
Abstract
Introduction:
In the first year postpartum, hypertension is a leading cause of morbidity and mortality, particularly for those with hypertensive disorders of pregnancy (HDPs). Given that timely recognition of hypertension is key to reducing short- and long-term cardiovascular risk, we assessed knowledge of when to seek medical attention for blood pressure (BP) elevations and rates of BP measurement in the first year postpartum.
Methods:
This was a secondary analysis of a cohort of 405 primiparas who enrolled in a randomized trial during pregnancy. We calculated the proportion who stated they would contact a clinician for a systolic BP above 140 and a diastolic BP above 90 at 3 months postpartum, and the frequency and location of BP checks reported from 2 to 12 months postpartum by HDP status.
Results:
HDPs were reported by 16% of participants. Mean age was 32 ± 5 years; 40% identified as non-White, and 25% had public insurance. At 3 months postpartum, 44.6% with HDPs and 23.5% without identified a systolic BP of 140 as the threshold above which to contact a clinician (p < 0.01); 52.4% with HDPs and 28.5% without identified a diastolic BP threshold of 90 (p < 0.01). From 3 to 12 months postpartum, people with HDPs were more likely to report a BP check (83.1% versus 59.4%, p < 0.01) and home BP monitoring (41.6% versus9.7%, p < 0.01). Home monitoring was not associated with awareness of when to seek help for hypertension among those with HDPs.
Conclusions:
Efforts are needed to improve awareness of when to seek medical attention for postpartum hypertension.
Introduction
Hypertensive disorders of pregnancy (HDPs), including chronic hypertension, gestational hypertension, and preeclampsia, are major causes of maternal morbidity and mortality worldwide. 1 In the first 42 days postpartum, HDPs contribute to nearly 1 out of 10 maternal deaths in the United States. 2 Of those with HDPs, blood pressure (BP) elevations often persist, such that more than half have chronic hypertension in the 12 months after delivery. 3 Over the life course, HDPs are associated with higher risk of cardiovascular disease, including myocardial infarction, stroke, and heart failure, and are recognized by the American Heart Association and the American College of Cardiology as risk-enhancing factors for cardiovascular disease. 4,5
Prompt recognition and treatment of hypertension during the postpartum period are key to reducing both short- and long-term cardiovascular risk. The American College of Obstetricians and Gynecologists and the International Society for the Study of Hypertension in Pregnancy recommend that people with HDPs have an early postpartum BP check within approximately 7 days postpartum and be counseled regarding the importance of ongoing care with a primary care clinician. 6,7 However, U.S. health insurance claims data demonstrate that, even by 6 months postpartum, less than 60% of people with HDPs had visited any health care provider who routinely checks BP. 8 Substantial differences in postpartum care exist by social determinants of health in both the United States and abroad, with lower rates of follow-up observed among those who identify as Hispanic or non-Hispanic Black, have lower income, or live in rural areas. 8,9
In a recent scientific statement, the American Heart Association identified home BP monitoring as a potential strategy to improve equity in postpartum BP monitoring and treatment. 10 Success of home BP monitoring relies not only on the availability of BP cuffs but also on patient knowledge of when to seek treatment of hypertension. Contemporary rates of postpartum home BP monitoring among people with HDPs are poorly understood. Furthermore, how often postpartum people are aware of when to seek care for an elevated home BP is unknown.
Therefore, we aimed to describe the frequency and location of BP measurement, as well as BP-related knowledge in the first year postpartum among those with HDPs and without HDPs. Recognizing the importance of social drivers of health-related behaviors and knowledge, we additionally explored variation in BP measurement and knowledge by social factors.
Methods
This was a secondary analysis of a cohort of U.S.-born primiparas who participated in a randomized trial examining the effects of prenatal counseling about the benefits of lactation or smoking cessation (NCT04601987). 11 The Institutional Review Board of the University of California San Francisco approved the original study. Eligible participants included U.S.-born individuals who were carrying a singleton pregnancy of at least 28 weeks, able to read English, and had reliable access to a device with internet access. Exclusion criteria were prior births, carrying multiple gestations, not planning on giving birth, use of reproductive technology, and inability or contraindication to breastfeeding. Participants were asked to self-report sociodemographic and health-related information on enrollment in their 2nd or 3rd trimester and on multiple occasions postpartum. At the 3-, 6-, 9-, and 12-month postpartum assessments, participants were asked if their BP was measured within the past month, as well as the location of the BP check (i.e., clinic, home, hospital, emergency room, pharmacy). At the 3-month postpartum visit, participants were asked “At which BP should a new mother contact a clinician because her BP is too high?”
For this analysis, we included 405 participants who self-reported information on BP checking at any postpartum assessment. HDPs were defined as self-reported chronic (prepregnancy) hypertension, gestational hypertension, preeclampsia, or use of antihypertensive medication before pregnancy, during pregnancy, or before 12 weeks postpartum. We calculated the proportion of people with and without HDPs who self-reported a BP check at any time within the first year postpartum, as well as the timing, frequency (median [interquartile range or IQR]), and location (health care facility only, home only, or both) of BP measurement. We additionally calculated the percent of people who stated they would contact a clinician for a systolic BP above 140 and a diastolic BP above 90 at 3 months postpartum, overall by HDP status and among people who checked their BP at home. Secondarily, we calculated the percent who identified systolic BP thresholds of <119 mmHg, 120–129 mmHg, 130–139 mmHg, 140–149 mmHg, 150–159 mmHg, and ≥160 mmHg, as well as the percent who identified a diastolic BP threshold ≤79 mmHg, 80–89 mmHg, 91–99 mmHg, 100–109 mmHg, and ≥110 mmHg.
We compared responses among those with and without HDPs using t tests for continuous variables and chi-squared for categorical variables. Exploratory subgroup analyses were conducted with consideration of the following sociodemographic and pregnancy-related factors: age (<35 or ≥35 years old), insurance (private or government), educational status (<college or ≥college), self-identified race/ethnicity, family history of hypertension, and gestational diabetes.
Results
Participants’ mean age was 31.6 (standard deviation or SD 4.9), 84.0% had at least a college education, 74.8% had private insurance, and 19.5% self-identified as African American or Black, 6.2% Asian, 4.9% Hispanic or Latina, and 59.5% White (Table 1). HDPs were reported by 65 (16.1%) participants, of which 6 (1.5%) reported chronic hypertension. People with HDPs were more likely to be of advanced maternal age (≥35 years old), have prepregnancy obesity, and a family history of hypertension (p < 0.05).
Characteristics of Study Population
HDP: hypertensive disorder of pregnancy.
p-Value comparing people with and without HDPs.
SD, standard deviation.
Of those with HDPs, 83.1% reported having their BP checked at least once from 2 to 12 months postpartum; the median number of BP measurements among these participants was 3 (IQR 0, 8) times; 41.5% had their BP checked only at a health care facility, 10.8% checked their BP only at home, and 30.8% checked their BP both at home and at a health care facility (Table 2). The majority (63.1%) had a BP check between 2 and 3 months postpartum. People without HDPs checked their BP less frequently (median 0 [IQR 0, 3]) and were less likely to have a BP check at any point in the first year postpartum (59.4%), to check their BP at home (3.2% home only, 6.5% both home and health care facility), and check their BP between 2 and 3 months postpartum (27.7%) (p < 0.01).
Frequency and Location of Blood Pressure Assessments in the First Year Postpartum Among People With and Without Hypertensive Disorders of Pregnancy
HDP: hypertensive disorder of pregnancy.
p-Value comparing people with and without HDPs.
SD, standard deviation; IQR, interquartile range.
At 3 months postpartum, 44.6% of people with HDPs reported that they would contact a clinician if their systolic BP was ≥140 mmHg and 52.3% if their diastolic BP was ≥90 mmHg (Table 3). Of the six people with chronic hypertension, one (16.7%) identified a systolic BP of 140 or a diastolic BP of 90. People without HDPs were less likely to identify a systolic BP threshold of 140 mmHg (23.5%) and a diastolic threshold of 90 mmHg (28.5%), p ≤ 0.01. Among those who checked their BP at home, 44.4% of those with HDP and 39.4% of those without HDP identified a systolic BP threshold of 140 mmHg.
Awareness of Need to Contact a Clinician for Hypertension by Hypertensive Disorder Status and Blood Pressure Checking Behaviors Postpartum
HDP: hypertensive disorder of pregnancy.
p-Value comparing people with and without HDPs.
In secondary analyses of systolic BP ranges, 9.2% with any HDPs identified a BP threshold from 130 to 139, 13.9% identified a BP of 150 to 159, and 13.9% identified a BP ≥160 mmHg. For diastolic BP, 13.9% identified a BP of 80–89, 12.3% a BP of 100–109 mmHg, and 6.2% a BP ≥110 mmHg (Fig. 1). Compared with those with HDP, people without HDP were less likely to provide an answer to the BP threshold at which they would contact a physician and identify a systolic BP of 140–149 mmHg or 150–150 mmHg and a diastolic BP of 90–99 mmHg.
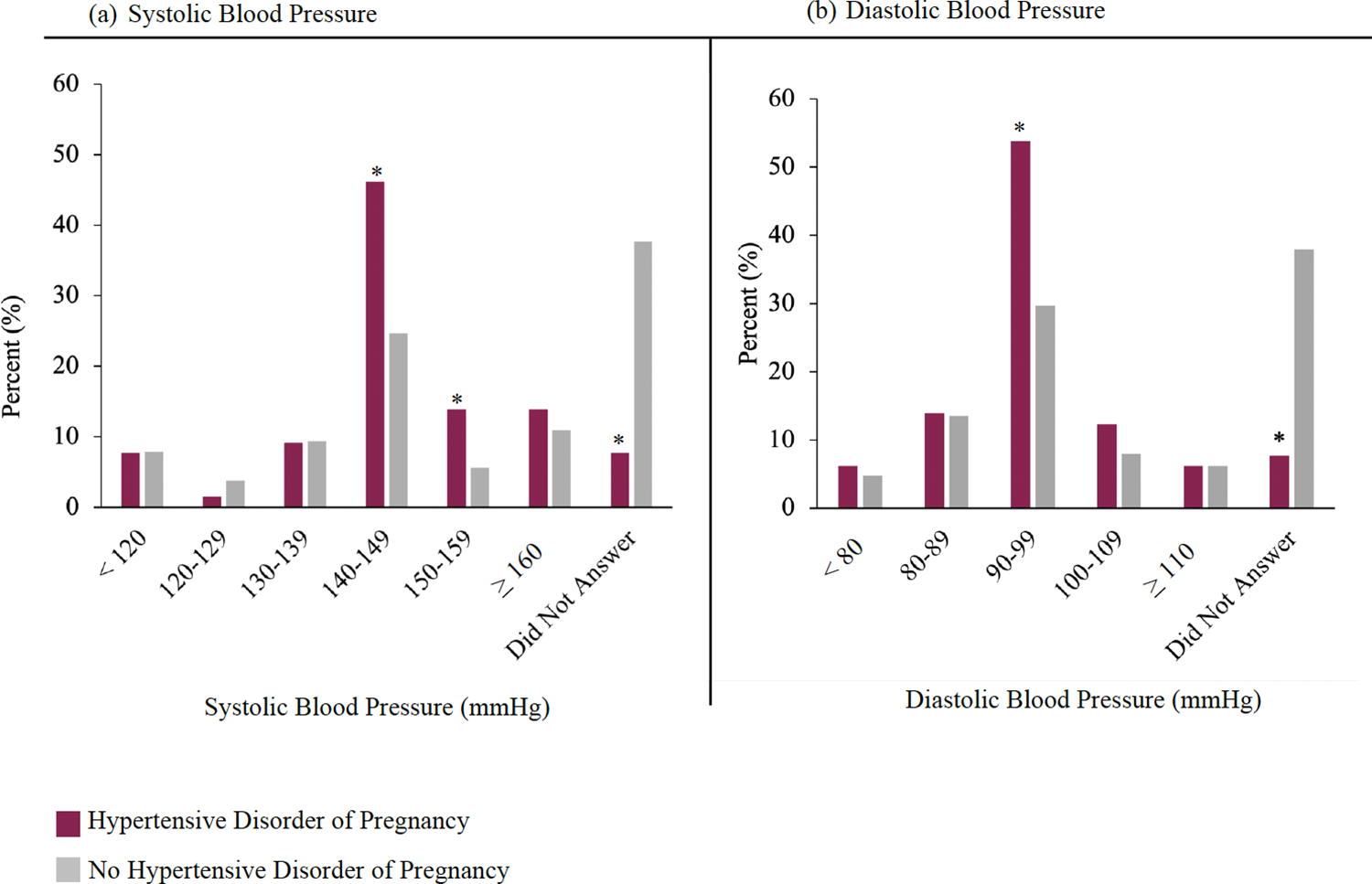
Systolic
In an exploratory subgroup analysis by sociodemographic and pregnancy-related factors, postpartum BP measurement and knowledge of when to contact a clinician for BP elevations were slightly higher among people with private insurance, who had at least a college education, identified as White, or had a family history of hypertension, although not all comparisons were statistically significant (Supplementary Tables S1 and S2). Family history of hypertension was associated with knowledge of when to contact a clinician for BP elevations among those without HDPs, but not among those with HDPs.
Discussion
In this sample of primiparous postpartum people recruited across the United States, approximately 80% of those with HDP and 60% of those without HDP had a BP check between 2 and 12 months postpartum. Although 40% of those with HDP and 10% of those without HDP reported checking their BP at home, knowledge regarding when to contact a clinician for BP elevations was poor. Less than half the people with HDPs or who checked their BP at home identified a systolic BP of 140 mmHg as the threshold above which they would contact a clinician because their BP was too high. Public health efforts are needed to improve postpartum BP assessment, self-monitoring, and awareness of when to seek medical attention for hypertension among birthing people with and without HDPs.
This study is unique in describing the frequency and location of BP monitoring during the first year postpartum, and in carefully considering home BP monitoring. Previous work using medical claims data has described rates of postpartum health care utilization, which typically includes routine BP checks. Similar to our study, claims data indicate that approximately 80% of people in the United States attend a health care visit in the first year postpartum. 12 However, only about half of these visits are for preventive care, even among those with HDPs who need counseling regarding BP and cardiovascular health optimization. 12,13 In the United Kingdom, where there is universal health care coverage, approximately 85% self-report attending a postpartum checkup with a clinician and 95% a home visit with a midwife. 14 Literature describing rates of home BP monitoring during the postpartum period in the United States and abroad remains limited. Outside of pregnancy, data from the National Health and Nutrition Examination Surveys from 2009 to 2014 demonstrated that approximately 50% of reproductive-age women with self-reported hypertension and 9% of those without hypertension engaged in home BP monitoring. These rates are similar to those reported among people with and without HDPs in the present study, respectively. 15
Despite utilization of home BP monitoring among people in this study, knowledge of when to contact a clinician for BP elevations during the postpartum period was poor. Data from nonpregnant people have similarly demonstrated that BP awareness is low, with less than 40% of reproductive-age individuals aware of a hypertension diagnosis in the United States, France, South Africa, Korea, and Iran. 16 –20 Among people with HDPs, single-center studies have shown that less than one-in-four people are aware of which HDP they were diagnosed with during pregnancy (e.g., chronic hypertension, gestational hypertension, or preeclampsia) or that preeclampsia can develop in the postpartum period. 21 In the current study, we found that less than half of people with HDP and less than one-quarter of people without HDP identified a systolic BP of 140 mmHg as the threshold above which they would contact a clinician because their BP was too high at 3 months postpartum. Furthermore, we observed differences in BP knowledge by social determinants of health, although comparisons were limited by small sample sizes. Less than one-third of people with publicly funded insurance or less than a college education correctly identified the BP threshold at which they should contact a clinician, regardless of HDP status.
Awareness of when to contact a clinician for BP elevations was greater among people with HDPs, overall, and within sociodemographic subgroups. This suggests that some BP-related education may be occurring during prenatal and early postpartum care among those with HDPs. However, awareness was still poor, even among people checking their BP at home. Given that hypertension is a leading cause of maternal morbidity and mortality, these results highlight the urgent need to improve BP-related knowledge among all birthing people. Small, single-center programs utilizing educational pamphlets and videos for people with HDPs have demonstrated some success in improving awareness of postpartum hypertension, symptoms of preeclampsia, and BP management strategies. 21,22 The Early Intervention to Promote Cardiovascular Health of Mothers and Children is an ongoing National Institutes of Health-funded program supporting a multicenter intervention utilizing home visitors to deliver educational modules to improve cardiovascular health during pregnancy and postpartum, including BP. Additional public health and policy changes are needed to support wider dissemination of BP-related awareness and knowledge before, during, and after pregnancy.
This study was strengthened by the availability of self-reported data on postpartum BP assessment and knowledge in a sample with 96% retention through 12 months postpartum. Therefore, we were uniquely able to characterize the frequency of clinic- and home-based BP monitoring, as well as knowledge regarding when to contact a clinician for BP elevations in the first year postpartum. Several limitations should be noted. First, sample sizes were small among those with HDP and within sociodemographic subgroups. Second, most people in this sample had private insurance and at least a college education, which is not representative of the U.S. birthing population. Therefore, we may have overestimated the frequency of postpartum BP checking and BP-related knowledge. Third, we did not have data on BP control of all participants and therefore could not determine if the frequency of BP monitoring and BP-related knowledge were associated with detection and control of hypertension during the first year postpartum.
In conclusion, in this national sample of postpartum people, less than half identified a systolic BP of 140 mmHg as the threshold above which they would contact a clinician because their BP was too high, even among people with HDPs or checking their BP at home. Among those with less than a college education or publicly funded insurance, less than one-third identified the correct BP threshold, regardless of HDP status. As such, public health efforts are needed to promote BP-related knowledge and awareness during pregnancy and the postpartum period.
Footnotes
Authors’ Contributions
N.A.C.: Conceptualization, methodology, formal analysis, and writing—original draft. H.B.: Data curation and writing—review and editing. E.B.S.: Conceptualization, methodology, resources, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
The authors have none to report.
Funding Information
Funding for Prenatal Counseling for Postpartum Health to E.B.S. (HRSA R40MC35364).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.