women smoking decreased from 15.5% to 8.6% (p < 0.01) and this decline was primarily driven by the decrease in nonmenthol cigarette smoking, which dropped from 8.6% to 3.4% (p < 0.05). The point estimate for menthol use declined from 6.9% to 5.2%, but this decline was not significant. Menthol smoking in the second trimester increased from 5.5% in 2004–2009 to 6.5% in 2015–2019 (p = 0.4). In the 2004–2009 “all” column, the rate of menthol smoking was below that of nonmenthol smoking (6.9% versus 8.6%, p = 0.01). However, by 2020–2022, the rate of menthol smoking surpassed that of nonmenthol smoking (5.2% versus 3.4%, p = 0.09).

National percentage of pregnant women aged 18–44 years who smoked menthol versus nonmenthol cigarettes or recently quit, by trimester: 2004–2022. N = 14,097 pregnant women age 18–44. Percentage within trimester who smoked in the last 30 days or recently quit within the past 12 months but more than 30 days ago. *Indicates the smoking or quit rate differs from the corresponding rate for the same trimester or all columns in 2004–09 at p < 0.05. Source: Authors’ calculations using the National Survey on Drug Use and Health.
In Figure 3, for the period 2004–2022, the overall proportion of pregnant smoking women who used menthol increased from 47.0% to 60.1% (p = 0.09). This overall increase reflects increases among Hispanic women (43.4% to 78.8%, p < 0.05), White women (34.7% to 48.6%, p < 0.05), and women of Other races (64.3% to 71.1%, p < 0.05).
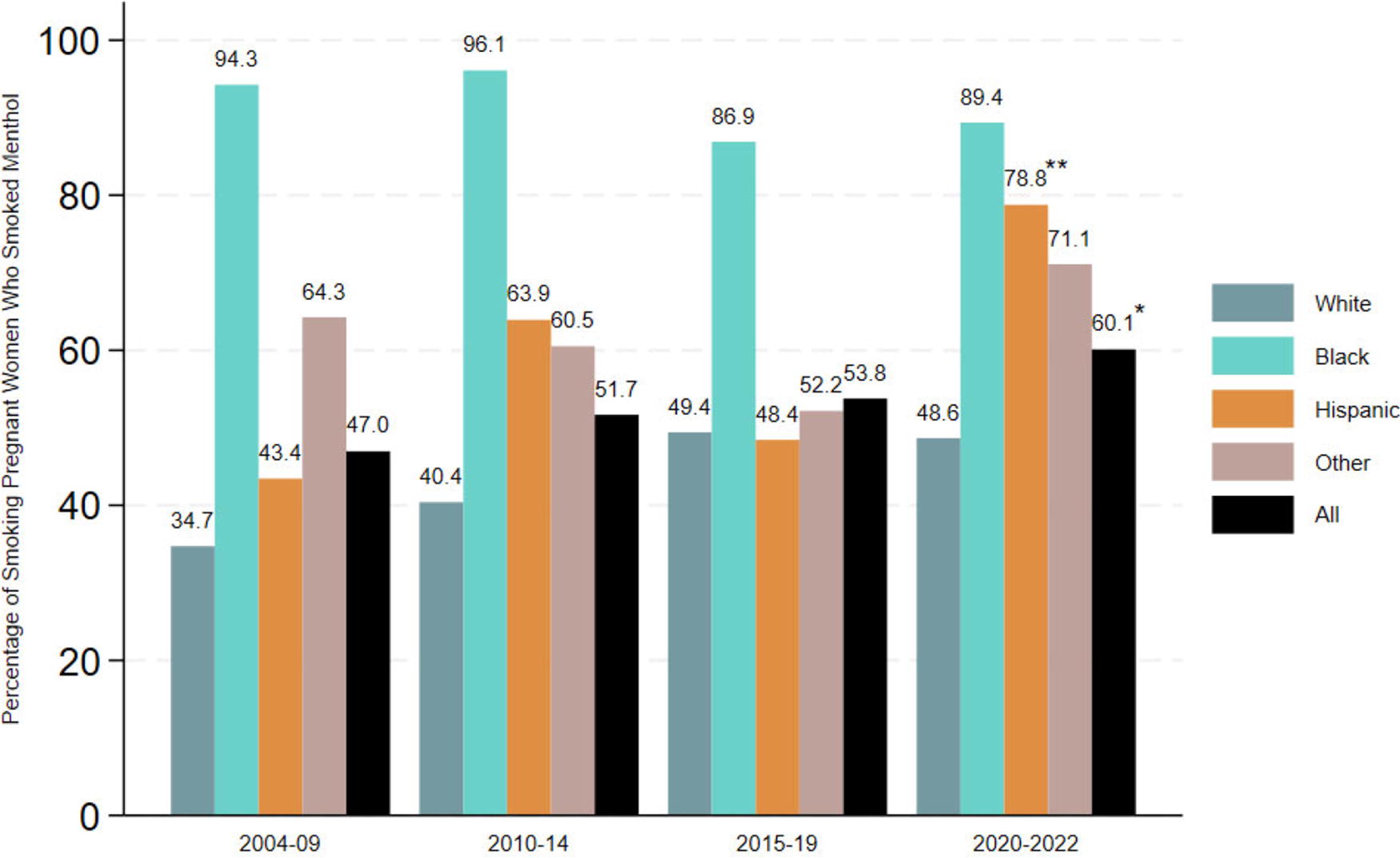
Percentage of smoking pregnant women who smoked menthol cigarettes, by race and ethnicity: 2004–2022. N = 2,916 pregnant women aged 18–44 years who smoked in the last 30 days. ** (*) 2020–2022 rate differs from the 2004–2009 rate at p < 0.05 (p < 0.1). Source: Authors’ calculations using the National Survey on Drug Use and Health.
Over the entire period, percentages ranged from 86.9% to 96.1% of pregnant Black women who smoked menthol cigarettes. In contrast, percentages rose from 34.7% to 48.6% of pregnant White women who smoked menthol cigarettes. So, Black women who smoked were almost twice as likely to use menthol than White women who smoked. This disparity persisted into the third trimester, where 94.4% of Black women smoked menthols compared with 38.2% of White women (Supplementary Fig. SA2).
Cessation
Overall, 85.3% of pregnant women who smoked over the past 12 months were asked by a health care professional about their smoking and were advised to quit (not shown). This advising varied by race: 88.6% for White women, 82.1% for Black women, 76.0% for Hispanic women (p = 0.04 compared with White women), and 77.0% (p = 0.08) for Other races. Among all pregnant women asked about smoking or advised to quit by a health care professional over the last 12 months, the overall quit rate was 45.7%, compared with 36.1% for those who were not asked about smoking nor advised to quit (p = 0.08) (See Supplementary Fig. SA3). However, the nonmenthol smoking rate was lower (24.1% versus 34.3%, p = 0.06) among those who had a professional ask about smoking or advised to quit. Menthol smoking remained at around 30% for those who smoked over the last 12 months, regardless of a health professional’s help (p = 0.91). In Supplementary Table SA4, we risk-adjust these numbers and estimate that women asked/advised to quit had 55% (p < 0.01) lower relative risks of still smoking nonmenthol cigarettes versus quitting than women not asked/advised to quit. For women using menthols, there was no correlation between quitting and being asked/advised to quit.
The relationship with health professional advice varied by race and ethnicity, as shown in Figure 4. The first observation is that for every race and ethnicity, menthol (12-month) smoking rates did not differ significantly between those who had a professional ask about smoking or advise quitting versus those with no such interaction. However, Hispanic women asked or advised to quit had a higher rate of quitting (70.2% versus 41.3%, p < 0.05) compared with Hispanic women not asked or advised to quit, and had a smaller rate of nonmenthol smoking (9.1% versus 37.9%, p < 0.05). White women asked about smoking/quitting also had more quits (42.9% versus 30.9%, p < 0.05) with less nonmenthol smoking (29.6% vs 44.7%, p < 0.05) versus those White women not asked to quit. In contrast, Black women had a different pattern, with 4.9 percentage points more of nonmenthol smoking (p = 0.07) when asked about smoking/quitting versus Black women not asked. However, this effect possibly was a substitutionary effect, with a commensurate 4.3 percentage point lower rate of menthol smoking (p = 0.81) when asked or advised to quit.
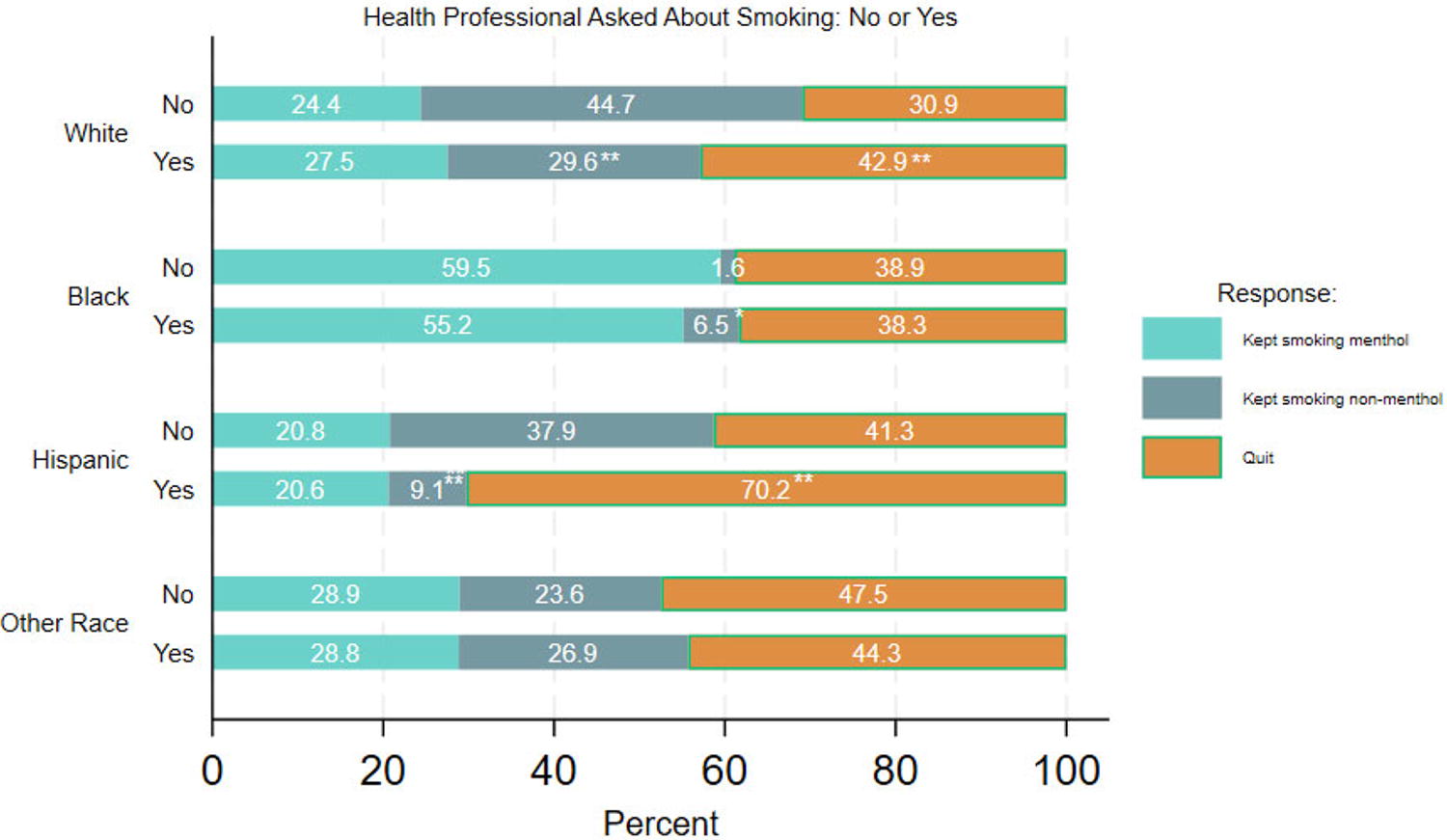
Pregnant women who smoked the past year and responded to a health professional asking about smoking, by race and ethnicity: 2013–2019. N = 1,315 pregnant women aged 18–44 years who smoked within the last 12 months. Yes = the patient was asked if they smoked and/or were advised to quit. No = the patient was not asked if they smoked and was not advised to quit in last 12 months. To quit is quitting more than 30 days ago. Kept smoking is smoking within the last 30 days. ** (*) Menthol, nonmenthol, or quit rates for Yes differ from those for No within race/ethnicity at p < 0.05 (p < 0.10). Source: Authors’ calculations using the National Survey on Drug Use and Health.
Discussion
Using the National Vital Statistics System (NVSS), the CDC has shown a large decline in maternal smoking, a 49% decline from 7.2% to 3.7% between 2016 and 2022. 6 Using the NSDUH, we show a similar 50% decline from 10.2% to 5.1%. However, our maternal smoking rates are higher than the NVSS’s rates, as the NVSS examined smoking rates only for women who gave birth. The NSDUH examined smoking among all pregnant women (including those with subsequent abortions and miscarriages after the interview; about 60% of pregnant women have a live birth). However, when we subset to the third trimester, our smoking rate is exactly what the NVSS data show (5.7% in 2016). 22 Thus, the NSDUH includes a broader set of pregnant women, including those who may have miscarried due to smoking. 23
What is new beyond the NVSS’s previous smoking reduction results is that almost all of this decline in maternal smoking was only with nonmenthol cigarettes. Maternal menthol cigarette smoking has persisted over the last two decades. This persistence disproportionately affected Black women and LGB women, who together make up 25% of the pregnant population but 44% of the maternal women smoking menthol. A national ban on menthol cigarettes will likely help reduce smoking in these highly vulnerable populations, especially Black women who suffer from high rates of maternal death and severe maternal morbidity. The dramatic increase in smoking of menthols by pregnant Hispanic women poses a severe challenge to another minoritized population with a higher-than-average fertility rate. 24
While initiating a national ban in the United States has been delayed, 25 many localities in the United States are banning menthol cigarettes. A recent meta-analysis of the literature found that a ban on menthol cigarettes, in general, causes 24% of those smoking menthol cigarettes to stop smoking. 4 Such a reduction in menthol cigarette smoking will likely improve maternal outcomes. For example, the percentage of women reporting mental health problems was 9.3 percentage points higher for women smoking menthol than women smoking nonmenthol. Poor physical health was reported to be more than three times as common among women smoking menthol. Also, women smoking menthol had 50% more inpatient admissions and 33% more ED visits than women smoking nonmenthol cigarettes, but no difference was observed for office visits. This finding suggests that the hospital visits were likely due to poorer health and not due to barriers to office visits. Using our results on excess ED visits due to menthol smoking in Table 2, we estimate that there is an excess of 32,400 extra ED visits each year due to menthol smoking versus nonmenthol smoking among pregnant women. A ban would likely reduce these excess ED visits. A limitation of our research is that we had no data on the associated infants at birth. Future research should examine the impact of such a menthol ban on infant morbidity and mortality.
Our findings reinforce our understanding that not smoking cigarettes is associated with higher health status and reduced health care expenditures for pregnant women. Recognizing that smoking is still a leading cause of preventable disability and death, the U.S. Department of Health and Human Services (DHHS) issued the “2023 Framework to Support and Accelerate Smoking Cessation” with six major goals. The first goal is “To Eliminate Smoking- and Cessation-Related Disparities.” 26 We found that Hispanic and Other race (e.g., American Indian) pregnant women receive less help from a health professional regarding quitting smoking, particularly during pregnancy, than did White women. Thus, there is potential for expanded cessation efforts to reduce racial and ethnic disparities in cessation, especially for African American, Hispanic, and American Indian women in childbearing ages.
Menthol cigarettes are the hardest cigarettes to quit. 27 We found that the largest increase in menthol smoking while pregnant was among Hispanic women. Menthol cigarettes have been heavily marketed to Black communities since the 1950s. Now, Hispanic youth experience the highest level of tobacco advertisement exposure compared with Black and White youth. 28 Hispanic youth had the largest increase in flavored tobacco product use (30.3%) over 30 days and were the most likely to vape in the future (42.3%). 29 In particular, Hispanic youths have higher rates of menthol use than Non-Hispanic White youths. 30
Given the increased difficulty menthol smokers face in quitting, we must develop more effective approaches that patients can use to quit. Based on our findings, several strategies beyond banning menthol cigarettes are worth further investigation, such as targeted or culturally-specific tobacco cessation efforts. Given the increasing use of menthols that we observed in the Hispanic population, smoking cessation programs targeting Hispanics should prove beneficial. Similarly, community-engaged menthol smoking cessation interventions need development just as community-targeted menthol advertising raised the demand for menthols in African American communities and now in Hispanic communities. Based on behaviors observed after menthol bans, they have direct and indirect effects on smoking cessation, suggesting that educational and awareness campaigns that target both types of impact will likely support more smoking cessation in implementing such policies.
A limitation of our article is that we could not estimate a causal effect of smoking cessation efforts on actual quitting among pregnant women. We only observed what patients self-reported during the survey about cessation over the past 12 months. Future research should explore the causal effect in greater detail. However, our preliminary results suggest that a renewed focus on smoking cessation programs in maternal care would go a long way in achieving DHHS’s first goal of reducing smoking cession disparities and likely improving the health of pregnant women, reducing their risks of poor pregnancy outcomes. The U.S. Preventive Services Task Force found insufficient empirical evidence to recommend the use of pharmacotherapy interventions for smoking cessation in pregnant women. Also, it is not known if e-cigarettes are less toxic than cigarettes for pregnant women. Given our findings that smoking contributes to more maternal hospitalizations, the major policy efforts to address maternal mortality and morbidity should not just focus on clinical issues but also provide funding to develop more smoking cessation interventions and technologies for pregnant women beyond behavioral interventions, focusing on menthol cessation. 31
Footnotes
Disclaimer
The views expressed in this article are those of the authors, and no official endorsement by the U.S. Department of Health and Human Services or the Agency for Healthcare Research and Quality (AHRQ) is intended or should be inferred.
Authors’ Contributions
W.E.: Conceptualization, data curation, methodology, formal analysis, visualization and writing. R.B.V.: Conceptualization, methodology, visualization and writing.
Author Disclosure Statement
No conflicts exist.
Funding Information
This study was funded by AHRQ. Role of the Funder/Sponsor: The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication. The views expressed in this article are those of the authors, and no official endorsement by the U.S. Department of Health and Human Services and AHRQ is intended or should be inferred.
Supplementary Material
Supplementary Figure SA1
Supplementary Figure SA2
Supplementary Figure SA3
Supplementary Table SA1
Supplementary Table SA2
Supplementary Table SA3
Supplementary Table SA4
Supplementary Data SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.