
Abstract
Introduction:
The 2021 update to the United States Preventive Services Task Force guidelines for lung cancer screening (LCS) aims to reduce disparities derived from sex, race/ethnicity, and socioeconomic status. Few studies have addressed adherence to LCS among female Veterans.
Methods:
To evaluate differences in adherence to LCS by sex, we conducted a retrospective cohort study within the VA Connecticut LCS Program between June 2013 and March 2020. Our primary outcome was nonadherence, defined as lack of completion of a chest CT scan within the guideline recommended interval plus a 90-day grace period. Eligible patients were enrolled in the screening program and had a baseline Lung-RADS score of 1, 2, or 3. Patients with Lung-Reporting and Data System (RADS) 4 were excluded due to variability in follow-up recommendations. We adjusted for age, race, smoking history, mental/medical comorbidities, and primary care (PC) visits (1-year after first/index CT). Logistic regression modeling was used to determine associations between sex and nonadherence overall and stratified by Lung-RADS 1–2 and Lung-RADS 3.
Results:
Among 4,711 Veterans, the overall rate of nonadherence was 34%. Female Veterans were 66% more likely nonadherent to follow-up (odds ratio [OR] = 1.66, confidence interval [CI] = 1.19–2.30) compared with male Veterans. Substance use disorder was associated with greater nonadherence (OR = 1.22, CI = 1.01–1.47). Lower nonadherence was observed among patients with COPD (OR = 0.77, CI = 0.66–0.9) and PC engagement (OR for nonadherence with 5 or more PC visits = 0.78, CI = 0.67–0.91). The associations between sex and nonadherence were similar in models stratified by Lung-RADS groups 1–2, although did not reach significance for the Lung-RADS 3 group.
Discussion:
In this cohort, female Veterans were more likely nonadherent. More work is needed to understand the distinct barriers to LCS follow-up among female Veterans. Health care system engagement significantly reduced nonadherence, which may partially explain higher rates of nonadherence among female Veterans who had fewer medical comorbidities.
Introduction
Lung cancer remains the leading cause of cancer-related death in the United States. The National Lung Screening Trial (NLST) showed that sequential low-dose CT scans (LDCT) reduce lung cancer-related mortality by 20%. 1 While adherence to follow-up in clinical trials exceeds 90%, real world estimates of adherence through lung cancer screening (LCS) programs is only 22.3%. 2 Because most lung cancers are found during follow-up imaging, optimizing adherence to follow-up is critical for reducing mortality. 2
Health care disparities impact all aspects of LCS including eligibility, participation, adherence, and outcomes. 2 –7 With higher rates of tobacco smoking than the general population, the implementation of LCS in Veterans is particularly important. 8 Available studies show that women had been less likely to be eligible for LCS based on pack-year smoking history; however, may benefit more from LCS. 9 The United States Preventive Services Task Force (USPSTF) LCS guidelines were updated in 2021 to include younger patients (minimum age decreased from 55 to 50 years) and fewer pack-year smoking history (reduced from 30 pack-years to 20). These changes are expected to result in an 81% increase in US adults being eligible for LCS (approximately 6.3 million additional patients) from the original 2013 recommendations. Initiating screening for an age-broadened population starting age 50 and reducing smoking history to 20 pack-years is likely to result in a higher relative increase of the female population eligible for screening, more lung cancer deaths averted, as well as life-years gained in the female population when compared with men. 10 While women account for approximately 15% of enrolled Veterans, enlistment is increasing, 11 and the effect of sex on LCS adherence is under-studied. To address this knowledge gap, we determined how sex impacted LCS adherence among patients enrolled in a single-center VA program.
Methods
We retrospectively analyzed a prospective cohort of Veterans participating in the VA Connecticut Health care System’s LCS program between June 2013 and March 2020. The observation period ended due to interruptions in health care delivery by the COVID-19 pandemic. Patients were referred for LCS based on USPSTF 2013 eligibility criteria (age 55–80, at least 30 pack years of smoking, current or former smokers with quit date within the last 15 years) (Fig. 1). 12 At the time of this study, the VA Connecticut Health care system utilized a hybrid centralized system for follow-up LDCT scans. During the initial implementation, LCS initiation was prompted using an electronic clinical reminder in the electronic health record As the program matured, the hybrid structure meant that patients could be followed either by their primary care (PC) provider or by the LCS nurse coordinator, 13 which began a phased introduction in late 2018. LDCTs were ordered either due to prompting by a clinical reminder in the electronic health record or could be initiated independently of the reminder.
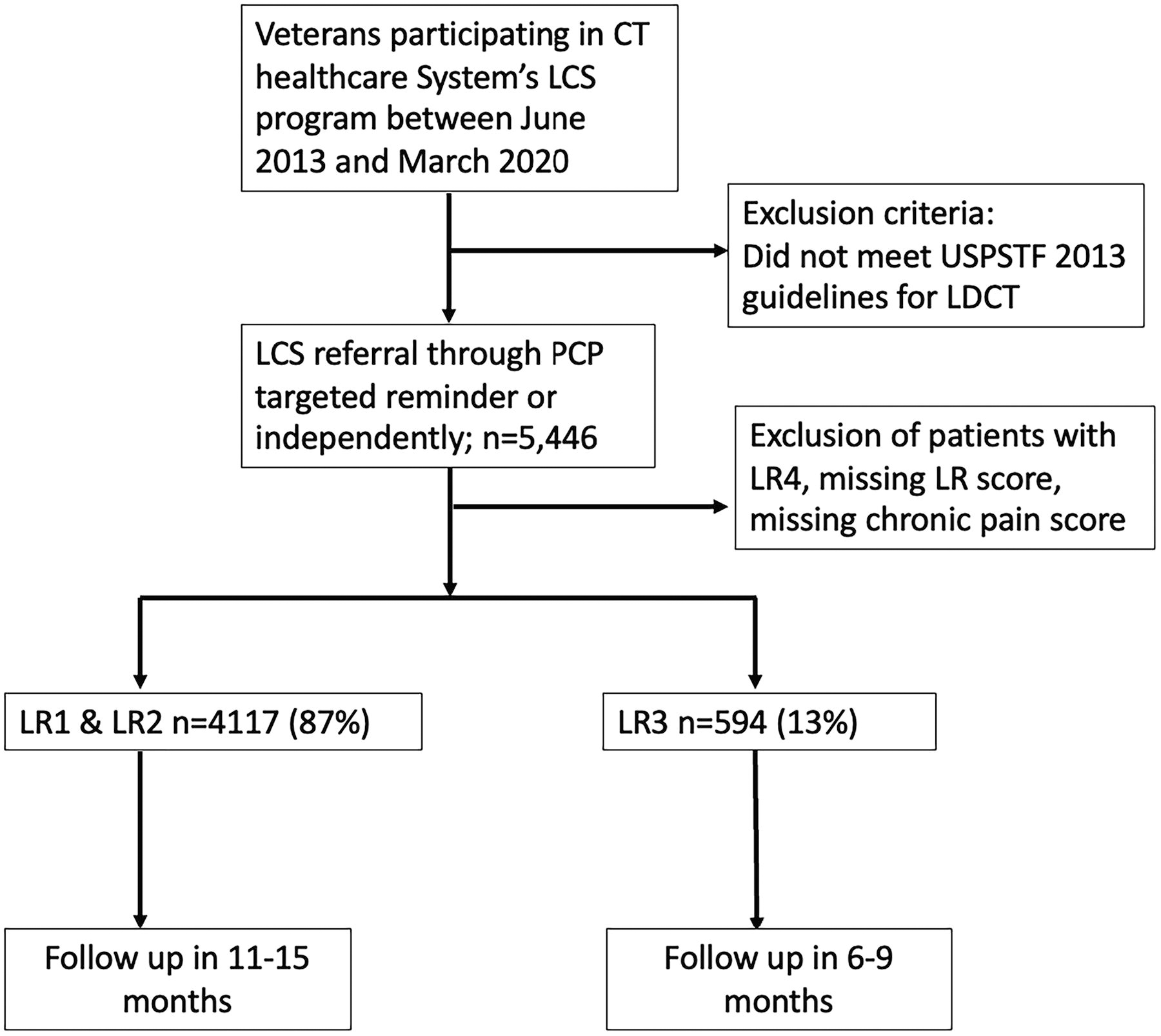
Flow diagram for patient enrollment and follow-up time interval.
Our primary outcome was nonadherence to first follow-up LDCT. Consistent with the NLST, nonadherence was defined as lack of evidence of VA-based LDCT within 90 days of the Lung-Reporting and Data System (RADS) (LR)-recommended interval from initial LDCT. 1,14 An LR score of 1 or 2 recommends follow-up in 12 months; thus, nonadherence was defined as no LDCT within 15 months of the initial scan. For an LR score of 3, follow-up in 6 months is recommended: nonadherence was defined as lack of LDCT within 9 months of initial scan. LR scoring (range 1–4) was extracted from clinical radiology reports or was applied based on reported nodule presence/dimensions, when available. We excluded patients with LR4 because follow-up included multiple diagnostic tests and interventions, which potentially included non-VA care (specialized scans, biopsies, and referral to a tumor board).
Exposure of interest was sex. Sex was defined as a self-reported binary variable of either male or female. Covariates included self-reported race and ethnicity (Veterans were able to self-identify as White/Black/Hispanic/Asian/AN/AI/Other), smoking status (current/former ascertained from VA Health Factors Data), 15 medical comorbidities (diabetes mellitus, asthma, congestive heart failure, chronic obstructive pulmonary disease, coronary artery disease, and hypertension), and mental health diagnoses (schizophrenia, major depressive disorder, post-traumatic stress disorder, bipolar disorder); comorbidities were determined by ICD-9/ICD-10 diagnosis codes. Chronic pain was determined by three pain intensity scores ≥4 in separate months in the past year that were documented during vital sign measurement. PC engagement was defined as number of PC visits during the 12 months following initiation of LCS; we grouped number of visits as 0, 1–4, or 5 or more.
Chi-square tests were used to assess bivariate relationships in categorical variables and Student t-tests for continuous variables. We used standard multivariable logistic regression models to determine associations between sex and nonadherence, adjusted for race/ethnicity combined into two categories (White and non-White) due to limited sample size (Black men = 13.41%, women = 11.46%; Hispanic men = 6.46%, women = 9.56%; American Indian/Alaskan Native men = 0.02%, women = 0.00%; Asian American/Pacific Islander men = 0.39%, women = 0.64%; Other men = 0.54%, women = 0.00)), 16 smoking status, substance use disorder, mental health conditions, comorbid medical conditions, and PC engagement. Multicollinearity was tested and not found reviewing tolerance, variance inflation, and collinearity diagnostics between the variables. Analysis was conducted using SAS Version 9.4. This study received full IRB approval.
Results
Among 5,446 Veterans (women 3.30%) enrolled in LCS, we excluded 735 because they had a LR4 nodule, did not have an assigned LR score, or did not have a chronic pain score leaving a total of 4,711 Veterans who were included in the model. The majority had LR1 or LR2 disease (n = 4,117, 87%) and fewer had LR3 nodules (n = 594, 13%).
Compared with male veterans, women were younger (mean age = 59.8 years SD 5.3 versus 63.9 years SD 6.1, p < 0.0001; Table 1), more likely to be current smokers (87.3% versus 74.6%, p = 0.0003), and more likely to have chronic pain (26.9% versus 19.1%, p = 0.01). Mental health conditions and asthma were more common in women, whereas other medical comorbidities were less common in women.
Multivariable Logistic Regression Models Overall and Stratified by Lung-RADS 1–2 Only, Lung-RADS 3 Only a
Data are bolded because they meet statistical significance with a confidence interval that crosses 1.0.
Also adjusted for age (years), non-White race, chronic pain, schizophrenia, PTSD, Major Depression, Bipolar, Diabetes, Asthma, Congestive Heart Failure, COPD, CAD, and Hypertension.
CAD, Coronary Artery Disease; COPD, Chronic Obstructive Pulmonary Disease; RADS, Reporting and Data System; PTSD, Post Traumatic Stress Disorder.
Overall nonadherence was 34% and varied with sex: women = 47% versus men = 34%. In adjusted logistic regression models, female sex was associated with 66% increased odds for nonadherence to follow-up (odds ratio (OR) = 1.66, [95% confidence interval (CI) = 1.19–2.3]; Table 2; Supplementary Table S1 for full mode results) compared with male sex. PC engagement with five or more visits during time of follow-up was significantly associated with decreased nonadherence (OR = 0.78 [0.67–0.91]).
Factors Associated with Lung Cancer Screening Nonadherence Stratified by Lung RADS 1–2 and Separately Lung RADS 3
Data are bolded because they meet statistical significance with a confidence interval that crosses 1.0.
CI, confidence interval; OR, odds ratio; CHF, Congestive Heart Failure; CAD, Coronary Artery Disease, COPD; Chronic Obstructive Pulmonary Disease
In patients with negative baseline LDCTs (Lung-RADS 1–2), nonadherence to follow-up remained higher in women (OR = 1.66 [1.17–2.36]) and patients with substance use disorder (OR = 1.26 [1.03–1.54]). Nonadherence was lower in patients with COPD (OR = 0.78 [0.66–0.92]). More annual PC visits were associated with lower nonadherence: five visits versus zero visits (OR = 0.79 [0.67–0.92]).
In patients with positive baseline LDCT (Lung-RADS 3), only current smoking status significantly associated with nonadherence (versus former smokers; OR = 1.86 [1.15–3.11]). There was no association with sex (OR = 1.83 [0.64–4.93]).
Discussion
Female sex was associated with nonadherence to LCS follow-up in our Veteran population. Our observation that female Veterans have a higher rate of nonadherence to LCS follow-up compared with male Veterans is in contrast to prior studies, which have suggested higher adherence to follow-up in civilian women participating in LCS. 17,18 It is notable that in another investigation of over 28,000 Veterans (of whom 94.8% were men), there was no association between female sex and adherence to follow-up scans (OR = 1.10, CI = 0.95–1.20). 19 There are several potential explanations for lower rates of adherence among female Veterans in our cohort.
First, medical comorbidities likely contribute to likelihood of obtaining follow-up. In non-Veteran patients eligible for LCS, those with a higher burden of medical and smoking-related comorbidities were found to have a higher likelihood of LCS utilization. 20,21 The women in our cohort had fewer medical comorbidities, potentially influencing how preventive practices such as LCS are perceived or acted upon by patients, as well as reducing opportunities for the patient to be on site to receive the CT scans. While we anticipated that less engagement with the health care system due to lower rates of medical comorbidities compared with men would impact adherence, we continued to observe an association between female sex and nonadherence even after adjusting for PC use. Whether counseling of female Veterans with more tailored messaging around the importance of follow-up CT scans could improve adherence is also important to address. It is also possible that differential experiences with the military such as military sexual trauma could negatively impact female Veterans’ abilities to complete follow-up CT scans.
Second, differences in mental health diagnoses may also contribute to nonadherence by sex. Prior studies of post-deployment Veterans showed that women were more likely to have PTSD (OR = 5.28), depression (OR = 3.09), and suicidal thoughts (OR = 2.59) compared with men and that over half reported that their mental health needs were not completely met by the VA. 22 Female Veterans in the current study were more likely to have major depressive disorder and bipolar disorder, which are associated with higher rates of nonadherence to LCS. 7,19 Targeted evaluation of the impact of mental health comorbidity burden and how to promote a safe and accessible “medical home” for female Veterans are needed to promote engagement overall and improved LCS adherence.
Finally, stigma has been shown to influence medical-seeking behavior and to decrease patient engagement. 23 In prior work, lung cancer stigma was associated with longer time to seek attention for symptoms and delayed medical help-seeking behavior. 23 Tobacco screening and smoking cessation efforts have also been marred by stigma. 24 We speculate that smoking and lung cancer-related stigma may differentially impact women versus men and contribute to lower rates of LCS adherence. For example, in a series of narrative interviews conducted by Antin et al. women who smoked felt stigmatized due to its association with “irresponsible citizenship” and masculinity. 25 Adjusting tools used to counsel patients about smoking and related health hazards may be important to be heard by women who smoke in a way that is compassionate and effective.
Our study has several limitations. First, we reported LCS adherence from a single clinical site that was an early LCS adopter during a period of decentralized LCS; follow-up studies are needed to determine the effectiveness of VA’s national LCS campaign through the Lung Precision Oncology Program to mitigate sex disparities to LCS adherence. Second, we also did not ascertain follow-up outside the VA. Third, we were limited in the racial and ethnic diversity of the patients included, leaving us insufficiently powered to examine the intersectionality between sex and race and ethnicity and LCS nonadherence. Fourth, in our electronic medical record-based approach, our study was unable to accurately ascertain number of pack-years smoked for each patient. 26 –28 Finally, we used 2013 LCS criteria, which have since been revised to offset disparities by sex for lung cancer risk.
Our study suggests that female Veterans are less adherent to LCS follow-up. Future research is warranted across the VA system to determine how LCS enrollment and adherence varies by sex, identify barriers to adherence, and implement strategies tailored to women’s health within the VHA. Our findings are of particular importance given that the updated 2021 USPSTF LCS guidelines intend to increase the number of women who are eligible for and participating in LCS. Thus, it is possible that selected populations may experience more benefit from the updated USPSTF guidelines based on their ability to participate or obtain follow-up testing. As LCS programs have evolved in the years since our data collection, various strategies have been implemented that significantly reduced rates of nonadherence. For example, centralizing a LCS program with a dedicated nurse coordinator has been shown to improve adherence. 17 It is possible that further centralization of our LCS program will further mitigate sex-based disparities in nonadherence to follow-up.
Authors' Contributions
All authors contributed to the data processing, writing, and editing of the manuscript.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.