
Abstract
Background:
The opioid overdose crisis remains a public health concern, and rates of suicide with opioid involvement have increased.
Objective:
To describe the prevalence of and factors associated with self-reported past 30-day suicide attempt or attempt “only when high or in withdrawal from alcohol or drugs” among reproductive-age women with past 30-day nonmedical prescription opioid use.
Methods:
Estimates are reported among women 18–55 years from 338 locations in 35 states using 2018–2020 National Addictions Vigilance Intervention and Prevention Program data. Bivariate analysis and multinomial logistic regression identified prevalence of and factors associated with past 30-day suicide attempt and attempt “only when high or in withdrawal from alcohol or drugs.”
Results:
Among 10,095 women, 2.7% reported a past 30-day suicide attempt, and 1.5% reported an attempt “only when high or in withdrawal from alcohol or drugs.” The largest magnitude of association for suicide attempt was extreme alcohol problem (adjusted odds ratio [aOR] = 2.84, 95% confidence interval [CI]: 1.80–4.47), and the largest magnitude of association for attempt “only when high or in withdrawal from alcohol or drugs” was no stable living arrangement (aOR = 2.66, 95% CI: 1.78–3.98).
Conclusion:
Comprehensive, upstream suicide prevention initiatives and substance use treatment can address factors associated with suicide attempt among reproductive-age women.
Introduction
Deaths by suicide occur in response to multiple biological, psychological, interpersonal, environmental, and societal influences that interact with one another, often over time. 1,2 A 2022 Centers for Disease Control and Prevention (CDC) report indicates that rates of suicide among females aged 10–14 years more than tripled from 0.6 per 100,000 in 2000 to 2.0 per 100,000 in 2020, and from 2007 to 2020, rates among females aged 15–24 years increased 87% (3.1 per 100,000 in 2007 to 5.8 per 100,000 in 2020). 3 Data from 36 states’ maternal mortality review committees indicate that mental health conditions, defined as deaths by suicide, overdose/poisoning related to substance use disorder, and other deaths related to a mental health condition, including substance use disorder, are a leading underlying cause of pregnancy-related mortality in the United States. 4
The rate of opioid-involved mortality continues to be a national crisis, with suicide death rates with opioid involvement for women more than doubling between 1999 and 2014 (0.3 per 100,000 to 0.7 per 100,000). 5 According to a 2020 report, approximately 7% of women reported prescription opioid use during pregnancy, and of those, one in five reported misuse, defined as taking too much, using someone else’s prescription, taking it in a different way than prescribed, or using it to get high. 6 Misusing prescription opioids for reasons other than pain 7,8 and use of opioid medication for psychiatric conditions other than anxiety 8 are associated with suicide attempts. A 2017 study using national survey data showed that after controlling for other health and psychiatric conditions, people who misused prescription opioids had 40–60% increased odds of suicidal ideation. 9
Data on self-reported nonmedical prescription opioid use and self-reported suicide attempt among reproductive-age women are limited. Using real-world epidemiological data collected during first intake assessment for substance use treatment from the National Addictions Vigilance Intervention and Prevention Program (NAVIPPRO®), we sought to describe among women aged 18–55 years with self-reported past 30-day nonmedical prescription opioid use: (1) the prevalence of past 30-day self-reported suicide attempt and of past 30-day self-reported suicide attempt “only when high or in withdrawal from alcohol or drugs” and (2) the prevalence of and sociodemographic, social, medical, and legal circumstances and conditions associated with self-reported past 30-day suicide attempt and self-reported past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs.”
Methods
Data for this analysis come from the Addiction Severity Index–Multimedia Version (ASI-MV), an instrument from the NAVIPPRO® (Integrated Behavioral Health, Inflexxion, Irvine, CA). 10 The ASI-MV is a validated, self-administered, computerized, structured clinical assessment tool that collects data from individuals being assessed for substance use treatment. This web-based assessment is based on the Addiction Severity Index, a standard clinical assessment designed for use on admission to drug and alcohol treatment with established reliability and validity, and is used primarily for clinical treatment planning and triage around substance use and associated life-functioning areas. 11,12
This analysis includes data from 338 substance abuse treatment center locations in 35 states a collected January 2018 through December 2020. Locations can use the ASI-MV at intake, discharge, or follow-up, which allows for repeat assessments of the same individual. This analysis only includes data from first intake assessments during the study period.
Similar to a previous analysis of this data, the group of interest was reproductive-age women (18–55 years) with past 30-day nonmedical use of prescription opioids. 13 Using variables in the ASI-MV, “use as prescribed” was defined as (1) having a current pain problem and taking a prescribed opioid medication for pain in the past 30 days; (2) obtaining the medication only from one’s own prescription; and (3) no use of the medication via an alternate route of administration (e.g., injection of a medication prescribed for oral use). 10 Past 30-day nonmedical use of prescription opioids was assigned if a respondent indicated any “use not as prescribed” or if a respondent indicated having used the prescription opioid medication “not in a way prescribed by your doctor, that is, for the way it makes you feel and not for pain relief” in the past 30 days.
The outcome was past 30-day suicide attempt, defined using the question, “In the past 30 days, have you attempted suicide or tried to kill yourself?” Respondents could report one of three mutually exclusive categories: (1) no suicide attempt; (2) a suicide attempt; or (3) a suicide attempt “only when high or in withdrawal from alcohol or drugs.” Women with missing data for this variable were excluded (n = 84).
Variables to assess an individual’s sociodemographic, social, medical, and legal circumstances and conditions included age; health insurance; race and ethnicity; educational attainment; U.S. Census Bureau region b of treatment site; marital status; current living situation; living with anyone with an alcohol problem, who uses nonprescribed drugs or who misuses prescription drugs; days worked for pay in the last 30 days; take home pay in the past 30 days; on probation or parole; history of emotional, physical, or sexual abuse; how bothered by family problems in the past 30 days; how bothered by people other than family in past 30 days; and alcohol severity rating. 11,14 Responses to ASI-MV questions regarding frequency and history of use, problems related to alcohol use, and interest in receiving treatment were used to calculate an alcohol severity score, which ranges from 0 to 9. Scores are categorized as the following: 0–1, no real problem; 2–3, slight problem; 4–5, moderate problem; 6–7, considerable problem; or 8–9, extreme problem. The score cannot be calculated if certain questions are not answered and are categorized as “not calculated.” Reporting of a suicide plan was assessed using the question, “In the past 30 days, have you seriously considered a plan for killing yourself?” Respondents could report one of three mutually exclusive categories: (1) no; (2) yes; or (3) “only when high or in withdrawal from alcohol or drugs.”
Medical conditions assessed included self-reported diagnosis of any of the following in their lifetime: depression or anxiety; manic depression or bipolar; phobia; panic disorder; obsessive-compulsive disorder; eating disorder; posttraumatic stress disorder; multiple personality disorder; personality disorder; psychotic or thought disorder; schizophrenia or paranoid delusional disorder; or dissociative disorder. Additional self-reported conditions and health care-related variables include: receipt of pension or money for a psychiatric disability; number of emergency department visits in the past 30 days; number of lifetime overdoses where needed someone else’s help to recover; pregnancy status; ongoing physical or medical problem that limits or interferes with daily activities; pain problem; and how bothered by physical or medical problems in past 30 days.
We examined each characteristic overall and stratified by past 30-day suicide attempt variable categories. We used multinomial logistic regression to calculate the crude and adjusted odds of past 30-day suicide attempt for each characteristic. Multinomial logistic regression allows for the examination of all three suicide attempt variable categories in one model. Characteristics were selected for model inclusion based on results from bivariate analysis, collinearity assessment, literature review, and expert clinical input. When possible, we selected variables for the adjusted model that used the same time frame as our outcomes of interest (i.e., past 30 days). For example, the variables “pain problem” and “how bothered by physical or medical problems in the past 30 days” were collinear, so the latter variable was selected for model inclusion. The frequency of missing data is reported in tables and not included in statistical comparisons or models. The final adjusted model included age; race and ethnicity; educational attainment; marital status; current living situation; living with anyone with an alcohol problem, who uses nonprescribed drugs, or who misuses prescription drugs; take home pay in the past 30 days; on probation or parole; history of emotional, physical, or sexual abuse; how bothered by family problems in the past 30 days; alcohol severity rating; depression or anxiety diagnosis; manic depression or bipolar diagnosis; posttraumatic stress disorder diagnosis; number of lifetime overdoses where needed someone else’s help to recover; and how bothered by physical or medical problems in past 30 days. SAS Version 9.4 (SAS Institute Inc., Cary, NC) was used for all data management and analyses. Statistical significance was assessed at p < 0.05. This analysis used deidentified data; therefore, it was not considered human subjects research and did not require institutional review board approval.
Results
This analysis included 10,095 women aged 18–55 years with self-reported past 30-day nonmedical prescription opioid use who were being assessed for substance use treatment. Overall, 95.8% (n = 9,675) self-reported no past 30-day suicide attempt, 2.7% (n = 271) self-reported a past 30-day suicide attempt, and 1.5% (n = 149) self-reported a past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs” (Fig. 1).
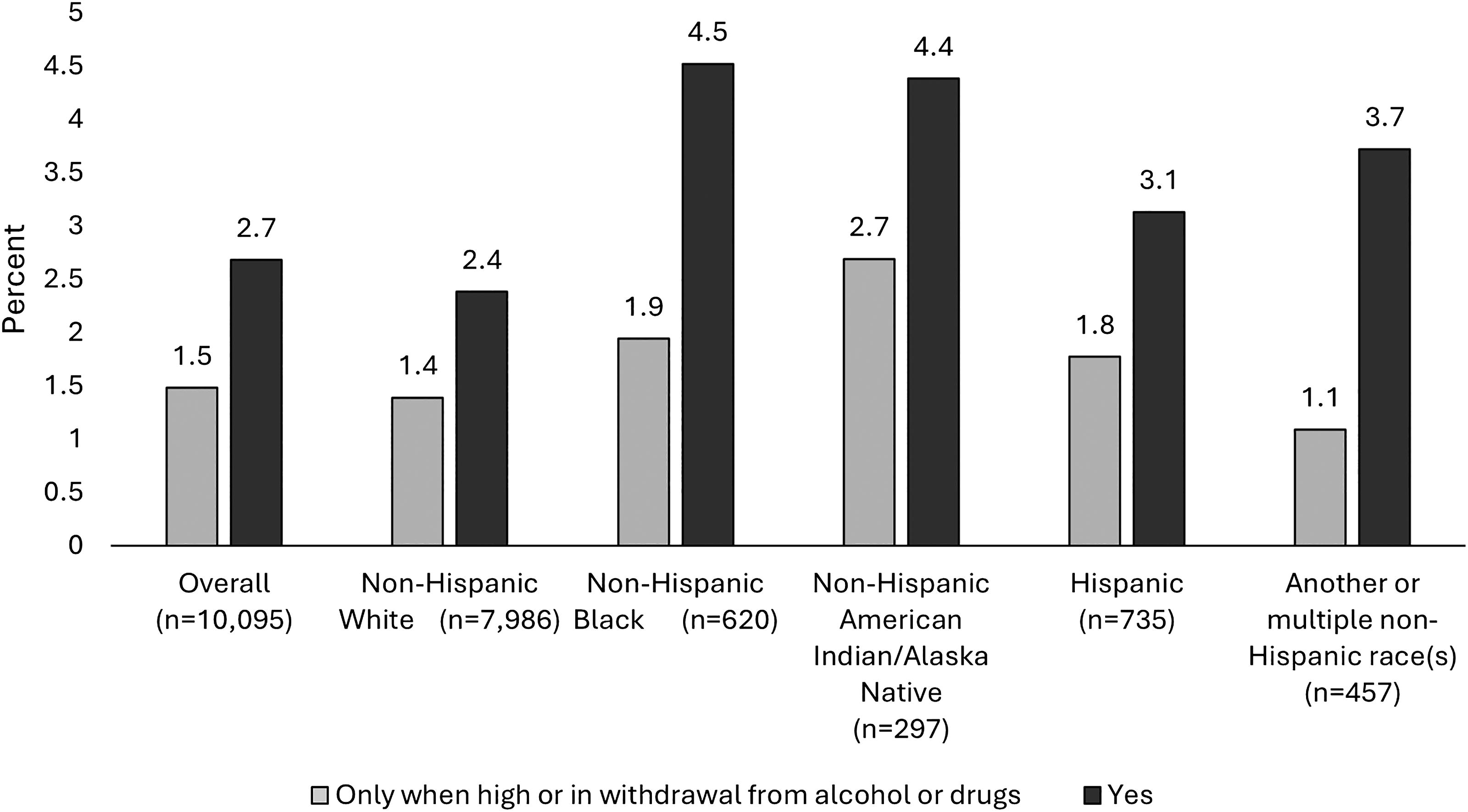
Percent of reproductive-age women with past 30-day nonmedical prescription opioid use with past 30-day suicide attempt, overall, and by race and ethnicity, National Addictions Vigilance Intervention and Prevention Program 2018–2020.
Most women in the analysis were 25–44 years of age and self-identified as non-Hispanic White (Table 1). More than 40% had publicly funded insurance (i.e., Medicaid/Medicare), and more than 40% had received a high school diploma or equivalent. More than three-quarters of the women were single, two-thirds lived in a private home or apartment, and nearly two-thirds of women did not work for pay in the previous 30 days. Nearly one-third were on probation or parole. More than 80% reported a history of emotional, physical, or sexual abuse. Among women who self-reported a past 30-day suicide attempt, 19.5% self-reported having a suicide plan in the past 30 days, and 65.8% self-reported having a suicide plan in the past 30 days “only when high or in withdrawal from alcohol or drugs.” Among women who reported a past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs,” 73.1% reported having a suicide plan in the past 30 days, and 6.3% reported having a suicide plan in the past 30 days “only when high or in withdrawal from alcohol or drugs.”
Past 30-Day Suicide Attempt Among Women of Reproductive Age with Past 30-Day Nonmedical Prescription Opioid Use, by Sociodemographic Characteristics, Social, and Legal Circumstances, National Addictions Vigilance Intervention and Prevention Program 2018–2020
Data were obtained from responses to the NAVIPPRO® Addiction Severity Index–Multimedia Version (ASI-MV) tool during first intake assessment for substance use at 338 program locations in 35 states. Nonmedical prescription opioid use is any use that is not considered “use as prescribed.” “Use as prescribed” was defined as: (1) having a current pain problem and taking a prescribed opioid medication for pain in the past 30 days; (2) obtaining the medication only from one’s own prescription; and (3) no use of the medication via an alternate route of administration. Nonmedical use was also assigned if a respondent indicated having used the prescription opioid medication “not in a way prescribed by your doctor, that is, for the way it makes you feel and not for pain relief.”
aPast 30-day suicide attempt was defined using the question, “In the past 30 days, have you attempted suicide or tried to kill yourself?” Respondents could report one of three mutually exclusive categories: (1) no suicide attempt; (2) a suicide attempt; or (3) a suicide attempt “only when high or in withdrawal from alcohol or drugs.”
bCategory includes women who identified as Asian, Native Hawaiian, or Pacific Islander, or “some other race” and those who selected multiple races due to very small cell sizes.
cOther category includes women who indicated they had commercial insurance, self-pay, or were uninsured.
dU.S. Census Bureau regions: Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming. https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf.
eSingle category includes individuals who identified as divorced, separated, or widowed.
f“Other” living situation category includes halfway house, supervised living facility, prison or jail, or hospital.
gSeverity scores are calculated via an algorithm that is dependent upon answers to various questions presented in the ASI-MV. Scores are interpreted and presented as follows: no real problem (0–1); slight problem (2–3); moderate problem (4–5); considerable problem (6–7); and extreme problem (8–9). For this analysis, scores were combined to compare between no real problem; slight, moderate, or considerable problem; and extreme problem.
GED, General Educational Development test; NAVIPPRO®, National Addictions Vigilance Intervention and Prevention Program.
Nearly three-quarters (72.9%) of women self-reported a diagnosis of depression or anxiety (Table 2). Almost one-third (31.7%) reported a diagnosis of manic depression or bipolar disorder. More than one-third (35.9%) reported a diagnosis of posttraumatic stress disorder. More than one-third (37.8%) of the women reported at least one overdose in which they needed someone else’s help to recover in their lifetime. Approximately 40% of the women reported an ongoing physical or medical problem that limits or interferes with daily activities, and almost half (48.7%) reported having a pain problem.
Past 30-Day Suicide Attempt Among Women of Reproductive Age with Past 30-Day Nonmedical Prescription Opioid Use, by Medical Conditions and Circumstances, National Addictions Vigilance Intervention and Prevention Program 2018–2020
Data were obtained from responses to the NAVIPPRO® Addiction Severity Index–Multimedia Version tool during first intake assessment for substance use at 338 program locations in 35 states. Nonmedical prescription opioid use is any use that is not considered “use as prescribed.” “Use as prescribed” was defined as (1) having a current pain problem and taking a prescribed opioid medication for pain in the past 30 days; (2) obtaining the medication only from one’s own prescription; and (3) no use of the medication via an alternate route of administration. Nonmedical use was also assigned if a respondent indicated having used the prescription opioid medication “not in a way prescribed by your doctor, that is, for the way it makes you feel and not for pain relief.”
aPast 30-day suicide attempt was defined using the question, “In the past 30 days, have you attempted suicide or tried to kill yourself?” Respondents could report one of three mutually exclusive categories: (1) no suicide attempt; (2) a suicide attempt; or (3) a suicide attempt “only when high or in withdrawal from alcohol or drugs.”
bDissociative identity disorder was added to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition in 1994 to replace multiple personality disorder and reflect a better understanding of the condition, namely, that it is characterized by fragmentation or splintering of identity, rather than by proliferation or growth of separate personalities.
cIntentionality not specified.
GED, General Educational Development test; NAVIPPRO®, the National Addictions Vigilance Intervention and Prevention Program.
Non-Hispanic Black women had the highest rates of suicide attempt (4.5%). Non-Hispanic American Indian/Alaska Native (AI/AN) women had both the second highest rate of suicide attempt (4.4%) and the highest rate of suicide attempt “only when high or in withdrawal from alcohol or drugs” (2.7%) (Fig. 1).
After adjusting for sociodemographic, social, medical, and legal circumstances and conditions, the adjusted odds of past 30-day suicide attempt were significantly higher for women aged 18–24 years (versus women aged 25–34 years), non-Hispanic Black women, and non-Hispanic AI/AN women (versus non-Hispanic White women) (Table 3). In addition, adjusted odds of past 30-day suicide attempt was significantly higher among women who reported no stable living arrangement or other living situation (versus women living in a private home or apartment); women who reported a history of emotional, physical, or sexual abuse (versus women with no history of emotional, physical, or sexual abuse); women who reported being extremely bothered by family problems in the past 30 days (versus women not at all bothered by family problems in the past 30 days); women who reported being slightly, moderately, or considerably bothered, or extremely bothered by physical or medical problems in the past 30 days (versus women not at all bothered by physical or medical problems in the past 30 days); and women who reported a slight, moderate, or considerable problem with alcohol, or an extreme problem with alcohol (versus women with no real problem with alcohol): the largest magnitude of association for this outcome. Women who reported being on probation or parole had lower odds of past 30-day suicide attempt compared with women reporting not being on probation or parole. Significantly higher adjusted odds of past 30-day suicide attempt were observed for women with a diagnosis of manic depression or bipolar disorder (versus women with no manic depression or bipolar diagnosis), a diagnosis of posttraumatic stress disorder (versus women with no posttraumatic stress disorder diagnosis), and women who reported at least one overdose where they needed someone else’s help to recover in their lifetime (versus women who reported zero lifetime overdoses where they needed someone else’s help to recover).
Crude and Adjusted Odd Ratios of Past 30-Day Suicide Attempt Among Women of Reproductive Age with Past 30-Day Nonmedical Prescription Opioid Use, National Addictions Vigilance Intervention and Prevention Program 2018–2020
Data were obtained from responses to the NAVIPPRO® Addiction Severity Index–Multimedia Version (ASI-MV) tool during first intake assessment for substance use at 338 program locations in 35 states. Bold font indicates statistical significance. Nonmedical prescription opioid use is any use that is not considered “use as prescribed.” “Use as prescribed” was defined as (1) having a current pain problem and taking a prescribed opioid medication for pain in the past 30 days; (2) obtaining the medication only from one’s own prescription; and (3) no use of the medication via an alternate route of administration. Nonmedical use was also assigned if a respondent indicated having used the prescription opioid medication “not in a way prescribed by your doctor, that is, for the way it makes you feel and not for pain relief.”
aPast 30-day suicide attempt was defined using the question, “In the past 30 days, have you attempted suicide or tried to kill yourself?” Respondents could report one of three mutually exclusive categories: (1) no suicide attempt; (2) a suicide attempt; or (3) a suicide attempt “only when high or in withdrawal from alcohol or drugs.”
bMultinomial logistic regression models adjusted for all characteristics listed in the table.
cCategory includes women who identified as Asian, Native Hawaiian, or Pacific Islander, or “some other race,” as well as those who selected multiple races due to very small cell sizes.
dOther category includes women who indicated they had commercial insurance, self-pay, or were uninsured.
eSingle category includes individuals who identified as divorced, separated, or widowed.
f“Other” living situation category includes halfway house, supervised living facility, prison or jail, or hospital.
gSeverity scores are calculated via an algorithm that is dependent upon answers to various questions presented in the ASI-MV. Scores are interpreted and presented as follows: no real problem (0–1); slight problem (2–3); moderate problem (4–5); considerable problem (6–7); and extreme problem (8–9). For this analysis, scores were combined to compare between no real problem; slight, moderate, or considerable problem; and extreme problem.
hIntentionality not specified.
CI, confidence interval; GED, General Educational Development test; NAVIPPRO®, the National Addictions Vigilance Intervention and Prevention Program; OR, odds ratio.
Similarly, the adjusted odds of past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs” were significantly higher for women aged 18–24 years (versus women aged 25–34 years); women who reported no stable living arrangement (the largest measure of association for this outcome) or other living situation (versus women living in a private home or apartment); women who reported being slightly, moderately, or considerably bothered, or extremely bothered by family problems in the past 30 days (versus women not at all bothered by family problems in the past 30 days); women who reported a slight, moderate, or considerable problem, or an extreme problem with alcohol (versus women with no real problem with alcohol); and women who reported at least one lifetime overdose in which they needed someone else’s help to recover (versus women who reported zero lifetime overdoses where they needed someone else’s help to recover). Women who were on probation or parole had lower odds of past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs” compared with women reporting not being on probation or parole.
Discussion
In this study using data collected from reproductive-age women undergoing their first intake assessment for substance use treatment at 338 substance abuse treatment center locations in 35 states in 2018–2020, we found that 2.7% of women with past 30-day nonmedical prescription opioid use reported a past 30-day suicide attempt and 1.5% reported a past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs.” Over one-third reported at least one overdose where they needed someone else’s help to recover in their lifetime. Past 30-day suicide attempts varied by race and ethnicity: non-Hispanic Black women reported the highest rate of past 30-day suicide attempt (4.5%), and non-Hispanic AI/AN women reported the highest rates of suicide attempt “only when high or in withdrawal from alcohol or drugs” (2.7%). Consistent with previous research on factors associated with suicide attempt, multiple sociodemographic, social, medical, legal circumstances, and conditions such as housing instability, experiencing family problems, substance misuse, and prior overdose were associated with higher adjusted odds of past 30-day suicide attempt and past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs.” 2,15,16
The rate of past 30-day suicide attempt (2.7%) among reproductive-age women with reported past 30-day nonmedical prescription opioid use is higher than rates of past-year suicide attempt reported among adults aged 18–25 years (1.9% in 2018 and 1.8% in 2019) and adults aged 26–49 years (0.5% in 2018 and 0.6% in 2019) in the 2019 report using National Survey on Drug Use and Health data. 17 It is difficult to find additional literature for comparison of prevalence estimates because of differing methodologies and populations included. Our finding that among women undergoing assessment for substance use treatment with past 30-day nonmedical prescription opioid use, 1.5% self-reported a past 30-day suicide attempt “only when high or in withdrawal from alcohol or drugs” adds to the body of literature on suicide attempt.
Among women with past 30-day nonmedical prescription opioid use and suicide attempt, the strongest magnitude of association was for an extreme alcohol problem; compared with women with no real problem with alcohol, women with an extreme alcohol problem had 2.84 times the odds of past 30-day suicide attempt in the adjusted model. Prescription opioids and alcohol are common substances identified in deaths by suicide overdose, occurring in 41% and 14% of cases, respectively, 18 and make up the largest proportion (31%) of suicide deaths due to multiple substance overdose. 19 Studies have found that greater frequency of prescription opioid use for reasons, including pain relief, relaxation, experimentation, to get high, to help with sleep, to help with feelings or emotions, to increase/decrease the effect of some other drug, or because of addiction, is associated with increased suicide thoughts and behaviors, 9,20 and acute use of alcohol (AUA) is associated with suicide fatalities and nonlethal suicide attempt. 21 AUA may precipitate suicide attempt by increasing dysphoria, aggression, and impulsivity; it may also weaken or remove barriers to self-harm by affecting one’s ability to find and use alternative coping strategies. 22 –25 In a 2017 analysis of AUA and risk of suicide attempt, a dose–response relationship between AUA and risk of suicide attempt was reported, such that the greater the AUA, the greater the odds of suicide attempt. 26 In addition, a 2004 study reported a 17-fold difference in standardized mortality ratios for suicide in women seeking alcohol treatment versus a 5-fold difference among men seeking alcohol treatment; in addition, they reported that women who use drugs and who have a history of suicide attempt have an 87-fold increase in suicides when compared with the general population. 27 The results of a 2018 report summarizing violent deaths from 27 states indicate that among deaths by suicide, history of suicide attempts is reported more frequently among women, and thus, addressing substance use and other comorbid conditions is important in reducing suicide rates. 28
In the current study, the association of both suicide attempt outcomes and one or more prior overdoses where help was needed to recover is consistent with findings from a previous study in a small nonclinical sample in which the number of prior opioid overdoses was associated with thoughts of suicide or a suicide attempt, independent of current depression. 29 Also, we found that non-Hispanic Black women and non-Hispanic AI/AN women had the highest rates of past 30-day suicide attempt and suicide attempt “only when high or in withdrawal from alcohol or drugs,” respectively. A report from 25 states and the District of Columbia showed disproportionate increases in overdose death rates during 2019–2020 among non-Hispanic Black and non-Hispanic AI/AN persons compared with non-Hispanic White persons and evidence that prior substance treatment was lowest among non-Hispanic Black persons. 30 An analysis of 2017–2019 Medicaid claims data also showed that among Medicaid patients, Hispanic persons, non-Hispanic Black persons, and non-Hispanic AIAN/Asian/Hawaiian/Pacific Islander persons have lower odds of receiving medications for opioid use disorder compared with non-Hispanic White Medicaid patients. 31
Our finding that both suicide attempt outcomes were associated with not having a stable living situation aligns with previous literature on suicide and housing instability. 32,33 Housing loss or instability may precipitate suicidal ideation or attempt by exacerbating existing mental health or substance use problems. 34,35 A study analyzing 2013–2016 Veterans Health Administration data showed that compared with unstably-housed female veterans aged 65 or older, the odds ratio for suicidal ideation among unstably-housed female veterans aged 18–39 years was 2.16 (95% CI: 1.04–4.49), and the odds ratio for suicide attempt was over 12 (aOR = 12.26, 95% CI: 3.00–50.05). 36
In the present study, the only factor associated with lower odds of both suicide outcomes was being on probation or parole. The direction of these relationships is unexpected. A 2022 meta-analysis found that women released from incarceration have more than three times greater risk of suicide compared with recently incarcerated men and nearly 15 times greater risk compared with nonincarcerated women. 37 A 2021 study found that recent arrest was associated with higher prevalence of suicide attempts compared with parole, probation, or no criminal justice involvement. 38 Our findings may differ from prior literature because the ASI-MV does not collect information on potential covariates such as time since arrest or time since incarceration.
The results in the present study have implications in clinical and public health settings. The nonmedical use of opioids and associated risk of suicidal behaviors remain a serious public health issue, and our findings highlight the need for continued surveillance of both opioid use and suicidal risk factors and behaviors in women of reproductive age. The Surgeon General’s Call to Action for suicide prevention recommends interventions that address individual-level mental health treatment while also focusing on teaching coping and problem-solving skills, strengthening relationships, and improving access and options for community- and societal-level support. 39 In addition, CDC’s Suicide Prevention Resource for Action provides examples of comprehensive and effective prevention efforts that address the multiple sociodemographic and medical influences on suicide behaviors. 2 Suicide prevention efforts recognize group-specific risk and protective factors and tailor interventions to appeal to different groups, including reproductive-age women. Our findings highlight the need for strategies and approaches to achieve and sustain reductions in suicide, including strengthening economic supports such as stable housing, creating protective environments that reduce substance use, teaching parenting skills to improve family relationships, and planning for safety and follow-up care after a suicide attempt. In 2022, CDC released updated national guidelines for clinicians prescribing opioids for pain care, with the goal of reducing the number of individuals who experience prescription opioid-related adverse events, including suicide. 40 These resources offer providers guidance on best practices related to both opioid use and suicide prevention, specifically for women.
Limitations
The findings in this report are subject to several limitations. First, ASI-MV data are self-reported and subject to recall, reporting, and social desirability biases. Second, to be included in our analysis, women had to self-report nonmedical use of prescription opioids. It is unknown how many met criteria for opioid use disorder. 41 Third, although ASI-MV captures data from a geographically diverse set of states and treatment programs, it is not population-based data. Geographic and site participation changes over time, and the network is not designed to be nationally representative. Thus, our results may not be generalizable to all women of reproductive age assessed for substance use at a substance treatment program or with nonmedical use of prescription opioids. Fourth, although women in this study were being assessed for substance use treatment, ASI-MV is used by the National Guard, public benefits offices, the criminal justice system, and others who purchase the assessment product, indicating that this analysis may include women who were not seeking substance use disorder treatment. It is unclear how many women this affects. The substance use treatment or criminal justice focus of some sites may capture important information on paths to engaging in treatment; however, this may also introduce inclusion bias. Fifth, due to small cell sizes, Asian, Native Hawaiian, and other Pacific Islander women were included in the “Another or multiple non-Hispanic race(s)” group. We acknowledge heterogeneity within the race and ethnicity groups but were unable to disaggregate the data further. Sixth, many variables in this analysis, including the primary outcome of suicide attempt, have a time bound of 30 days. Therefore, we are unable to measure the association between risk factors and suicide attempts that occur outside of these time bounds. Seventh, our final regression model was built to reflect the relationships between covariates and our outcomes; however, other combinations of covariates may result in more parsimonious models.
Conclusions
Our findings highlight that among reproductive-age women being assessed for substance use treatment with nonmedical prescription opioid use, past 30-day suicide attempt and suicide attempt “only when high or in withdrawal from alcohol or drugs” were associated with multiple sociodemographic, social, medical, legal circumstances, and conditions, such as housing instability, experiencing family problems, substance misuse, and prior overdose. Comprehensive, upstream public health suicide prevention initiatives and substance use treatment for women using opioids can address these circumstances and conditions.
IRB Status
This activity was conducted consistent with applicable federal law and Centers for Disease Control and Prevention policy (see, e.g., 45 C.F.R. part 46, 21 C.F.R. part 56, 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq).
Footnotes
Acknowledgments
This project was supported in part by an appointment to the Research Participation Program at the Centers for Disease Control and Prevention, administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and the Centers for Disease Control and Prevention.
Authors’ Contributions
E.K.K.: Led the literature review, contributed to data interpretation, prepared figures (visualizations), and led the preparation and revision of the final article. C.L.D.: Conceptualized the study, conducted all analyses, led data interpretation, drafted the original article, and critically reviewed and revised the final article. L.E.W.: Contributed to the conceptualization of the study and data interpretation and critically reviewed the final article. L.D. and M.T.: Contributed to data interpretation, critically reviewed the article for important intellectual content, and revised the final article. M.L.: Contributed to literature review, supported project administration, and reviewed and revised the final article. J.Y.K.: Led the conceptualization and design of the study, critically reviewed the article for important intellectual content, revised the final article, and provided supervision to article development. All authors contributed to and have approved the final article.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.