
Abstract
Objective:
This study examines postpartum health care utilization among women with severe maternal morbidity (SMM) subtypes (e.g., blood transfusion, renal), focusing on both early (within 7 days) and late (8–42 days) postpartum periods. By including outpatient visits alongside inpatient and emergency department (ED) visits, the study offers a comprehensive view of postpartum health care needs among women with SMM.
Methods:
This retrospective cohort study used data from Optum’s de-identified Clinformatics® Data Mart Database from 2008 to 2019. The primary outcomes were early and late postpartum inpatient readmissions, early and late ED visits, and outpatient care within 42 days after delivery. Multilevel logistic regression models were used to estimate the association between SMM subtypes and postpartum readmission, ED, and outpatient care.
Results:
Except for hemorrhage, most SMM subtypes increased the postpartum odds of health care utilization. Women with other medical SMM (e.g., puerperal cerebrovascular disorders or sickle cell disease with crisis) had 2.9 times the odds (odds ratio [OR]: 2.87, 95% confidence interval [CI]: 1.30–6.34) of experiencing early readmissions compared with those without other medical SMM. Women with sepsis had 4.5-fold elevated odds (OR: 4.53, 95% CI: 2.48–8.28) of late readmission, a 1.9-fold increased odds (OR: 1.85, 95% CI: 1.12–3.04) of early ED visits, and over a 2-fold increased odds (OR: 2.27, 95% CI: 1.67–3.08) of postpartum outpatient visits compared with those without sepsis.
Conclusion:
This study reveals that certain SMM subtypes significantly increase postpartum health care utilization, emphasizing the need for further research and interventions to improve outcomes for affected women.
Introduction
Severe maternal morbidity (SMM) refers to life-threatening complications during childbirth that can result in adverse immediate and long-term health consequences. 1 The Center for Disease Control and Prevention (CDC) operationalizes SMM using 21 indicators that include a wide range of conditions (e.g., eclampsia) and procedures performed (e.g., hysterectomy). 2 Women experiencing SMM often present similar characteristics to those who experience maternal mortality, suggesting that SMM exists on a continuum of severity that could potentially end in maternal death. 3
SMM constitutes a traumatic event, impacting not only the health and well-being of affected women but also their families. The postpartum period, also known as the fourth trimester, begins right after childbirth and extends for up to 6 weeks. This critical period is crucial in determining the long-term health trajectories of both the mother and infant. 4 For women with SMM, the postpartum period is fraught with both elevated health risks and challenges in accessing appropriate care. Women with SMM have been reported to experience distressing health care encounters such as discontinuity of care, communication gaps, and perceived neglect of their physical and emotional needs, leading to disappointment in care. 5
These pronounced vulnerabilities in women with SMM are further illuminated when assessing postpartum hospitalization readmission rates, revealing notable differences between women with and without SMM. In the general population, postpartum readmission rates are observed to range from 0.7% to 1.2%. 6,7 In contrast, women with SMM experience an elevated readmission rate spanning from 3.5% to 5.0%. 7,8 It has been found that compared with individuals without SMM at delivery, individuals with SMM have a 57% and 69% increased risk of being readmitted to the hospital within 7 days of delivery and 8 to 42 days postpartum, respectively. 8 Assessing postpartum readmissions within specific time intervals offers a more refined understanding of health care utilization patterns. In general, early readmissions within the first week postdischarge are associated with acute medical conditions, are generally more preventable, and can be managed with hospital-based interventions. 9,10 Conversely, late readmissions may indicate underlying chronic health issues and, while less preventable, may be more amenable to management through ambulatory and home-based care. 9,10
While postpartum readmissions are relatively uncommon for women with and without SMM, postpartum emergency department (ED) visits are more frequent, with approximately 5.8% of women seeking postpartum care in the ED within 42 days of childbirth. 11 A California-based study showed that women with SMM were 58% more likely to visit the ED within 90 days of giving birth compared with women without SMM. 12 Data from New York state revealed a stronger association where women with nontransfusion SMM were 2.6 times as likely to seek ED care within the initial 42 days following childbirth compared with their counterparts without SMM. 11 A more granular exploration is warranted to differentiate early (0–7 days postpartum) versus late (8–42 days postpartum) ED patterns among women with SMM and across specific SMM groups. This distinction is important because it addresses a current knowledge gap and could enhance tailored interventions, benefiting both clinical practice and maternal outcomes.
While the previous points highlight inpatient and ED patterns during the postpartum period, another crucial aspect to consider is outpatient service utilization. Evidence suggests a potential underutilization of postpartum outpatient services, with approximately 40% of women not attending any postpartum visit. 13 Moreover, outpatient postpartum care patterns in women with SMM and among women with various SMM clinical subtypes have not been explored. This gap in research might be due to the use of state and national hospital databases for SMM studies, which usually lack outpatient care information. To address these knowledge gaps, this study leveraged an expansive multiyear administrative claims database of commercially insured women. The primary objective of this investigation was to describe inpatient and outpatient health care utilization patterns (i.e., inpatient, ED, outpatient) across the spectrum of SMM clinical subtypes. 14
Methods
Data sources
This study used a retrospective cohort design leveraging Optum’s de-identified Clinformatics® Data Mart Database (CDM) to evaluate postpartum health care utilization among women with and without SMM, nontransfusion SMM, and by SMM clinical subtypes. CDM is derived from a database of administrative health claims for members of large commercial and Medicare Advantage health plans. CDM utilizes medical and pharmacy claims to derive patient-level enrollment information, health care costs, and resource utilization information. The population is geographically diverse, spanning all 50 states, and is statistically de-identified under the Expert Determination method consistent with HIPAA and managed according to Optum customer data use agreements. CDM administrative claims submitted for payment by providers and pharmacies are verified, adjudicated, and de-identified before inclusion. CDM contains each patient’s 5-digit zip code.
Zip codes were assigned to counties using the Housing and Urban Development crosswalk files. 15 The Area Health Resources File (AHRF) and Agency for Toxic Substances and Disease Registry databases were used to derive county-level covariates of interest, including the social vulnerability index (SVI) 16 and metropolitan status. The AHRF offers comprehensive data spanning health care professions, facilities, population attributes, health care utilization, and environmental factors across county, state, and national levels. 17
Target population
The target population of this study comprised women aged 12 to 55 years with a delivery hospitalization from January 1, 2008 to December 31, 2018. Delivery hospitalizations were identified using the ICD-9/10-CM/PCS and DRG codes shown in Supplementary Appendix SA1. Deliveries associated with diagnostic and procedure codes found in Supplementary Appendix SA2, which include indicators of ectopic and molar pregnancies, or other outcomes resulting in abortion, were not included in the analysis. To ensure a comprehensive assessment of prenatal comorbidities before delivery and to track postdelivery health care utilization, continuous enrollment for 365 days both before and following the delivery event was required. Figure 1 illustrates the inclusion/exclusion criteria alongside the corresponding sample sizes.
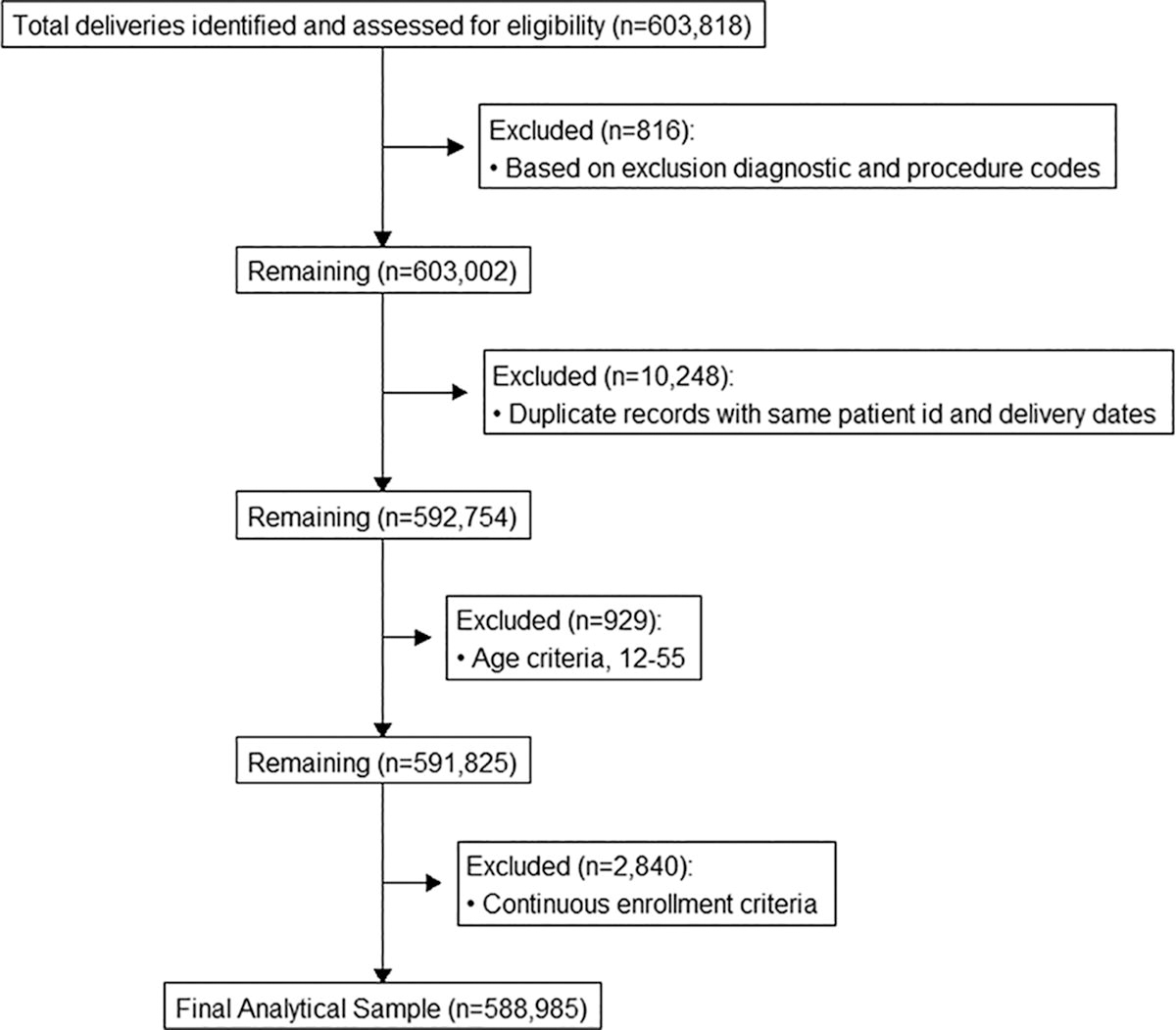
Diagram illustrating development of analytical sample.
Outcomes of interest
The outcomes of interest included all-cause postpartum readmission, ED, and outpatient visits that occurred 42 days (i.e., 6 weeks) from the discharge date of the delivery hospitalization. Postpartum readmissions and ED visits were divided into early (≤7 days) and late (8–42 days) categories, aligning with established classifications in obstetric literature. 18 Binary early and late indicators were developed for inpatient readmissions and ED visits. Specifically, the presence of a singular readmission event during the early postpartum period was indicative of a positive classification for early readmission in the dataset. This logic also applied to late readmissions and ED visits. ED visits were identified using the following: (a) CPT/HCPCS codes: 99281, 99282, 99283, 99284, 99285, 99291; (b) revenue codes: 0450, 0451, 0452, 0456, 0459, 0981; and (c) place of service code: 23. Postpartum outpatient visits were captured using a combination of provider category, CPT/HCPCS, and ICD-9/10-CM codes listed in Supplementary Appendix SA3. Starting in 2018, the American College of Obstetricians and Gynecologists adjusted their postpartum care guidelines, advising women to seek care within the first 3 weeks after childbirth, followed by another visit by the 12th week. 13 Before this revision, the guidance suggested a minimum of one visit within the 6-week period following delivery. Given that most deliveries in this study occurred before the 2018 revision, a binary indicator (yes/no) was created to indicate whether a woman had a postpartum outpatient visit within 42 days following delivery.
Primary exposure of interest
The primary exposure of interest was SMM during the delivery hospitalization. SMM was identified using the CDC’s ICD-9/10-CM/PCS system (Supplementary Appendix SA4). Given the rarity of many of the 21 SMM subtypes, which made subtype-specific evaluations challenging, we aggregated individual indicators into nine clinical categories based on the AIM rubric (Supplementary Appendix SA4). 14 The nine AIM SMM subtypes include the following: cardiac, hemorrhage, other medical, other obstetric, pulmonary, renal, respiratory, sepsis, and transfusion. In addition, a separate category called nontransfusion SMM was created, excluding women whose only SMM was a blood transfusion during the delivery hospitalization. Blood transfusions are frequently excluded from the criteria for SMM because they may not accurately represent instances of SMM in the absence of other indicators. 19,20
Covariates
Maternal age was grouped as 12–19, 20–29, 30–34, 35–39, and 40–55. Prenatal care was measured using the adequacy of prenatal care utilization (APNCU) index using four categories as follows: inadequate, intermediate, adequate, and adequate plus. 21,22 The APNCU is based on two primary components as follows: the timing of the initiation of prenatal care and the number of prenatal visits adjusted for the gestational age (GA) at delivery. To construct the APNCU index, it was necessary to estimate GA, as the CDM does not include information regarding the infant’s GA. Therefore, GA had to be estimated using ICD-9/10-CM codes listed on the maternal record. For the ICD-9-CM era, due to the lack of specific gestational week codes, we utilized the classification system developed by Li et al. (Supplementary Appendix SA5) to infer GA. Conversely, in the ICD-10-CM period, the introduction of Z3A** series allowed for a week-by-week classification. For example, a Z3A36 code indicates a gestational age of 36 weeks, whereas Z3A38 signifies 38 weeks (Supplementary Appendix SA5). High validity has been established for the Z3A** codes that specify gestational age at delivery. 23
Type of delivery (cesarean vs. vaginal) was captured using DRG codes 765 and 766, ICD-9-PCS code 74**, and ICD-10-PCS codes 10D00Z0, 10D00Z1, and 10D00Z2. An obstetric comorbidity (OCI) score developed by Leonard et al. (Supplementary Appendix SA6) 24 was used to capture maternal comorbidities documented up to 365 days before delivery, as well as those recorded during the delivery hospitalization. Studies have shown that relying solely on comorbidities reported during the delivery hospitalization can fail to identify certain conditions, including chronic diseases like chronic renal disease, with an underreporting rate of up to 35%. 25 By assessing comorbidities both before and during delivery, this approach aimed to ensure a comprehensive evaluation of maternal comorbidity burden. The comorbidities were summed, and respective weights were applied. The “score for SMM” weighting system was used for any SMM and the nine SMM subtypes (cardiac, renal, etc.). The “score for non-transfusion SMM” weighting system was used for the analysis of nontransfusion SMM cases. For capturing county-level social determinants of health, the SVI was used, which encompasses the following four domains: (1) socioeconomic status (SES), (2) household characteristics, (3) racial and ethnic minority status, and (4) housing type and transportation. 16 Health professional shortage areas primary care physicians (HPSA PCP) at the county level were grouped into three categories as follows: none, partial, and whole. In addition, based on urban–rural classification, counties were designated as either metropolitan or nonmetropolitan.
Statistical analysis
Counts and proportions were calculated to assess the distribution of categorical variables within the overall study sample, as well as for other specific outcomes such as early and late readmissions, ED visits, and outpatient visits. Similarly, means and standard deviations (SDs) were calculated for continuous variables. Rates per 1,000 deliveries and 95% confidence interval (CI) for any SMM, nontransfusion SMM, and each of the nine AIM SMM subtypes were calculated across each of the study outcomes. Data cells with counts fewer than 5 were suppressed to adhere to Optum data privacy standards.
The “performance” package in R
26
was used to assess multicollinearity among the independent variables. Multilevel logistic regression models were used to obtain adjusted odds ratios (ORs) and 95% CIs for the associations between SMM subtypes and each outcome (i.e., early and late readmissions and ED). The selection of covariates for model inclusion was informed by directed acyclic graphs and a review of the literature. We first assessed the association between any SMM versus non-SMM and the five outcomes while adjusting for covariates, including age, delivery type, APNCU index, prenatal OCI, SVI themes, metropolitan area, and HPSA PCP. The analyses were repeated for the nontransfusion SMM group versus no SMM and the SMM subtypes. The below bullet points illustrate the different models assessed for early readmissions. Early inpatient admission (outcome) = Any SMM (reference = no SMM) + covariates Early inpatient admission (outcome) = Nontransfusion SMM (reference = no SMM) + covariates Early inpatient admission (outcome) = Cardiac (reference = no cardiac SMM) + Hemorrhage (reference = no hemorrhage SMM)+ .... + last SMM subtype (reference = X) + covariates
To account for repeated deliveries by the same woman over the 10-year study duration, all 15 models were implemented as multilevel logistic regression analyses. Data management (joining tables using PROC SQL and recoding variables) was performed in SAS version 9.4 (SAS Institute, Inc., Cary, North Carolina), and data analysis and graphics were performed in R version 4.3.1 (Comprehensive R Archive Network, https://cran.r‐project.org/). To run the multilevel logistic regression models, the lme4 package was used. 27 This study was approved by the University of Texas Health Science Center School of Public Health Institutional Review Board.
Results
The characteristics of the study population are presented in Table 1. In the overall study sample, the most common age group was 30 to 34 years (38.3% of deliveries). In addition, 65.0% underwent vaginal deliveries, 32.7% received ‘adequate plus’ prenatal care (32.7%), 60.1% lived in counties with partial shortages of primary care physicians (HPSA PCP), and the majority resided in metropolitan areas (92.8%). Approximately, 1.3% (n = 7,502) of women in the sample had at least one SMM at delivery. The mean prenatal OCI score in the overall study population was 6 (SD = 7.9). The mean prenatal OCI scores were higher for individuals who experienced early (mean = 10.8, SD = 11.1) and late readmission (10.4, SD = 11.0) than for the overall study population and for other outcomes (i.e., early and late ED, outpatient). For SES, the SVI scores were slightly higher among those with early (mean: 0.39, SD: 0.24) and late readmission (mean: 0.40, SD: 0.24) compared with the overall sample and other outcomes (i.e., early and late ED, outpatient).
Demographic and Clinical Characteristics of Commercially Insured Women
Overall and by Earlya (0–7), Lateb (8–42), postpartum inpatient readmissions, emergency department visits, and outpatient visits, 2008–2019.
Early refers to events within 7 days postdelivery discharge.
Late refers to the period from 8 to 42 days postdelivery discharge.
Outpatient visits are those that took place within the 42 days following delivery discharge in an outpatient setting.
The prenatal obstetric comorbidity score captured all comorbidities present (both inpatient and outpatient) one year before the delivery date, as well as those documented during the delivery hospitalization.
Health professional shortage areas (HPSA) in primary care are calculated based on the number of health professionals available in a geographical area relative to the population that needs services.
Data suppressed due to cell counts less than 5.
IP, inpatient; ED, emergency department; APNCU, adequacy of prenatal care utilization; OCI, obstetric comorbidity; SMM, severe maternal morbidity; SD, standard deviation; SVI, Social Vulnerability Index.
In the overall study population, early and late postpartum admissions occurred at a rate of 6.6 per 1,000 (95% CI: 6.4–6.8) and 5.8 per 1,000 (95% CI: 5.6–6.0), respectively (Table 2). Early visits to the ED occurred at a rate of 29.1 per 1,000 (95% CI: 28.7–29.5), with the rate for late ED visits at 47.2 per 1,000 (95% CI: 46.7–47.7). The postpartum outpatient rate in the sample was 478 per 1,000 (95% CI: 476.8–479.3). Compared with the rate in the overall population, postpartum health care utilization was higher among women with any SMM and women with any of the SMM subtypes.
Rates a of Inpatient Postpartum Readmission, Emergency Department Visits, and Outpatient Care per 1,000 Deliveries by Severe Maternal Morbidity Subtypes, 2008–2019
Visits represent binary indicators (i.e., at least one IP/ED/OP visit).
Early refers to events within 7 days postdelivery discharge.
Late refers to the period from 8 to 42 days postdelivery discharge.
Outpatient visits are those that took place within the 42 days following delivery discharge in an outpatient setting.
IP, inpatient; ED, emergency department; SMM, severe maternal morbidity; 95% CI, 95% confidence interval.
Supplementary Appendix SA7 presents the results of postpartum health care utilization rates across individual and county-level factors. Women in the highest SES SVI quartiles generally experienced higher rates of health care utilization for outcomes such as early and late inpatient and ED visits. However, an exception was observed regarding outpatient visits where the lowest SES quartile (Q1) showed higher rates of outpatient visits at 498.6 per 1,000 (95% CI: 496.1–501.2) compared with the highest quartile (Q4) at 469.9 per 1,000 (95% CI: 467.3–472.5). As quartiles of racial and ethnic minority status SVI increased so did rates of late inpatient readmission. Conversely, postpartum outpatient visits revealed the opposite trend for racial and ethnic minority status SVI where the lowest quartile (Q1) had an outpatient rate of 493.3 per 1,000 and the highest quartile (Q4) had an outpatient rate of 454.2 per 1,000. With the exception of early inpatient readmissions, women residing in nonmetropolitan areas had higher rates of postpartum health care utilization compared with women residing in metropolitan areas.
Results of the multilevel adjusted logistic regression models are displayed in Table 3. Compared with deliveries without SMM, the presence of any SMM was consistently associated with increased odds of both early (OR: 1.53, 95% CI: 1.29–1.82) and late postpartum (OR: 2.02, 95% CI: 1.71–2.40) admissions, early (OR: 1.32, 95% CI: 1.19–1.46) and late (OR: 1.28, 95% CI: 1.18–1.40) ED visits, and outpatient care (OR: 1.34, 95% CI: 1.28–1.41). Except for hemorrhage, it was found that most SMM subtypes were associated with an increased odds of postpartum health care events. Notably, both other medical SMM (OR: 4.08, 95% CI: 2.01–8.29) and sepsis (OR: 4.53, 95% CI: 2.48–8.28) were associated with more than a fourfold increase in the odds of late inpatient readmissions.
Multilevel Logistic Regression Models Obtaining Adjusted Odds Ratios and 95% Confidence Intervals Investigating the Association Between Severe Maternal Morbidity Subtypes and Postpartum Health Care Utilization, 2008–2019
Early meaning within 7 days from delivery discharge date.
Late meaning between 8 and 42 days from delivery discharge date.
Outpatient visits are those that took place within the 42 days following delivery discharge in an outpatient setting.
Any SMM explored as the main exposure with outcomes (5 different models) adjusted for age, type of delivery, APNCU Index, prenatal obstetric comorbidities, SVI SES, SVI Household characteristics, SVI Racial/Ethnic Minority Status, SVI Housing type and transportation, SVI, metropolitan area, HPSA PCP.
Nontransfusion SMM explored as the main exposure with outcomes (5 different models) adjusted for age, type of delivery, APNCU Index, prenatal obstetric comorbidities (nontransfusion weighting system), SVI SES, SVI Household characteristics, SVI Racial/Ethnic Minority Status, SVI Housing type and transportation, SVI, metropolitan area, HPSA PCP.
Each of the SMM subtypes included in the 5 models adjusted for age, type of delivery, APNCU Index, prenatal obstetric comorbidities, SVI SES, SVI Household characteristics, SVI Racial/Ethnic Minority Status, SVI Housing type and transportation, SVI, metropolitan area, HPSA PCP.
IP, inpatient; ED, emergency department; SMM, severe maternal morbidity; 95% CI, 95% confidence interval; OR, odds ratio.
Discussion
The overall early and late readmission rates observed in this study were 0.66% and 0.58%, respectively, aligning with previously reported postpartum readmission rates in the literature, which vary between 0.5% and 2.0%. 6 –8,28,29 In this study, the rate for late postpartum ED visits (4.7%) aligns with the previously documented range of 4.4% to 5.8% for ED visits within 42 days. 11,30 Less than half of the study sample (47.8%) had a postpartum outpatient visit within 42 days of delivery. These findings are consistent with a five-year retrospective cohort study by Bennett et al, which investigated predictors of postdelivery primary care among women with commercial insurance and Medicaid. Their study found that although women with pregnancy complications are more likely to attend a postpartum outpatient visit, postpartum outpatient rates in the overall population were low. 31 Specifically, their study identified a postpartum outpatient rate of 49.5% for women with commercial insurance and 45.8% for those covered by Medicaid. 31 The postpartum visit is crucial to support a new mother’s overall health by addressing her physical, mental, and emotional well-being. In addition, it plays an important role in preventing future health complications, promoting optimal recovery, and ensuring long-term wellness. 32 Despite the importance of postpartum visits, many women do not attend these visits for a variety of reasons, such as “feeling well,” time constraints, cultural beliefs, lack of social support, long appointment wait times, and transportation issues. 32 –34 To increase attendance at postpartum visits, it is essential to emphasize the importance of postpartum care during prenatal appointments. Engaging a broader care team, including counselors, postpartum nurses, and discharge planners, can help provide patients with support and guidance to receiving follow-up care. 35 One initiative, the “I Gave Birth” bracelet program, provides new mothers with bracelets to help educate them, their families, and medical professionals on the importance of postpartum care and recognizing warning signs. This program has led to a 0.77% reduction in obstetrical-related readmissions and improved timely care-seeking behavior among patients. 36 By raising awareness, this initiative demonstrates a promising approach to improve postpartum visits. However, improving postpartum care visits requires more than individual-level changes. It demands broader systemic efforts at the societal and environmental levels that include expanding insurance coverage, reducing logistical challenges, and enhancing coordination between health care providers and patients to streamline postpartum visit scheduling.
We found that women living in counties with higher socioeconomic vulnerability had increased rates of all postpartum outcomes except for outpatient care. Research indicates that women living in low SES neighborhoods have higher rates of adverse pregnancy outcomes such as preterm birth, 37 small for gestational age, 37 severe maternal morbidity, and maternal mortality, 38 which may lead to higher rates of postpartum readmissions and ED visits. Limited access to primary care services in low-income neighborhoods further exacerbates these issues as lower income neighborhoods are less likely to have access to high-quality health care. 39 Notably, the variation in how community-level factors such as zip code, county, and neighborhood characteristics are defined and measured can make comparisons across studies challenging. Therefore, further research investigating how community level factors are associated with postpartum outcomes is warranted.
In this study, it was found that SMM is an independent risk factor for readmissions, ED visits, and outpatient visits, highlighting the need for specialized medical attention in the postpartum period. The heightened need for health care services in patients with SMM is driven by a higher incidence of complications, such as hemorrhage, retained placenta, and complications from procedures, 7 requiring specialized advanced care. Addressing postpartum SMM outcomes requires a multidisciplinary approach to enhance patient outcomes and reduce risks, underscoring the need for additional research.
This study also identified differences across SMM subtypes in postpartum health care utilization rates and risk of health care utilization, with notable variations in the risk of readmissions and ED visits among distinct SMM subtypes. Individuals with sepsis faced increased risks for late readmissions, early and late ED visits, and outpatient care. Specifically, women with sepsis were 4.5 times more likely to have a late postpartum readmission than those without sepsis. These results are similar to those from Girsen et al., who reported that women with sepsis had a 4.6- and 4.9-fold greater risk of early and late readmission, respectively. 6 The increased postpartum health care utilization among women with sepsis may stem from maternal sepsis episodes that continue to manifest in the postpartum period. 40 –42
In this study, it was also found that women with Other Medical SMM face an increased risk for both early and late readmissions, with a marked increase during the later period. A contributor to this observation might be sickle cell disease (SCD) with crisis, which is encompassed in the Other Medical SMM category. Prior studies have documented elevated postpartum readmission rates among women with SCD, particularly in the later postpartum period. 8,43 A study by Bae et al. revealed that in comparison with women without SCD, women with SCD faced a 50% elevated risk of postpartum complications, including deep venous thrombosis, sepsis, urinary tract infections, cardiac arrest, and stroke. 43
Limitations/strengths
The results of this study should be interpreted considering several limitations. The CDC’s SMM classification is reliant on diagnostic and procedure codes that might introduce potential misclassification bias in identifying true SMM cases. This is particularly relevant for blood transfusion cases where it is difficult to distinguish between minor and severe cases of blood loss due to the lack of information such as the number of units transfused. To address this, we conducted additional analyses focusing on nontransfusion SMM and observed similar trends in health care utilization in the any SMM and nontransfusion SMM groups. Another limitation of this study is the lack of individual-level race and ethnicity data, which hinders our ability to conduct an in-depth investigation into disparities in postpartum outcomes. Given the well-established literature highlighting significant racial and ethnic disparities in maternal health, particularly in postpartum care, this omission limits our capacity to explore how such disparities might influence the outcomes observed in our study. Furthermore, the community factors examined were limited to county-level data, which may not precisely reflect individual readmission, ED, or outpatient visit behaviors. The study period spans during the ICD-9-CM to ICD-10-CM transition period, which may influence SMM estimates. However, the majority of the study period takes place during the ICD-9-CM period. While some studies reported a decrease in SMM incidence after the implementation of ICD-10-CM, 44 others noted an increase in SMM rates, although not directly associated to the ICD coding change. 45 Therefore, the transition period is unlikely to affect the core findings of the study regarding SMM and postpartum outcomes. This study includes patients with commercial insurance, and while the results are generalizable to the commercially insured population, they do not account for those covered by Medicaid or without any insurance, thus limiting the broader applicability of our findings. Moreover, the study population consists of patients with continuous enrollment both before and after delivery, which further limits the generalizability to a broader population without stable private insurance coverage. We encourage future research to replicate this analysis in Medicaid and uninsured populations to further explore potential disparities in SMM postpartum health care utilization outcomes.
Despite the limitations, this study offers notable strengths. The longitudinal nature of the study facilitates a detailed exploration of patient history both before and following delivery, ensuring the capture of prenatal comorbidities, and tracking subsequent health care interactions in the postpartum period. Spanning several years, the research also manages to identify and include rare SMM subtypes often not included in postpartum health care utilization studies. Notably, the study fills an existing knowledge gap by detailing patterns of SMM subtypes in relation to both early and late ED visits and outpatient care, areas previously under-researched.
Conclusion
This study demonstrates that SMM is an independent predictor of postpartum inpatient readmissions, ED visits, and outpatient care. In addition, the research underscores differences in postpartum health care utilization across the various SMM subtypes. To enhance postpartum care, it is vital to understand the differential impacts of individual SMM subtypes and their implications for tailored interventions. Harnessing this understanding contributes valuable knowledge that may inform and refine clinical guidelines, ultimately aiming to enhance postpartum care for mothers and their families.
Footnotes
Authors’ Contributions
J.L.M.: Conceptualization, methodology, software, formal analysis, and writing—original draft. C.G.C.: Writing—reviewing and editing. L.E.M.: Writing—reviewing and editing. C.X.B.: Writing—reviewing and editing. J.L.S: Writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4
Supplementary Appendix SA5
Supplementary Appendix SA6
Supplementary Appendix SA7
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.