
Abstract
Background:
Stress has been found to be linked to adverse health outcomes. Having an objective measure of stress to complement validated self-reported stress measures is helpful for assessing the impact of interventions aimed at reducing stress and measuring its associations with health outcomes. Allostatic load is an objective measure that summarizes stress’s impact on multiple physiological systems. However, inconsistent combinations of indicators in an allostatic load index (ALI) are found in literature. The purpose was to (1) explore the ability to identify a set of indicators for inclusion in an ALI related to perceived stress and (2) explore the ability of the calculated ALI to identify an association between ALI and Perceived Stress Scale (PSS) score category among a small sample of women with HIV and comparable women without HIV.
Materials and Methods:
Data were from participants of the Women’s Interagency HIV Study in the United States during 2014–2019 whose PSS score on the PSS-10 questionnaire were in the highest (n = 103) and lowest (n = 103) quartiles for the cohort. The pilot study explored an ALI based on a combination of 15 indicators selected from a literature review. Stepwise regression and logistic regression were used to perform the preliminary analysis.
Results:
Stepwise regression models identified five indicators for an ALI based on PSS scores. A positive association was found where the ALI predicted membership in the higher stress group (odds ratio = 1.62; 95% confidence interval: 1.11, 2.37; p = 0.012).
Conclusion:
This pilot study identified a concise set of ALI indicators that may be useful for future stress research and practice. Although preliminary, the identification of an ALI for operationalizing stress may provide a cost-effective and straightforward tool for future research. With further refinement, this measure could offer a method for researchers studying chronic stress, with potential for future clinical application for managing stress-related health outcomes.
Introduction
Research has shown a link between stressors and negative health outcomes or disease risk, with impacts on health occurring directly through physiological responses and also indirectly through changes in health behaviors and social support. 1,2 People living with HIV (PWH) have stressors associated with a fear of HIV on one’s lifespan, a sense of isolation due to HIV stigma, and the preexisting psychosocial burdens prevalent among PWH within marginalized populations (e.g., sexual minorities, individuals who use drugs, those living with low incomes or deficient housing, and those experiencing disparities from racism). 3 –6 Some research has shown that women living with HIV (WWH) experience an increased level of psychosocial stress than men living with HIV and the general population. 7 These stressors may be linked to social and structural issues, including fewer resources needed to care for oneself and others, especially children. 8 Additionally, the stigma associated with HIV can impact relationship stressors and contribute to issues such as higher rates of intimate partner violence among WWH. 9
Physiological stressors are also experienced among PWH, as HIV and antiretroviral medications do not fully restore the immune system. Although HIV can be controlled with antiretroviral medications, chronic inflammation and immune activation persist despite viral suppression. 10 –12 The immune response has been associated with an increase in incidences of serious non-AIDS comorbidities such as coronary artery disease, neurocognitive disorders, metabolic syndrome, chronic liver/kidney dysfunction, and non-HIV-associated cancers. 10 –13
Regardless of the stressor, experiencing chronic stress has been consistently linked to negative health outcomes. 14 –17 The majority of studies examining stress among PWH have used subjective measures of stress, such as the Perceived Stress Scale (PSS). 18 Biomarkers have also been used to determine levels of stress, as they can potentially observe an event through a biological measurement. 19,20 Researchers have utilized a single biomarker, such as heart rate or cortisol level, to measure physiological stress. 16 Because many negative health outcomes are the result of multiple physiological systems working together, focusing on a single biomarker may not provide the predictive value needed. Another method for measuring the stress responses from multiple physiological systems could be to utilize a composite biomarker index that combines multiple biomarkers into a single score. 20
When stressors are introduced, physiological systems respond and adapt to remain in optimal operating ranges. A measure of allostatic load has been designed to summarize the impact that stress has on the body when physiological systems do not adapt and return to normal ranges, leading to wear and tear on the body. 21 Allostatic load was conceptualized by McEwen and Stellar 20 and later operationalized by Seeman et al. 21 to include a 10-variable index within four physiological systems: cardiovascular, metabolic, neuroendocrine, and immunogenic. The neuroendocrine and immunogenic systems serve as the “primary mediators,” which increase in response to ongoing stressors and lead to “secondary outcomes” in the metabolic and cardiovascular systems. 21 –23 Through the expansion of this concept and the inclusion of additional biomarkers, it is difficult to establish a definitive standard for the indicators used when examining an allostatic load index (ALI). Thus, heterogeneous definitions of ALI are displayed throughout the literature. 15,24 –27 Johnson 24 identified 26 studies utilizing an ALI, with 59 identified biomarkers combined in 20 different ways. Mauss 27 reported that 39 individual biomarkers were used to calculate ALI with combinations of indicators that ranged from 6 to 17 within 16 different studies. Additionally, many studies of stress among PWH have utilized single indicators commonly utilized within an ALI, but very few have utilized a composite ALI. 20,26 –28,29 The limited use of a consistent combination of indicators to derive an ALI among PWH, and specifically among WWH, and comparable women without HIV indicates that further exploration of a composite measure through pilot work remains needed in order to identify a set of indicators for an ALI to utilize in future work.
Therefore, the purpose of this pilot study was to (1) explore the ability to identify a set of indicators for inclusion in an ALI related to perceived stress and (2) explore the ability of the calculated ALI to identify an association between the ALI and the PSS score categories in a small sample of WWH and comparable women without HIV from the Women’s Interagency HIV Study (WIHS). We hypothesized that a relationship between the calculated ALI and PSS score categories will be present in this exploration. This would serve as a preliminary exploration of the combined physiological indicators of stress and could potentially be used in place of the commonly used subjective measure (i.e., PSS) in future research work.
Materials and Methods
Participants
This pilot study was a secondary analysis of data and specimens from the WIHS. 30 –33 The WIHS was a multisite prospective longitudinal cohort study within the United States that enrolled WWH and comparable women without HIV to understand the impact of HIV over time. Participants completed interviews and physical examinations every 6 months to obtain demographic, psychosocial, behavioral, anthropometric, laboratory, and clinical data, as well as collection of biological specimens for future research.
The data and specimens for this analysis were collected from the participant’s first WIHS visit between 2014 and 2019. This period was the initial 5 years after the southern sites joined WIHS, thus giving a larger sampling frame from 10 WIHS sites throughout the United States. Within the WIHS repository, participants were categorized into quartiles based on the cohort distribution of PSS scores. Then, all participants within the lowest and highest PSS quartiles with a completed physical examination (including anthropometric and laboratory data) and blood specimens submitted to the WIHS repository, all within 30 days of each other, were eligible for inclusion (n = 444). Based on available funding and the nature of initial exploration through this pilot study, a sample of 206 (n = 103 from the lowest quartile and n = 103 from the highest quartile) participants were selected from the eligible cohort. Participants within the two quartiles were matched 1:1 based on race/ethnicity, age, body mass index (BMI), and HIV serostatus. Study activities were approved by institutional review boards at each participating site, and all participants provided informed consent for data to be utilized.
Perceived Stress Scale
The outcome of interest was the self-reported PSS. 18 The PSS is a widely used measure to determine the perception of stress during the previous month. The PSS has demonstrated good internal consistency and validity across many studies. 34 –36 Each item in the 10-item scale was scored using a 5-point Likert scale, ranging from 1 (never) to 5 (very often), asking participants to identify how often they felt a certain way. An example statement is, “Over the past month, how frequently have you felt nervous and stressed?” The total PSS score is computed by summing all 10 items, with higher scores indicating greater perceived stress (scores range from 0 to 40). Established score categories for the PSS are low stress (0–13), moderate stress (14–26), and high stress (27–40). 18
In this study, based on the sample distribution, participants were in the lowest (n = 103) and highest (n = 103) quartiles of PSS scores to provide a bipolarity of perceived stress scores for the analysis based on having limited funding. The lowest quartile indicated very low perceived stress (scores ranged from 0 to 6), and the highest quartile indicated moderate/high perceived stress (scores ranged from 20 to 37).
Allostatic load indicators
The indicators to derive the ALI were selected based on a literature review of components utilized within ALIs representing four physiological systems (cardiovascular, metabolic, neuroendocrine, and immunological). Fifteen biological and anthropometric indicators were identified and included in the study. There were three cardiovascular indicators (systolic blood pressure [BP], diastolic BP, and heart rate) and five metabolic indicators (waist–hip ratio, triglycerides, high-density lipoprotein [HDL] cholesterol, hemoglobin A1c, and fasting glucose) obtained from participants’ research records. Neuroendocrine indicators (cortisol and dehydroepiandrosterone sulfate [DHEA-s]) and immunological indicators (C-reactive protein [CRP], interleukin-6 [IL-6], tumor necrosis factor-alpha [TNF-α], insulin-like growth factor-1 [IGF-1], and interleukin-1 beta [IL-1β]) were measured using participants’ frozen serum obtained from the repository. All samples were collected based on established protocols from within the WIHS study.
Serum biomarkers were quantified with commercially available enzyme-linked immunosorbent assays according to the manufacturer’s instructions (MP Biomedicals 07M-21602 [cortisol] or 07M-5125A [DHEA-s], Invitrogen KHA0031 [CRP], R&D Systems DG100B [IGF-1], Bio-Plex Multiplex Kit 12007283 [IL-6, IL-1β, TNF-α]). All samples were shipped from the Multicenter AIDS Cohort Study (MACS)/WIHS Combined Cohort Study (MWCCS) biorepository on dry ice and stored in a −80°C freezer until the analysis occurred. Duplicate samples were measured with quality controls on each plate. Measurements that were not bound by the standard curve or had a coefficient of variance greater than 10% were excluded from the analysis.
Consistent with previous studies, the ALI was calculated using the count method. 19 This method is based on the sum of indicators identified to be in the highest risk quartile (<25th percentile for HDL cholesterol and DHEA-s and >75th percentile for all others). Values falling into the highest risk quartile are dichotomized as 1, with all other values assigned 0. The ALI score is then calculated based on the sum of the dichotomous (0/1) indicators. For this study, high-risk cut points for the indicators were based on clinically established high-risk quartiles. 37,38 The clinical cut points used to assign high risk for each indicator are shown in Table 1.
High-Risk Cut Point Values for Each Allostatic Load Indicator
Lower quartile utilized for cut point.
BP, blood pressure; CRP, C-reactive protein; DHEA-s, dehydroepiandrosterone sulfate; HDL, high-density lipoprotein; IGF-1, insulin-like growth factor-1; IL-1β, interleukin-1 beta; IL-6, interleukin-6; TNF-α, tumor necrosis factor-alpha.
Covariates
Age, race/ethnicity, BMI, and HIV serostatus covariates were controlled by matching with the following categories utilized: race/ethnicity (Black/African American, non-Hispanic; White, non-Hispanic; All Hispanic; Other), age (<41, 41 to <61, ≥61), BMI (0 to <18.5 [underweight], 18.5 to <25 [normal], 25 to <30 [overweight], ≥30 [obesity]), and HIV serostatus (positive, negative). Additional demographic variables that served as potential covariates to perceived stress were marital status (married*[legally, common law married, lives with partner], previously married [widowed, divorced, annulled, separated], never married, other) and education (less than high school, completed high school, any higher education*), with the asterisks indicating the reference groups.
Statistical analysis
Demographic and clinical data were explored using summary statistics. Mean and standard deviation (SD) were used for continuous variables, whereas frequency and percentages were used for categorical variables. Exploratory analysis included independent sample t-tests and chi-square tests were used to compare continuous and categorical variables, respectively, by HIV serostatus and PSS groups. A total of 15 allostatic load indicators were explored as potential predictors of the PSS score. A stepwise regression analysis was conducted to explore the combination of indicators to be included in the ALI. The model selection was based on the highest adjusted R-squared value with all coefficients of the included variables being statistically significant (p < 0.05). To evaluate the dichotomous high-risk category of the indicators used to calculate the ALI, frequency and percentage distributions were calculated based on both the sample distribution and clinical high-risk thresholds. A logistic regression analysis was performed to assess the preliminary association between the resulting ALI score and PSS categories with odds ratios (ORs) and 95% confidence intervals (CIs). A receiver operating characteristic (ROC) curve was generated with the area under the curve (AUC) calculated to assess the ability of the calculated ALI to classify moderate/high or low perceived stress grouping. The Statistical Package for Social Sciences (Version 29) was used, with a p-value <0.05 indicating statistical significance.
Results
A total of 206 participants contributed data to the analysis. Characteristics of the sample are presented in Table 2. The mean age of participants was 49 (SD = 7.3) years. Most identified as Black/African American (71%), were living with HIV (74%), and were obese (BMI ≥30 kg/m2) (64%). Participants in the sample were most likely to have never been married (34%) and have less than a 12th-grade education (34%). No significant sociodemographic differences by HIV serostatus or among PSS groups were identified (data not shown).
Sociodemographic Characteristics of Study Population (N = 206)
BMI, body mass index; HIV, human immunodeficiency virus; PSS, Perceived Stress Scale; SD, standard deviation.
Mean levels of the 15 individual allostatic load indicators for the sample and by HIV serostatus are presented in Table 3, with significant differences noted among certain metabolic (waist–hip ratio) and neuroendocrine (cortisol and DHEA-s) indicators. WWH had a higher waist–hip ratio (p = 0.024) and lower levels of cortisol (p = 0.047) and DHEA-s (p = 0.001) when compared with women without HIV. Using stepwise regression, we identified five factors—TNF-α, systolic BP, IL-6, cortisol, and HDL cholesterol—that were significantly associated with PSS score (Table 4). Five total models were identified, and we selected the model that demonstrated the highest adjusted R-squared value (R 2 = 0.110) compared with the other models in predicting PSS.
Means, SDs, and HIV Serostatus Differences on Allostatic Load Indicators and Perceived Stress
p-Value obtained comparing means of women with HIV and women without HIV using t-test.
BP, blood pressure; CRP, C-reactive protein; DHEA-s, dehydroepiandrosterone sulfate; HDL, high-density lipoprotein; IGF-1, insulin-like growth factor-1; IL-1β, interleukin-1 beta; IL-6, interleukin-6; SD, standard deviation; TNF-α, tumor necrosis factor-alpha.
Results of Stepwise Regression Analysis to Identify the Combination of Indicators to Be Included in an Allostatic Load Index
Dependent variable: Perceived Stress Scale.
BP, blood pressure; CI, confidence interval; CRP, C-reactive protein; DHEA-s, dehydroepiandrosterone sulfate; HDL, high-density lipoprotein; IGF-1, insulin-like growth factor-1; IL-1β, interleukin-1 beta; IL-6, interleukin-6; LL, lower limit; SE, standard error; Sig., significant; TNF-α, tumor necrosis factor-alpha; UL, upper limit.
The combination of the five indicators identified by stepwise regression was used to calculate an ALI using dichotomized risk scores in the count method to give a possible score range of 0–5 (see Supplementary Table S1). The mean ALI score was 0.43 (SD = 0.80, range 0–4), with 88% of the participants having a calculated ALI ≤1. There was no difference in ALI score by HIV serostatus (see Table 3; WWH: mean = 0.41, SD = 0.8; women without HIV: mean = 0.47, SD = 0.9).
A logistic regression analysis was performed to explore the association between the five-indicator ALI score and PSS grouping. A positive association between ALI and being in the moderate/high stress group was identified (OR = 1.62; 95% CI: 1.11, 2.37; p = 0.012). The odds of being in the moderate/high PSS group are multiplied by 1.62 for every 1 unit increase in the five-indicator ALI score. Figure 1 shows the results of the ROC evaluating the ability of the model using the ALI score to classify patients into low or moderate/high perceived stress groups. The AUC of 0.594 (p < 0.05) indicates a modest discrimination between participants with moderate/high and low perceived stress levels, suggesting the model is moving in the right direction, but its discriminative ability remains limited.
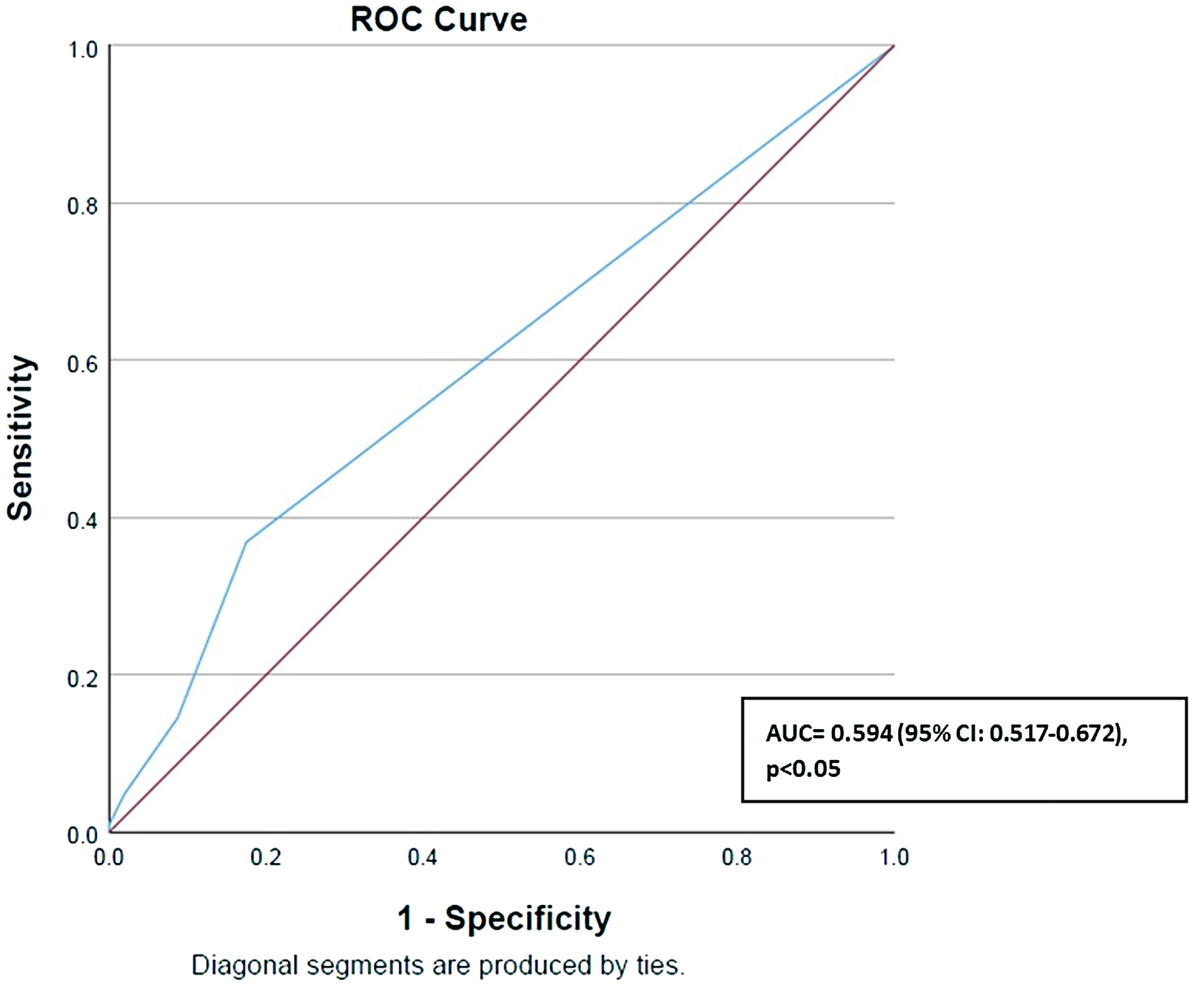
Receiver operating characteristic curve for participants in the moderate/high perceived stress category. AUC, area under the curve.
Discussion
Given the limited research on ALI among PWH and the inconsistent definitions and markers used to define ALI throughout the literature, this study aimed to statistically explore a simplified set of ALI indicators that could be used as an objective measure of stress in future research. First, the number of indicators to be included within a calculated ALI were reduced from 15 to 5, with each of the four physiological domains represented. Next, an initial attempt was made to explore the utility of the minimal set of indicators by examining the relationship between the calculated ALI and perceived stress groups. Despite the small sample size and pilot nature of the study, significant associations were found between the calculated five-indicator ALI and PSS. Given the exploratory nature of this pilot study, these findings are considered preliminary and may inform the design of future research studies.
Allostatic load was originally conceptualized with 10 biomarkers spanning four physiological systems. 21 Since its conception, the number of indicators utilized within an ALI has varied, with the number of indicators ranging from 4 to 25, and more studies utilizing larger combinations of indicators within an ALI. 15,24 –28 However, there is benefit in having a condensed ALI that is effective for use in clinical practice and in future research opportunities. The clinical benefit of a minimal number of indicators measuring ALI is to improve objective and cost-effective markers of chronic stress and, ultimately, an effective manner of predicting negative health outcomes due to chronic stress. The research benefit of having a smaller combination of indicators to operationalize ALI would enhance the cost-effectiveness of the awarded funding, enabling the inclusion of larger sample sizes, which ultimately strengthens the study’s validity.
Mauss 39 also identified a streamlined ALI based on five indicators; however, these represented only two of the four physiological systems. Many additional studies that utilized a lower number of indicators did not include indicators from each of the four physiological systems but rather focused on one primary mediator and one secondary outcome physiological system. 25 Variations in ALI are expected among studies to predict unique tertiary outcomes. However, supporting the initial concept of allostatic load to operationalize the combination of impacts from multiple body systems is important. While our study’s design did not require each of the four physiological systems to be represented within the final model, the results identified a five-indicator ALI that spanned all four physiological systems. Additionally, the five indicators identified in this study have been consistently used in calculating ALI among other studies in combination with additional indicators. 23 –25
Another variation in an ALI calculation identified in the literature is whether the indicators are based on sample distribution or clinical high-risk thresholds. Using sample distribution to calculate the high-risk thresholds can lead to a large amount of variance among studies. 40 Additionally, there are no standard clinical cut points for each biomarker utilized within the allostatic load literature, also potentially leading to variations among studies. 40 There are no clearly defined guidelines in the literature for using the sample distribution or clinical thresholds, highlighting an area for further exploration. In this pilot study, we examined both sample distributions and clinical high-risk thresholds to help inform the analysis. We found that many indicators based on sample distributions were not considered high-risk in the clinical setting (see Supplementary Table S1). As a result, high-risk thresholds for the calculated ALI were based on clinically established high-risk quartiles for the individual indicators.
The focus of this pilot work was to inform future research by exploring whether an objective stress measure could replace the subjective PSS. In examining our findings, we identified a relationship between the subjective psychological measure (i.e., PSS) and the objective physiological measure (i.e., calculated ALI). However, the low AUC suggests more exploration is needed. This aligns with other studies that have found weak or no relationships between psychological and physiological stress measures. 41 Several factors may contribute to the lower AUC, including the small sample size, limited variability in stress levels within the sample, or the exploratory nature of the five-indicator ALI model. Additionally, the difference in reference periods for the study measures may also play a role: the PSS monitors stress within the past month, while the ALI is intended to measure the physiological impact of chronic stress, presumably over a longer period of time. Therefore, further exploration will be needed before using the measures as proxies for one another to evaluate the stress response.
Limitations
This pilot study has some limitations regarding the indicators included within the study. While the indicators included in this data exploration were commonly identified in the literature in relation to ALI, other frequently cited indicators were excluded due to resource constraints. Additionally, certain initial indicators identified in the literature, such as epinephrine and norepinephrine, were excluded from our study. These indicators were originally considered as part of the pilot study, but attempts to measure them proved unreliable. The failure to obtain consistent measurements was likely due to the instability of these biomarkers in stored samples, leading to their removal from the study. An additional indicator limitation was related to the use of cortisol, as it can fluctuate based on the time collected. For this reason, 24-hour urine cortisol is often used to represent the diurnal rhythm. Standard serum cortisol analysis usually occurs on samples collected within a specific time, such as first thing in the morning or in the evening. In this study, serum cortisol was from stored samples in which the time of day was unspecified, which may have impacted the predictive validity of cortisol levels.
Our study aimed to investigate if allostatic load reflected the subjectively measured PSS, and therefore, the identified ALI was calculated based on that outcome. In the sample, it was originally expected that perceived stress levels among WWH and comparable women without HIV would be higher. However, a limitation we identified was that the overall PSS scores and the calculated ALI scores were both particularly low. Having a sample with low-stress scores does not allow these results to be generalized to a higher-stressed population. Additionally, the study did not account for medications the participants may be taking or the presence of chronic health conditions that may have impacted stress levels and individual indicators within the ALI.
Implications for future research
There are important directions for future research on operationalizing and utilizing allostatic load as a measure of chronic stress, building on the findings of this pilot study. First, the results from this study should be replicated with a larger dataset that has greater variability in stress levels to assess whether the calculated ALI can effectively discriminate between mid-range and high-stress scores. Additionally, this study’s initial exploration of ALI indicators relied on the subjective PSS measure, a questionnaire intended to measure generalized current stressors. Expanding this study to include additional measures of chronic stress experienced by women will help explore the combination of indicators within the calculated ALI for future research focused on the long-term impact of stress on women. Further exploration with a larger dataset can also help determine if there are differences in ALI when stratified based on HIV serostatus, enabling a deeper investigation into the impact of HIV on health outcomes. Following the continued validation of the indicators used in operationalizing the ALI, future work to utilize the measure can be conducted to explore the mediating impact that a participant’s ALI has on negative health outcomes.
Conclusion
This study aimed to explore a method to statistically identify a simplified set of ALI indicators that could serve as an objective measure of stress in future research. A minimal set of five indicators that span four physiological systems was found to be associated with the perceived stress levels in a sample of WWH and comparable women without HIV. The ALI, calculated based on risk indices, included systolic BP (cardiovascular), HDL cholesterol (metabolic), cortisol (neuroendocrine), and IL-6 and TNF-α (immunological). Continuing to explore a reduced yet parsimonious ALI could offer a cost-effective and simpler method for researchers studying chronic stress, with the potential for future clinical application. Additionally, standardizing the method for operationalizing allostatic load among researchers would enhance the interpretation of results across studies and improve practice in the management of chronic stress-related health outcomes.
Footnotes
Acknowledgments
The authors would like to acknowledge the National Program of Cancer Registries of the Centers for Disease Control and Prevention for the funds that helped support the collection and availability of the cancer registry data and thank the following state cancer registries for their help: AL, CA, FL, GA, IL, MD, MS, NY, NC, PA, and VA. The authors assume full responsibility for analyses and interpretations of these data.
Authors’ Contributions
Study concept and design were by K.C.H. and D.K.-P. Acquisition, analysis, and interpretation of data were by K.C.H., M.K., L.M.H., W.Y., and D.K.-P. Critical revisions of the article for important intellectual content were performed by K.C.H., M.K., L.M.H., W.Y., I.B., P.L.F., M.LA., M.C.-R., A.C., M.H.C., A.E., A. Sharma, A. Spence, S.D.W., G.W., and D.K.-P. All co-authors listed have reviewed and approved this article before submission.
Data Availability
Author Disclosure Statement
The authors have no disclosures.
Funding Information
The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). MWCCS (Principal Investigators): Atlanta CRS (Ighovwerha Ofotokun, Anandi Sheth, and Gina Wingood), U01-HL146241; Baltimore CRS (Todd Brown and Joseph Margolick), U01-HL146201; Bronx CRS (Kathryn Anastos, David Hanna, and Anjali Sharma), U01-HL146204; Brooklyn CRS (Deborah Gustafson and Tracey Wilson), U01-HL146202; Data Analysis and Coordination Center (Gypsyamber D’Souza, Stephen Gange and Elizabeth Topper), U01-HL146193; Chicago-Cook County CRS (Mardge Cohen, Audrey French, and Ryan Ross), U01-HL146245; Chicago-Northwestern CRS (Steven Wolinsky, Frank Palella, and Valentina Stosor), U01-HL146240; Northern California CRS (Bradley Aouizerat, Jennifer Price, and Phyllis Tien), U01-HL146242; Los Angeles CRS (Roger Detels and Matthew Mimiaga), U01-HL146333; Metropolitan Washington CRS (Seble Kassaye and Daniel Merenstein), U01-HL146205; Miami CRS (Maria Alcaide, Claudia Martinez, and Deborah Jones), U01-HL146203; Pittsburgh CRS (Jeremy Martinson and Charles Rinaldo), U01-HL146208; UAB-MS CRS (Mirjam-Colette Kempf, James B. Brock, Emily Levitan, and Deborah Konkle-Parker), U01-HL146192; UNC CRS (M. Bradley Drummond and Michelle Floris-Moore), U01-HL146194. The MWCCS is funded primarily by the National Heart, Lung, and Blood Institute (NHLBI), with additional co-funding from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD), National Institute on Aging (NIA), National Institute of Dental & Craniofacial Research (NIDCR), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Neurological Disorders and Stroke (NINDS), National Institute of Mental Health (NIMH), National Institute on Drug Abuse (NIDA), National Institute of Nursing Research (NINR), National Cancer Institute (NCI), National Institute on Alcohol Abuse and Alcoholism (NIAAA), National Institute on Deafness and Other Communication Disorders (NIDCD), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute on Minority Health and Health Disparities (NIMHD), and in coordination and alignment with the research priorities of the National Institutes of Health, Office of AIDS Research (OAR). MWCCS data collection is also supported by UL1-TR000004 (UCSF CTSA), UL1-TR003098 (JHU ICTR), UL1-TR001881 (UCLA CTSI), P30-AI-050409 (Atlanta CFAR), P30-AI-073961 (Miami CFAR), P30-AI-050410 (UNC CFAR), P30-AI-027767 (UAB CFAR), P30-AI-124414 (ERC-CFAR), P30-MH-116867 (Miami CHARM), UL1-TR001409 (DC CTSA), KL2-TR001432 (DC CTSA), and TL1-TR001431 (DC CTSA). The authors gratefully acknowledge the contributions of the study participants and the dedication of the staff at the MWCCS sites. This work was supported by the University of Alabama at Birmingham/University of Mississippi Medical Center MWCCS Internal Developmental Pilot Award.
Additionally, Dr. Pariya L. Fazeli is supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 1R01AG077997-01A1 and 1RO1MH131177-01.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.