
Abstract
Introduction:
Postpartum acute care utilization (PACU), including visits to an emergency department, obstetric triage, or urgent care (“outpatient”), and hospital readmissions, may indicate medical complications and signal unmet health needs.
Methods:
We estimated the incidence of PACU and examined patterns by sociodemographic factors, pregnancy and birth characteristics, time since discharge from the birth hospitalization, and medical indications. We constructed a retrospective cohort of people aged ≥18 years who delivered ≥1 liveborn infant >20 weeks of gestation from July 1, 2021, to December 31, 2022, using electronic health record data from a quaternary maternity hospital in the Southeastern United States PACU data throughout the health care system were collected through March 31, 2023. We excluded people with a hospital stay >6 days (n = 29).
Results:
In this cohort of 6,041 birthing people, 11.3% had ≥1 outpatient encounters (range 0–6) and 3.2% had ≥1 hospital readmissions (range 0–4) within 12 weeks of discharge from the birth hospitalization. Median time to first outpatient PACU was 10 days post-discharge and 6 days for first hospital readmission. Among encounters for the top five medical indications, time to first postpartum acute care encounter varied by medical indication (log-rank test of equality over strata Chi-square = 69.93, degrees of freedom = 4, p < 0.0001). Complications specified during the puerperium (n = 234) and hypertension and hypertensive-related conditions complicating the puerperium (n = 87) were the two most frequent indications.
Conclusion:
These findings can inform efforts to direct health resources to improve postpartum health care and health outcomes.
Introduction
The postpartum period is a vulnerable time for the health of birthing people: two-thirds of pregnancy-related deaths in the United States occur a day or more after childbirth and birthing people frequently experience medical complications in the postpartum period. 2,3 Despite this, in the United States, high-quality, systematic data on maternal morbidity after the birth hospitalization are not well characterized. 4
One approach for assessing postpartum health status is to quantify postpartum acute care utilization (PACU). Many birthing people utilize acute care in the postpartum period, including visits to the emergency department (ED), obstetric (OB) triage, urgent care facility, and hospital readmissions. 5 –10 PACU may indicate medical complications after discharge from the birth hospitalization and may signal unmet postpartum health needs.
Assessing patterns of PACU can inform efforts to improve perinatal health care systems so that birthing people are healthy and safe postpartum. The objectives of this study were to estimate the incidence of PACU in the early postpartum period within a Southeastern health care system and to examine patterns of PACU by sociodemographic factors, pregnancy and birth characteristics, postpartum maternity visit attendance, time since discharge from the birth hospitalization, and medical indications.
Methods
Study design and data source
This study was reviewed and approved by the University of North Carolina (UNC) Office of Human Research Ethics (IRB# 22–0156). Using electronic health record (EHR) data from North Carolina (NC) Women’s Hospital and the UNC Health System, we constructed a retrospective cohort of individuals aged ≥18 years who gave birth to ≥1 liveborn infant at >20 weeks of gestation from July 1, 2021 to December 31, 2022 at NC Women’s Hospital, a quaternary care maternity hospital with over 4,000 births per year. For individuals with two eligible live births during the study period (n = 39), we randomly selected one birth for inclusion in the cohort.
PACU data for visits occurring throughout the UNC Health System were collected through March 31, 2023. Time zero for PACU was defined as the day of discharge from the birth hospitalization, not date of delivery, to avoid immortal time bias. 11 For this analysis, individuals were followed for 12 weeks (84 days) from the date of discharge. Because lengthy stays at the birth hospital indicate a medical problem, we excluded those with a birth hospitalization stay >6 days (n = 29) (Supplementary Fig. S1).
Key Variables
Outcomes
We examined PACU in the 12 weeks following discharge from the birth hospitalization. We defined PACU in three ways, which were not mutually exclusive: (1) any PACU (visits to an ED, OB triage, or urgent care facility, and hospital readmissions); (2) outpatient PACU (visits to an ED, OB triage, or urgent care facility that did not result in hospital readmission); and (3) hospital readmission (including visits that originated in an ED or OB triage that resulted in hospital readmission). We calculated the timing of each acute care encounter as the number of midnights between discharge from the birth hospitalization and PACU.
Sociodemographic factors
We extracted sociodemographic information as recorded in the EHR for the birthing person at the birth hospitalization: age in years (18–19, 20–29, 30–39, 40 and older), insurance provider (private versus Medicaid, Medicare, or self-pay), residential address, race/ethnicity (non-Hispanic [NH] White, Hispanic, NH Black, NH additional/not reported), primary language (English, Spanish, other), and marital/partner status (married/partnered, unmarried/not partnered, and unspecified/unknown). Using the census code of the birthing person’s residential address at the time of birth hospitalization, metropolitan and non-metropolitan (including micropolitan, small town, and rural areas) was defined by primary Rural-Urban Commuting Area codes, consistent with other published studies. 12 –14 Since EHR data do not include measures of racism, we extracted race and ethnicity from the EHR to use as a proxy for the experience of interpersonal and structural racism. 15 –17 Among individuals with Hispanic ethnicity recorded, 85% did not have a race reported, so we were not able to disaggregate Hispanic ethnicity by race.
Pregnancy and birth characteristics
Pregnancy and birth characteristics extracted from the EHR included parity (defined as the total number of live births prior to the birth in this study [0, 1–4, and 5+], categories correspond to nulliparity, multiparity, and grand multiparity), 18 plurality (singleton versus multiple gestation), gestational age at birth in weeks (<28, 28–36, 37–40, and 41+), mode of delivery (vaginal, Cesarean section, and vaginal birth after Cesarean), non-transfusion severe maternal morbidity (SMM) during the birth hospitalization, maternal comorbidities, maternal major mental health disorder, length of the birthing person’s postpartum hospital stay in days (0, 1, 2, 3, 4, 5, and 6), whether any baby from the birth stayed in the neonatal intensive care unit (NICU) (yes/no), whether any baby from the birth had a hospital stay longer than the birthing person (yes/no). SMM, excluding blood transfusion, was defined using International Classification of Diseases 10th Revision (ICD-10) diagnosis and procedure codes for 20 indicators in the birth hospitalization claim, consistent with federal definitions and reporting. 19 We categorized birthing people as having no SMM indicators or ≥1 SMM indicator. To assess a birthing person’s burden of comorbidities, we used the validated OB scoring system developed by Leonard and colleagues to identify and weight 27 comorbidities according to their association with non-transfusion SMM, generating an overall comorbidity score. 20 Because mental health conditions are a leading underlying cause of pregnancy-related mortality in the United States, we stratified PACU by the presence of a major mental health disorder diagnosis code at the birth hospitalization (i.e., other mental health disorders complicating pregnancy, childbirth, and the puerperium [O99.34], schizophrenia, schizotypal and delusional disorders [F20-F29] and mood (affective) disorders [F30-F39]). 1,20
Postpartum maternity visit
We defined a “postpartum maternity visit” as a scheduled health care encounter that took place after discharge from the birth hospitalization with a visit type listed as “initial prenatal,” “office visit,” “postpartum visit,” “routine prenatal” or “telemedicine” that had a department specialty of “family medicine,” “obstetrics,” or “obstetrics and gynecology.”
Medical indications
We defined the “medical indication” for each acute care encounter using the primary final coded diagnosis of the encounter, which is the stated diagnosis of the patient reported for billing purposes. It was extracted from the EHR and categorized using the Clinical Classifications Software Refined (CCSR) system published by Healthcare Cost and Utilization Project, which aggregates ICD-10 codes into clinically meaningful categories. 21 When more than one primary final coded diagnosis was present, we prioritized using Current Procedural Terminology codes (Supplementary Table S1).
Chief complaint, the stated reason for the acute care encounter given by the patient, was extracted from the EHR and categorized using methods employed by Brousseau et al. in which common postpartum conditions, such as vaginal bleeding and fever, were grouped separately and systems-based categories were created for other complaints (Supplementary Table S2). 5
Statistical Analysis
Using bivariate analyses, we assessed whether sociodemographic factors, pregnancy, and birth characteristics were associated with any PACU, outpatient PACU, and hospital readmission. Among birthing people who attended a postpartum maternity visit and had a postpartum acute care encounter within 84 days of discharge from the birth hospitalization, we assessed whether the individual attended the postpartum maternity visit before, after, or on the same day as their postpartum acute care encounter. This was done to characterize whether acute care utilization was the birthing person’s first health care encounter for their own health needs following discharge from the birth hospitalization, which is important for informing improvements to postpartum health care systems.
We calculated the ten most common CCSR medical indications for each PACU outcome. We also calculated the top ten medical indications grouped by body system for each PACU outcome and report the top five medical indications within the leading body system category for each PACU outcome. Among PACU for the five most common medical indications within each PACU outcome, we generated 12-week cumulative incidence curves stratified by medical indication and assessed the equivalence of time to first PACU by medical indication using log-rank tests for equality over strata.
Chief complaint was missing for 40% of OB triage visits and 24% of hospital readmissions; because of these data quality issues, we categorized and report chief complaint for ED and urgent care visits only.
Statistical significance was assessed at an alpha level of 0.05. Analyses were conducted using SAS Software for Windows version 9.4 (SAS Inc, Cary, NC).
Results
In this cohort of 6,041 birthing people, 13.3% had ≥1 postpartum acute care encounter, 11.3% had ≥1 outpatient postpartum acute care encounter (range: 0–6), and 3.2% had ≥1 hospital readmission (range: 0–4) within 12 weeks of discharge from the birth hospitalization. The median time to first PACU was 10 days after the birth hospitalization discharge date for outpatient encounters and 6 days for hospital readmissions. Approximately one-quarter (n = 1,679) of the cohort did not have a postpartum acute care encounter or a postpartum maternity visit within the UNC Health System in the 12 weeks after discharge from the childbirth hospitalization.
Sociodemographic characteristics of the cohort are presented in Table 1 overall and for any PACU, outpatient PACU, and hospital readmissions. Birthing people insured by Medicaid, Medicare, or self-pay comprised 52% of the cohort; while they accounted for a similar proportion of outpatient PACU, they accounted for 63% of postpartum hospital readmissions. Although Hispanic/Latinx individuals made up 27% of the cohort, they accounted for 22% of outpatient PACU and 31% of postpartum hospital readmissions. NH Black birthing people comprised 21% of the cohort and accounted for 28% of outpatient PACU and 32% of postpartum hospital readmissions. Those with a preferred language of Spanish made up 13% of the cohort and accounted for 7.6% of outpatient PACU and 14% of postpartum hospital readmissions.
Sociodemographic Characteristics of Birthing People Aged ≥18 Years Who Gave Birth to ≥1 Liveborn Infant at >20 Weeks of Gestation at a Quaternary Maternity Hospital in the Southeastern United States Between July 1, 2021, and December 31, 2022, and Their Postpartum Acute Care Utilization up to 12 Weeks after Discharge from the Birth Hospitalization
Includes hospital admissions and visits to an Emergency Department, Obstetric triage, or urgent care facility within the University of North Carolina Health System that occurred within 84 days of discharge from the birth hospitalization.
Includes visits to an Emergency Department, Obstetric triage, or urgent care facility within the University of North Carolina Health System that did not result in hospital admission and occurred within 84 days of discharge from the birth hospitalization.
Defined as any visit that resulted in hospital admission, including those that originated in an Emergency Department or Obstetric triage, that occurred within 84 days of discharge from the birth hospitalization.
Using the Census code of the birthing person’s residential address at birth as recorded in the electronic health record matched with primary Rural-Urban Commuting Area (RUCA) codes, metropolitan was defined as “metropolitan” and non-metropolitan was defined as “micropolitan,” “small town,” and “rural areas.” 12
The electronic health record data used in this analysis do not include measures of structural racism, so race and ethnicity were extracted to serve as proxies for the experience of structural racism. Among birthing people with Hispanic ethnicity recorded, 85% did not have a value for race recorded, so Hispanic ethnicity could not be disaggregated by race. The Additional/Not Reported group includes American Indian/Alaskan Native, Native Hawaiian or Other Pacific Islander, multi-race, and not reported; these groups could not be analyzed separately in accordance with policies about reporting small cell sizes.
Categories with a sample size <11 are not presented in accordance with policies about reporting small cell sizes.
Pregnancy and birth characteristics of the cohort are presented in Table 2 overall and for any PACU, outpatient PACU, and hospital readmissions. Individuals who delivered via Cesarean section made up 31% of the cohort, but accounted for 45% of postpartum hospital readmissions. Those with nontransfusion SMM at delivery made up 1.8% of the cohort, but accounted for 7.4% of hospital readmissions. Individuals whose babies were sent to the NICU and people who were discharged home before their infant(s) had a higher incidence of outpatient PACU and postpartum hospital readmissions compared with the proportion of the total sample that they made up. Individuals with a major mental health disorder comprised 27% of the cohort and accounted for 35% of outpatient PACU and 36% of postpartum hospital readmissions.
Pregnancy and Birth Characteristics of Birthing People Aged ≥18 Years Who Gave Birth to ≥1 Liveborn Infant at >20 Weeks of Gestation at a Quaternary Maternity Hospital in the Southeastern United States Between July 1, 2021, and December 31, 2022 and Their Maternity Care Utilization and Postpartum Acute Care Utilization up to 12 Weeks after Discharge from the Birth Hospitalization
Includes hospital admissions and visits to an Emergency Department, Obstetric triage, or urgent care facility within the University of North Carolina Health System that occurred within 84 days of discharge from the birth hospitalization.
Includes visits to an Emergency Department, Obstetric triage, or urgent care facility within the University of North Carolina Health System that did not result in hospital admission and occurred within 84 days of discharge from the birth hospitalization.
Defined as any visit that resulted in hospital admission, including those that originated in an Emergency Department or Obstetric triage, that occurred within 84 days of discharge from the birth hospitalization.
Defined as the total number of live births prior to the birth in this study.
Severe maternal morbidity during the birth hospitalization, excluding blood transfusion, was defined using International Classification of Diseases 10th Revision diagnosis and procedure codes for 20 indicators in the birth hospitalization claim. 19
Comorbidities at the birth hospitalization were identified using the International Classification of Diseases 10th Revision codes specified in the validated obstetric scoring system developed by Leonard and colleagues wherein 27 comorbidities were flagged and multiplied by derived risk scores for nontransfusion severe maternal morbidity. 20
As defined by Leonard et al., including “other mental health disorders complicating pregnancy, childbirth, and the puerperium” (O99.34), “schizophrenia, schizotypal, and delusional disorders” (F20–F29) and “mood (affective) disorders” (F30–F39). 20
Individuals with birth hospitalization stays greater than 6 days were excluded from this analysis. Length of postpartum hospital stay was defined as the number of midnights between when an individual gave birth and when they were discharged from the birth hospitalization.
Defined as a scheduled health care encounter with a visit type listed as “initial prenatal,” “office visit,” “postpartum visit,” “routine prenatal,” or “telemedicine” that had a department specialty of “family medicine,” “obstetrics,” or “obstetrics and gynecology.” We report this measure only for birthing people who had a postpartum maternity visit and a postpartum acute care encounter within 84 days of discharge from the birth hospitalization.
Categories with a sample size <11 are not presented in accordance with policies about reporting small cell sizes.
Among birthing people with outpatient PACU and a postpartum maternity visit, 34% attended a maternity visit before the outpatient acute care encounter and 5% attended a maternity visit on the same day. Among birthing people who had a postpartum hospital readmission and a postpartum maternity visit, 26% attended a maternity visit before readmission and 8% attended a maternity visit on the same day.
The top ten medical indications for first postpartum acute care encounters, first outpatient postpartum acute care encounters, and first hospital readmissions are presented in Table 3. The top ten medical indications grouped by body system for each PACU outcome are presented in Supplementary Table S3, and the top five medical indications within the leading body system category for each PACU outcome are presented in Supplementary Table S4. For all three PACU outcomes, the leading medical indication was complications specified during the puerperium [e.g., “Other specified diseases and conditions complicating puerperium (O99.893),” “Delayed and secondary postpartum hemorrhage (O72.2)”]. The leading ICD-10 codes within this medical indication are presented in Supplementary Table S5.
Top Ten Medical Indications for First Acute Care Encounters, First Outpatient Acute Care Encounters, and First Hospital Readmissions up to 12 Weeks After Discharge from the Birth Hospitalization in a Cohort of Birthing People Aged ≥18 Years Who Gave Birth to ≥1 Liveborn Infant at >20 Weeks of Gestation at a Quaternary Maternity Hospital in the Southeastern United States Between July 1, 2021, and December 31, 2022
The final coded diagnosis, the stated diagnoses of the patient reported for billing purposes, was extracted from the electronic health record and categorized using the Clinical Classifications Software Refined (CCSR) system published by Healthcare Cost and Utilization Project, which aggregates International Classification of Diseases 10th Revision codes into clinically meaningful categories. 21 Categories with a sample size <11 are not presented in accordance with policies about reporting small cell sizes.
Hypertension and hypertensive-related conditions complicating the puerperium were the second leading medical indication for first PACU (11%) and first for hospital readmissions (31%) and the third leading indication for first outpatient PACU (6%). The leading ICD-10 codes within this medical indication are presented in Supplementary Table S6.
Among encounters for the top five medical indications, time to first postpartum acute care encounter varied by medical indication. Over three-quarters of encounters for hypertension and hypertensive-related conditions occurred in the first week after discharge, while encounters for abdominal pain and other digestive/abdomen symptoms occurred more gradually in the 12 weeks following discharge (log-rank test of equality over strata Chi-square = 69.93, degrees of freedom [df]=4, p < 0.0001, Fig. 1). Results for first outpatient PACU were similar (log-rank test of equality over strata Chi-square = 68.46, df = 4, p < 0.0001, Fig. 2). Time to first hospital readmission also varied by indication among the leading indications (log-rank test of equality over strata: Chi-square = 56.34, df = 3, p < 0.0001, Fig. 3).
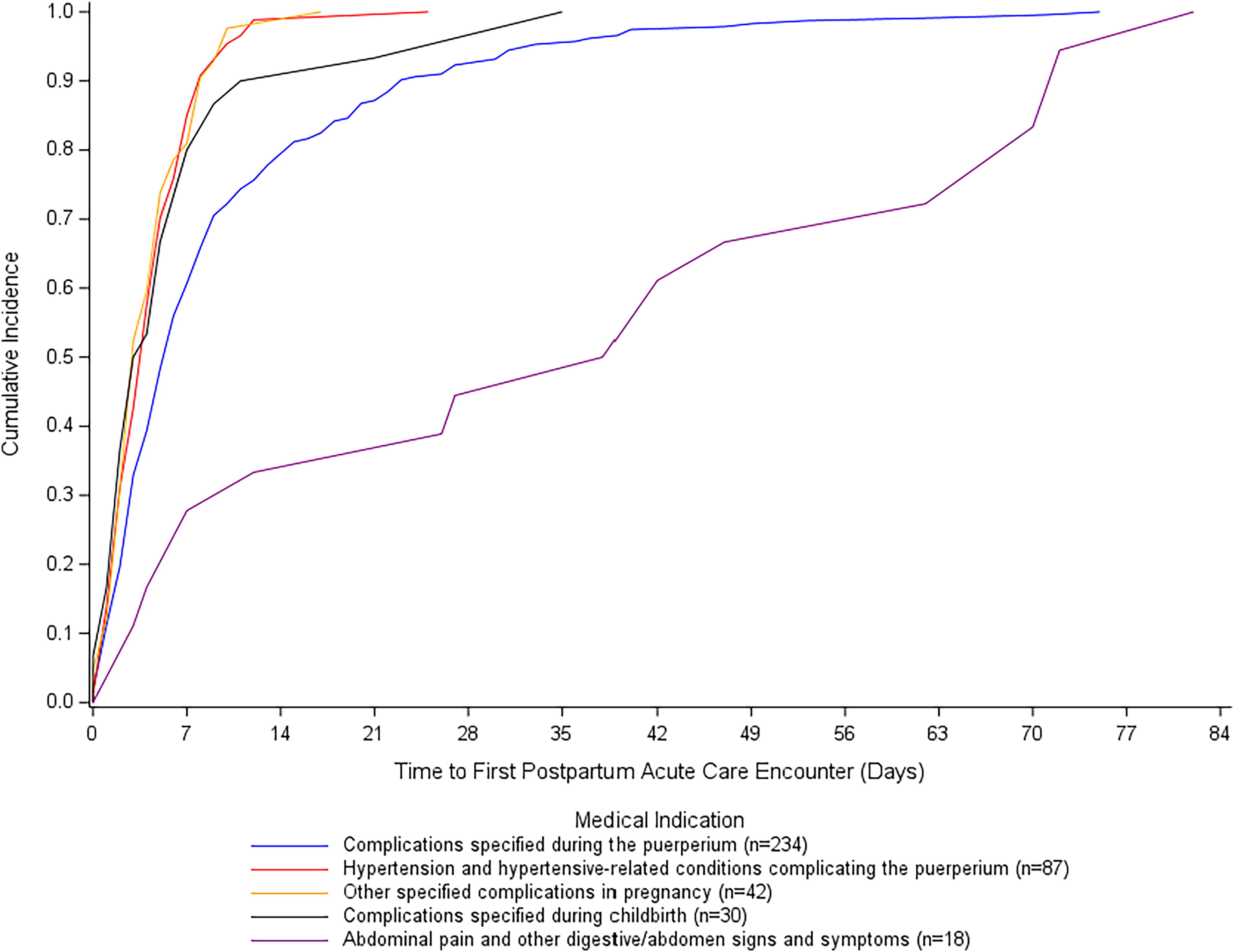
Time to first postpartum acute care encounter since discharge from the birth hospitalization among the five most frequent medical indications (log-rank test of equality over strata: Chi-square = 69.93, df = 4, p < 0.0001

Time to first outpatient postpartum acute care encounter since discharge from the birth hospitalization for the five most frequent medical indications (log-rank test of equality over strata: Chi-square = 68.46, df = 4, p < 0.0001). Medical indications were determined using the final coded diagnosis, the stated diagnoses of the patient reported for billing purposes, extracted from the electronic health record of the birthing person, and categorized using the Clinical Classifications Software Refined (CCSR) system published by Healthcare Cost and Utilization Project.
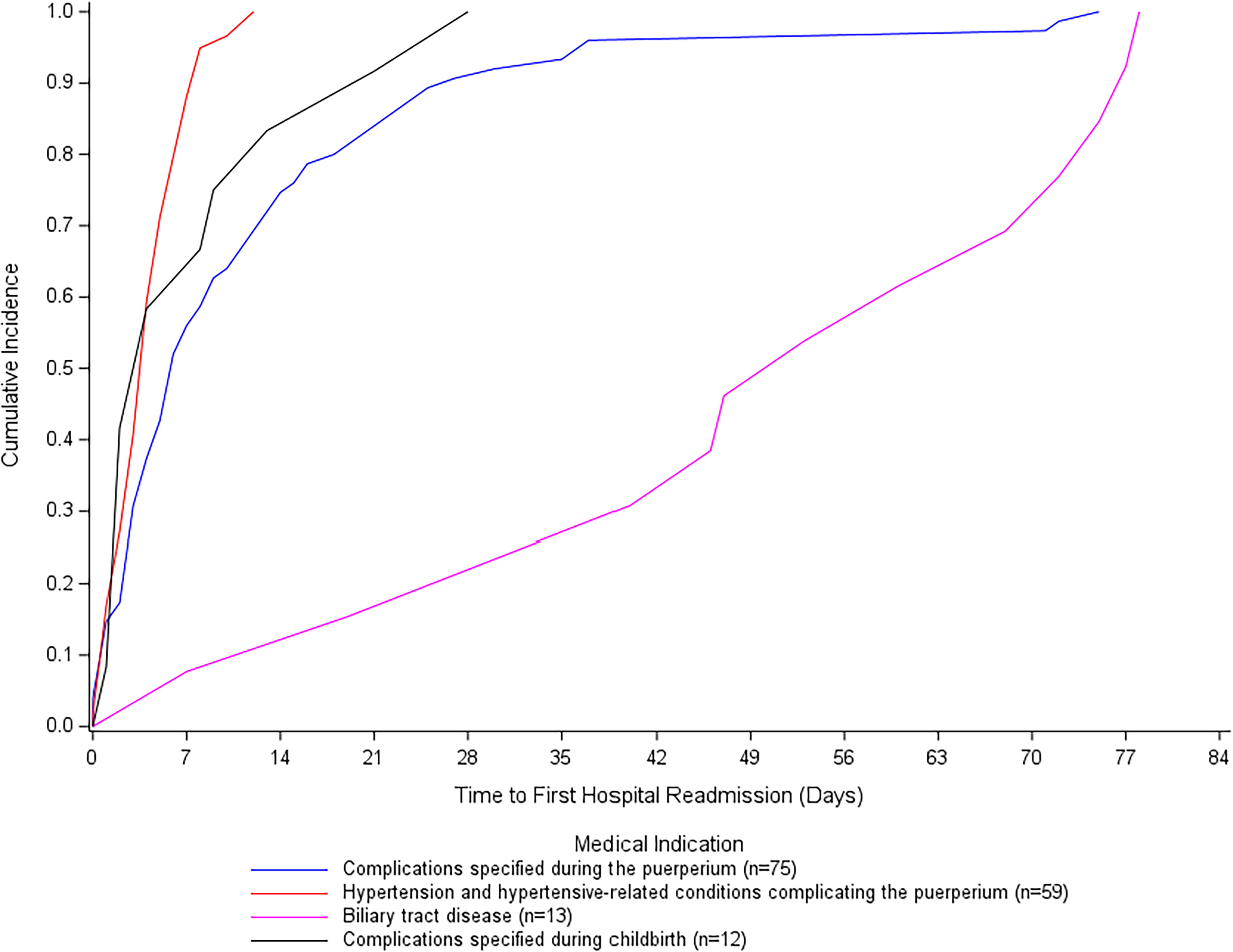
Time to first hospital readmission since discharge from the birth hospitalization for the four most frequent medical indications (log-rank test of equality over strata: Chi-square = 56.34, df = 3, p < 0.0001
The leading chief complaints for first ED visits were wound/surgery complications, abdominal pain, and cardiology complaints (e.g., chest pain, palpitations, and shortness of breath), which each accounted for one in ten visits (Table 4). For first urgent care visits, the leading chief complaints were infectious disease (18%), general/miscellaneous (14%), and head and neck pain/problem/swelling (11%) (Table 5).
Chief Complaint for First Emergency Department Visits up to 12 Weeks After Discharge from the Birth Hospitalization in a Cohort of Birthing People Aged ≥18 Years Who Gave Birth to ≥1 Liveborn Infant at >20 Weeks of Gestation at a Quaternary Maternity Hospital in the Southeastern United States Between July 1, 2021, and December 31, 2022
Chief complaint, the stated reason for the acute care encounter given by the patient, was extracted from the electronic health record and categorized using methods employed by Brousseau et al. in which common postpartum conditions, such as vaginal bleeding and fever, were grouped separately and systems-based categories were created for other complaints. 5 Categories with a sample size <11 are not presented in accordance with policies about reporting small cell sizes.
Percent of total not including missing.
Chief Complaint for First Urgent Care Visits up to 12 Weeks After Discharge from the Birth Hospitalization in a Cohort of Birthing People Aged ≥18 Years Who Gave Birth to ≥1 Liveborn Infant at >20 Weeks of Gestation at a Quaternary Maternity Hospital in the Southeastern United States Between July 1, 2021, and December 31, 2022
Chief complaint, the stated reason for the acute care encounter given by the patient, was extracted from the EHR and categorized using methods employed by Brousseau et al. in which common postpartum conditions, such as vaginal bleeding and fever, were grouped separately and system-based categories were created for other complaints. 5 Categories with a sample size <11 are not presented in accordance with policies about reporting small cell sizes.
Percent of total not including missing.
Discussion
Key findings
In this cohort of birthing people, one in ten had one or more outpatient postpartum acute care encounters and one in 30 had one or more hospital readmissions within 12 weeks of discharge from the birth hospitalization. On average, first hospital readmissions occurred 6 days after discharge and outpatient postpartum acute care encounters occurred 10 days after discharge. Hypertension and hypertensive-related conditions were a leading medical indication for both outpatient postpartum acute care encounters and hospital readmissions. The timing of first postpartum acute care encounters, first outpatient postpartum acute care encounters, and first hospital readmissions varied by medical indication, with the majority of visits for hypertension and hypertensive-related conditions occurring within the first week of discharge for both outpatient encounters and hospital readmissions.
Results in the context of what is known
In our study, 11.3% of birthing people had ≥1 outpatient postpartum acute care encounter and 3.2% had ≥1 hospital readmission within 12 weeks of discharge from the birth hospitalization. These findings are largely consistent with previous studies, and differences observed are likely explained by variation in duration of postpartum follow-up and demographics of the study population, including payor mix. In previous studies, hospital readmissions varied from 1.2% within 90 days in a population-based cohort in California to 6.6% within six months of delivery in a Medicaid population delivering at a regional perinatal care center in the Mid-Atlantic. 8,10 Previous studies found that ED visits varied from 5% within 42 days of delivery among birthing people who delivered at a tertiary care women’s hospital to 35% within six months of delivery in a Medicaid population delivering at a regional perinatal care center in the mid-Atlantic. 5,8 Existing evidence suggests that ED visits and hospital readmissions peak in the first one to two weeks after discharge from the birth hospitalization. 6,7,10 Consistent with these results, we found that outpatient PACU occurred, on average, 10 days after discharge from the birth hospitalization and that hospital readmissions occurred, on average, 6 days after discharge. This study and the growing literature on this topic highlight the need to restructure postpartum care so that birthing people engage with their maternity care provider within the first few days of discharge from the birth hospitalization. 22 Doing so may help to identify and intervene on postpartum health concerns early, providing reassurance and care to birthing people who may be uncertain about what is normal in the postpartum period 43 and, potentially, preventing PACU.
NH Black birthing people in the United States disproportionately experience adverse maternal health outcomes. 23,24 In our study, NH Black individuals comprised 21% of the study population, but accounted for 28% of outpatient PACU and 32% of hospital readmissions, providing additional evidence that disparities in maternal health and health service use persist into the postpartum period. Nationally, Hispanic women have a lower pregnancy-related mortality ratio than NH White women and a rate of SMM that is higher than that of NH White women and lower than that of NH Black women. 23,24 In our study, Hispanic birthing people made up 27% of the population and comprised 22% of outpatient PACU and 31% of hospital readmissions; this burden of hospital readmissions could indicate that Hispanic individuals continue to experience a higher burden of life-threatening complications, indicated by hospital readmissions, in the postpartum period. While NH White women made up 40% of the study population and 41% of outpatient PACU, they accounted for only 30% of hospital readmission.
Our findings should be considered in the context of structural factors, including policies governing postpartum insurance coverage, which likely impact postpartum health care utilization. Birthing people with insurance coverage may attend more scheduled postpartum visits and may have fewer preventable hospital readmissions and ED visits than those who lack insurance. 25 Prior to 2020, coverage for some birthing people with North Carolina Medicaid ended after approximately two months postpartum; during our study, which assessed PACU from July 2021 through March 2023, NC Medicaid coverage extended through one year postpartum. 26 –28 In this analysis, 52% of births were covered by Medicaid, Medicare, or self-pay. We found this population accounted for 63% of hospital readmissions, suggesting a higher incidence of serious complications.
In our study, individuals with Cesarean sections, non-transfusion SMM at delivery, a high comorbidity score, or the presence of a major mental health disorder had disproportionately high PACU compared to their proportion of the total sample. Existing literature demonstrates associations between postpartum hospital use and birth complications, including SMM and long length of stay, as well as certain birth characteristics, including Cesarean mode of delivery. 10
In the United States, mental health conditions are the leading underlying cause of pregnancy-related deaths. 1 In our study, birthing people with a major mental health disorder had a higher incidence of outpatient PACU and postpartum hospital readmissions compared with the proportion of the total sample that they made up, consistent with other studies. A study using all-payer claims data in Maine found that people with prenatal depression had nearly twice the rate of acute health care use in the first two years postpartum compared with those without prenatal depression. 29 A retrospective cohort study at an academic medical center reported that 6.6% of birthing people with mental health disorders used the ED within 30 days of delivery compared to 3.6% of birthing people without a mental health disorder, and anxiety and depression were the mental health conditions with the highest risk of ED use. Birthing people with mental health disorders had more presentations for hypertension and psychiatric evaluations than those without mental health disorders, and most of these visits occurred in the first two weeks after delivery. 30 Our findings support and extend existing evidence that birthing people with mental health conditions utilize postpartum acute care more often than those without mental health conditions, suggesting that this population may have unmet postpartum health needs.
Hypertension and hypertensive-related conditions was a leading medical indication for both outpatient PACU and hospital readmissions in our study and are a leading cause of pregnancy-related deaths in the United States, particularly among NH Black women. 1,31 Existing studies report that hypertension and hypertensive disorders are leading visit indications for postpartum ED visits and hospital readmissions as well. 5,7,10 In our study, nearly all postpartum acute care encounters for hypertension and hypertensive-related conditions occurred within the first week after discharge from the birth hospitalization, before many birthing people attend a postpartum maternity visit.
Strengths and limitations
We constructed this cohort using EHR data from a quaternary hospital within a large health care system that has 17,000 births per year, accounting for one in seven North Carolina births. 32 The EHR data used in this study contain a high density of information regarding patient sociodemographic factors, pregnancy and birth characteristics, and health service use. Thus, we were able to describe patterns of PACU by an array of sociodemographic and medical factors, allowing us to identify who is most vulnerable to PACU and might benefit from tailored postpartum medical care. Because the EHR data contain date of discharge from the birth hospitalization, we calculated the timing of postpartum acute care encounters based on the birthing person’s discharge date, avoiding issues of immortal person-time that could present if birth date was used instead. 11 Our study includes a broad range of acute care visit locations, with both outpatient locations and hospital readmissions, to comprehensively assess PACU. Notably, we included visits to OB triage in the outpatient PACU outcome. OB triage is used to screen and evaluate OB patients; some are connected to hospital labor and delivery units, while others are located elsewhere. 33 OB triage is a prominent source of acute care in the early postpartum period; in our analysis, 30% of first postpartum acute care encounters took place at an OB triage location. Finally, we used a published classification system to describe acute care visits by clinically meaningful indications and demonstrated that the timing of acute care visits varies by indication, which has important clinical implications.
This study has several limitations. First, the cohort analyzed herein is not a population-based sample, so our findings may not be representative of PACU trends in other settings and populations. Second, postpartum health service use outside of the UNC Health System, including acute care encounters and maternity visits, is not observed in these data. Thus, PACU and maternity visit attendance are likely underestimated in this study. Third, we cannot observe if, when, and for what reasons individuals seeking postpartum acute care were not able to obtain it, which are important questions for future research. Fourth, missingness and data constraints limit our ability to incorporate social drivers of health, such as educational attainment, upstream determinants of health, such as structural racism, and features of acute care encounters, such as chief complaint for all visit types, into this analysis. Fifth, the administrative data used to categorize medical indications were nonspecific or missing for many encounters, limiting our ability to describe the reason for the encounter. Finally, while preventing “unnecessary” PACU is a sensible goal, PACU for true emergencies is an appropriate and important use of health care. In a recent commentary, authors representing the Society for Maternal-Fetal Medicine noted several limitations of postpartum hospital readmission as a quality metric. 34 We posit that these concerns are also relevant for outpatient PACU and contend that researchers and policymakers must thoughtfully measure and interpret PACU as an indicator of postpartum health and health needs in light of these constraints.
Implications for practice and research
Usual postpartum care consists of a single visit around six weeks after birth. 22 In this context, it is not surprising that most people who had a postpartum hospital readmission in our study did not attend a maternity visit beforehand. Existing studies highlight that many birthing people feel unprepared for the postpartum period. 35 –40 and those who have postpartum complications feel fear. 41,43 Routine systems of perinatal health must be reformed and reimagined to better support postpartum health and safety. 42
Our findings underscore the importance of routine, scheduled follow-up in the early postpartum period. The American College of Obstetricians and Gynecologists recommends that all birthing people have a comprehensive postpartum visit within three weeks of birth and ongoing follow-up as needed and recommends that high-risk individuals have earlier follow-up, which should occur within one to three weeks of birth. 22 Our findings suggest that early follow-up may be beneficial for all birthing people as the average time to first PACU not resulting in admission was ten days post-discharge and the average time to first hospital readmission was six days. A scheduled visit in the first few days after discharge from the birth hospitalization may help meet the postpartum health needs of birthing people and prevent PACU; such early postpartum care may be especially important for those who disproportionately utilize postpartum acute care and are readmitted to the hospital.
These results also suggest that the timing of PACU varies by visit indication, highlighting windows of time that precede PACU during which intervention and follow-up may be beneficial. For example, to address the health needs of people who would utilize acute care for hypertension and hypertensive-related conditions, home visits or at-home blood pressure monitoring in the first few days after hospital discharge may help to identify and address complications early, potentially avoiding PACU. The design of interventions that proactively address postpartum health needs should be the focus of future work.
Conclusion
In this study of birthing people in a health care system in the Southeastern United States, PACU was common and occurred shortly after discharge from the birth hospitalization. On average, PACU that did not result in readmission occurred 10 days post-discharge, and hospital readmissions occurred 6 days post-discharge, indicating a need for postpartum follow-up soon after discharge. Early follow-up is particularly important for groups with a high incidence of PACU, including individuals with public insurance, non-Hispanic Black race/ethnicity, and one or more babies in the NICU, and it is also important for individuals at high risk for common PACU visit indications, including hypertension and hypertensive-related conditions. These findings can inform efforts to direct health resources to improve postpartum health care and health outcomes.
Footnotes
Authors’ Contributions
C.E.B.: Conceptualization, methodology, formal analysis, writing—original draft, writing—review and editing, visualization, supervision, and project administration. B.W.P.: Conceptualization, methodology, and writing—review and editing. C.J.V.: Conceptualization, methodology, and writing—review and editing. C.T.: Conceptualization and writing—review and editing. K.T.: Conceptualization, methodology, and writing—review and editing. A.M.S.: Conceptualization, methodology, resources, data curation, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
The authors report no conflict of interest.
Funding Information
This research was supported in part by a training grant from the National Institute of Child Health and Development (
Supplementary Material
Supplemental Supplementary Figure S1
Supplemental Supplementary Table S1
Supplemental Supplementary Table S2
Supplemental Supplementary Table S3
Supplemental Supplementary Table S4
Supplemental Supplementary Table S5
Supplemental Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.