
Abstract
Introduction:
Recent outbreaks of measles (rubeola) have underscored the importance of immunity and vaccination. By late 2019, measles had a decade of rising cases, culminating in widespread outbreaks. The COVID-19 pandemic exacerbated this event due to disruptions in healthcare services. Unlike rubella, rubeola testing is not routinely performed in the United States. The objective of this study is to evaluate rubella and rubeola immunization status and the potential concordance between rubella and rubeola immunity.
Methods:
This was a retrospective study of patients treated at a single reproductive endocrinology clinic between January 1, 2015, and March 31, 2019. Patients were excluded if rubella or rubeola results were missing. Results were classified as immune (positive) or nonimmune (negative or indeterminate). Logistic regression analysis was used to predict immunity status based on factors such as age, body mass index, and race.
Results:
Of 524 cases, 387 (73.9%) patients were immune to both rubella and rubeola while 86 (16.4%) exhibited immunity to rubella only. There was a statistically significant difference in concordance between rubeola and rubella immunity (p = 0.0014) with more immune to rubella (90.3%, n = 473) compared with rubeola (72.2%, n = 415). Nearly two-thirds of patients reported receiving the measles, mumps, and rubella (MMR) vaccine (n = 361, 68.9%). Most patients were white/Caucasian (n = 442, 84.45%), obese or morbidly obese (n = 247, 47.1%), and >30 years old (n = 276, 52.7%).
Conclusions:
Rubella immunization status does not definitively predict rubeola immunity. Given increasing risk of measles outbreaks in the United States, prenatal testing for rubeola could prove beneficial.
Introduction
Despite its eradication in the year 2000, the United States has experienced a measles resurgence. From January 1 to December 31, 2019, 1,274 individual cases of measles were confirmed in 31 states becoming the year with the greatest number of reported cases in the United States since 1992. While the number of cases dropped from 2020 to 2023 with 13, 49, 121, and 58 confirmed cases respectively, as of August 15, 2024, there were already 219 cases. 1 Concurrently, there has been a decline in the vaccination rate among children in the United States, dropping to 92.7% by 2023, below the threshold required for herd immunity, which is ≥95%. 1 Meanwhile, globally, there has been an 18% surge in estimated measles cases in the years 2021–2022. 2 Between decreased vaccination rates and international travel, measles cases in the United States are becoming increasingly more common. Moreover, amid the COVID-19 pandemic, disruptions stemming from it compounded the conditions for this resurgence. At the peak of the pandemic, there were heightened disparities in vaccine access globally, along with a diversion of resources away from routine immunization, including the MMR vaccine. Consequently, this led to lingering immunity gaps and instances of missed vaccine doses. In addition, the relatively low number of reported cases in 2020 might also be attributed to the global focus on addressing the coronavirus resulting from strategies designed to mitigate the spread of transmissible disease as well as widespread disruptions in healthcare services. 3,4 Finally, there is a growing perception that vaccinations are either unsafe or unnecessary, leading to hesitancy toward vaccines and the rise of antivaccination movements. This reluctance stems from a mix of cultural or religious beliefs, misinformation, distrust in healthcare systems, and concerns over the perceived risks associated with vaccines. Notably, this encompasses the widely discussed yet subsequently retracted suggestion of a connection between autism and the MMR vaccine. 5
Measles, a highly contagious disease, presents with fever, coryza, conjunctivitis, cough, and an erythematous maculopapular rash. Although measles is often characterized as a largely benign childhood infection, it can result in serious complications like meningoencephalitis, corneal ulcers causing blindness, pneumonia, and myocarditis. 6 Complications secondary to measles are most common in young infants, pregnant women, immunocompromised young children, and seronegative adults. Thus, the rising number of measles cases has important implications for the health of pregnant women and neonates. Adverse pregnancy outcomes secondary to measles infection include spontaneous abortion, preterm delivery, low-birthweight neonates, and maternal/fetal death. 6 –8 Infants infected with measles are also at increased risk for complications, including subacute sclerosing panencephalitis, blindness, or death. 8,9 If maternal infection is acquired around the time of birth, neonatal risk for serious infection and complications increases significantly. 6
With the development of the measles, mumps, and rubella (MMR) vaccine, measles has become a preventable illness, found to be 97% effective at two doses and 93% effective at one dose in preventing infection. 1 Historically, breakthrough cases among fully vaccinated individuals typically are reported to be around 5%, and recent 2024 data are consistent with those of prior years. 1 Of the 284 measles cases reported in 2024, 4% received two doses of the MMR vaccine, 7% received one dose, and 89% of cases were reported as unvaccinated or unknown status. 1 Vaccination strategies have previously successfully reduced the spread of measles in the United States. Administration of the MMR vaccination is recommended in a two-dose series at 12–15 months and 4–6 years. In addition, vaccination in women before or during their reproductive years with the MMR vaccine is strongly recommended to avoid congenital infections or inadequate immunity in infants. 1,8 Unlike measles, rubella can be vertically transmitted directly to the fetus, causing congenital malformations such as microcephaly, cardiac defects, deafness, fetal growth restriction, placental insufficiency, or spontaneous abortion. With this risk for serious infection for the mother, fetus, and newborn, it is routine practice to test rubella antibody titers during pregnancy to determine risk. While the MMR vaccine cannot be given to pregnant patients, current guidelines suggest screening all pregnant women for rubella immunity and offering postpartum immunization to all susceptible mothers. Evidence of immunity includes written documentation of vaccination or laboratory evidence such as rubella IgG antibody testing. 10 However, the determination of measles immunity is not routinely performed in the United States, including in unvaccinated patients or those with unclear vaccination history. In these instances, it is unclear if immunity to rubella established with serological testing infers immunity to measles.
Limited evidence exists on whether identifying likely rubella immunity implies resistance to measles in pregnant women based on seropositivity given that both vaccines are included in the MMR formulation. Current data suggest that immunity to rubella is greater than immunity to measles in certain populations and that large percentages of those rubella immune demonstrate measles susceptibility. 11 –13 Nevertheless, the complexity arises from differences in MMR vaccination rates, international travel patterns, local regulations on immunization, and access to prenatal care, making it challenging to draw definitive conclusions. The primary aim of this study was to evaluate immunity to rubella and rubeola, and if there was a concordance between immunization status between the two.
Materials and Methods
This is a retrospective chart review study conducted at a single Midwestern reproductive endocrinology and infertility clinic. This study was approved by The University of Kansas Medical Center Institutional Review Board.
Patients aged ≥18 years and had received treatment at the facility between January 1, 2015, and March 31, 2019, were included in this study. After the medical record review, patients were excluded if either rubella or rubeola laboratory results were missing or incomplete.
Study data were abstracted from the electronic medical record system at the clinic and managed using the Research Electronic Data Capture tool hosted at the University of Kansas Medical Center. 14,15 The variables abstracted from the electronic medical records included race, body mass index, age, previous history of MMR vaccination obtained through patient self-report or vaccination records, rubella and rubeola immunity status, and date of testing. Results were classified as immune (tested positive) or nonimmune (tested negative or indeterminate) as determined by the commercial assay performing the test. The primary outcome of this study was immunity concordance between rubella and rubeola test results.
Data were managed using Microsoft Excel (Microsoft Corp, Redmond, WA). All statistical analyses were conducted using SAS 9.4 (SAS Int. Inc., Carry, NC). Frequencies, proportions, means, and standard deviations were calculated. Pearson’s chi-square and Fisher’s exact tests were used to test associations between two nominal or categorical variables in contingency tables. Logistic regression analysis was used to predict immunity to rubeola based on rubella immunity status, age, body mass index, and race. All statistical tests with p values ≤0.05 were considered significant.
Results
Of the 608 patients initially meeting inclusion criteria, 84 (13.8%) patients were excluded from the study due to missing lab results. The remaining 524 patients were included in the final cohort. The majority of patients were white/Caucasian (n = 442, 84.45%), obese or morbidly obese (n = 247, 47.1%), and older than 30 years old (n = 276, 52.7%). More than half of patients self-reported receiving the MMR vaccine (n = 361, 68.9%). Table 1 illustrates patient demographic and clinical characteristics.
Patient Demographics and Clinical Characteristics
Data are presented as n (%) or mean ± SD.
MMR, measles, mumps, and rubella.
Out of the total, 387 patients (73.9%) were found to be immune to both rubella and measles, as indicated in Table 2. In addition, 86 patients (16.4%) showed immunity to rubella but not to measles. Concordance of immunity between rubella and measles, assessed using a two-tailed z test for proportions, revealed a significant difference (p = 0.0014). It was observed that a higher proportion of patients were immune to rubella (90.3% [n = 473]) compared with measles (72.2% [n = 415]).
Concordance Between Rubella and Rubeola Immunity
Data are presented as n (%).
Several variables were analyzed to explore their possible association with rubella and rubeola immunity status; these variables included: race, body mass index category, and age category. Notably, there was no statistically significant difference between the immunity status for rubella (Table 3) or rubeola (Table 4) and any of the listed variables.
Rubella Immunity and Potential Associated Factors
Data are presented as n (%).
Rubeola Immunity and Potential Associated Factors
Data are presented as n (%).
Based on the Kappa (Κ = 0.18), there is poor agreement beyond chance that rubella immunity confers rubeola immunity (Fig. 1). The likelihood of being immune to rubeola is four times greater if the patient is immune to rubella (OR: 3.994; 95% CI: 2.165 to 7.366), when controlling for age (categorical), race, and body mass index.
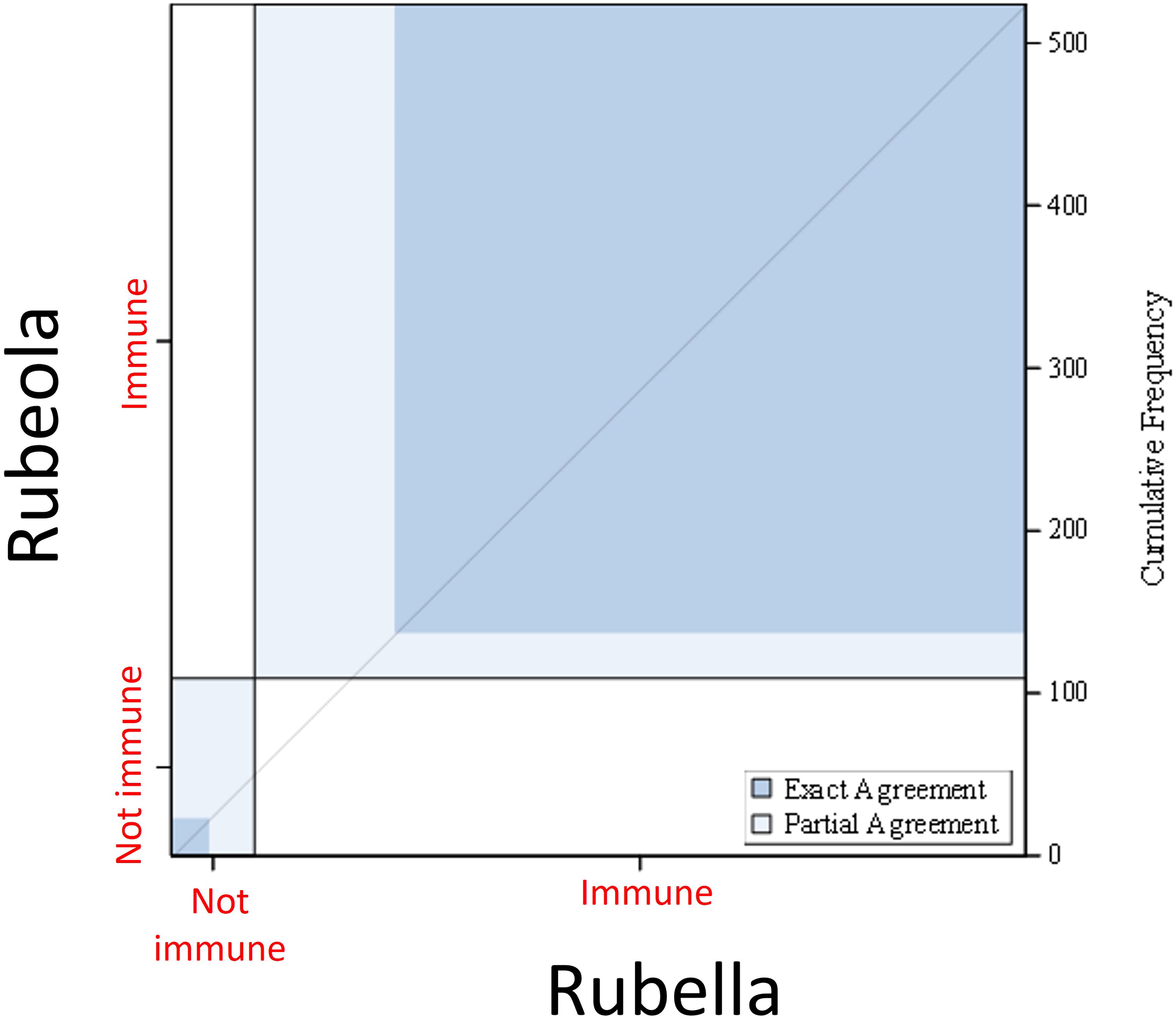
Agreement between rubella and rubeola immunity status. This figure illustrates the agreement between rubella and rubeola immunity status in the study population. The
Discussion
In our study population, we noted a measles serologic immunity rate of 72.2% and a rubella serologic immunity rate of 90.3% meaning that around one-third of these patients were serologically measles nonimmune. These figures contrast with the immunity rates reported in populations of similar studies. This includes a study performed by Lam et al. (2021) examining measles immunity in pregnant women in New York City showing higher immunity rates for both measles and rubella at 77% and 95%, respectively. 13 However, these differences may be explained by different MMR vaccine coverage between New York (97.9%) and Kansas (91.6%) as of 2023. 1 With vaccine coverage in the studied population being well below the percentage needed to confer herd immunity, measles susceptibility would be expected to be lower. However, this does not explain the differences in immunity between rubella and measles. One explanation is that seroconversion for measles following MMR vaccination is less than that of rubella. Schenk et al. (2021) found an estimated seroconversion rate of 96.0% (95% CI: 94.5–97.4) for measles and 98.3% (97.3–99.2) for rubella. 16 This would indicate susceptibility to measles may be greater even in vaccinated populations.
In our study, it was observed that rubella immunization status alone does not conclusively confer immunity to measles. Nevertheless, after adjusting for age, race, and body mass index, rubella immunity emerged as the sole predictive factor for measles immunity. We selected these specific variables for the following rationales: age, as older generations may have adhered more closely to MMR immunization recommendations; race, considering potential disparities in vaccination influenced by access, cultural or religious practices that may vary among different racial groups; and body mass index, since obesity could potentially impact immunity, and the prevalence of obesity in the United States is increasing.
The goal of prenatal testing for rubella immunity is to identify women who are candidates for vaccination in the postpartum period as the MMR vaccine is contraindicated in pregnancy. 8 Since the rubella vaccine was licensed in 1969, rubella-associated morbidity and mortality along with the incidence of congenital rubella syndrome have significantly declined. 17 Likewise, after the measles vaccine was licensed in 1963, there has been a 99% reduction in the incidence of measles in the United States. 17 However, there has been a spike in measles infections in recent years both globally and within the United States. This may be credited in part to decreasing rates of MMR administration due to vaccine hesitancy secondary to several factors including disruptions in vaccination schedules or missed doses secondary to COVID-19, individual patient cultural or religious beliefs, distrust in health care systems, or concerns over the perceived risks associated with vaccines. When communities experience an outbreak, there is often fear among obstetrics providers and patients may inquire about their own immunity status. Providers may use the patient’s reported vaccination status as evidence. If providers perform a rubeola IgG, they may find apparent nonimmunity or indeterminant results. This could lead to significant confusion and fear and there is a high likelihood based on current vaccination trends that these episodes will occur more frequently.
Our study has several strengths, including a relatively large sample size, minimized misclassification bias, and comprehensive medical records. However, a potential limitation lies in the inconsistency of MMR vaccination records from patient medical records. We cannot distinguish whether the information originates from official immunization documentation or patient self-reporting. In addition, it is important to note the cutoff values used to determine immunity status vary by the commercial assay. This variability underscores the challenge of comparing serological results between testing platforms without standardization of serological testing methods. Our data were obtained from primarily Caucasian women from the Midwest who were patients at a fertility clinic, thereby restricting generalizability. Nonetheless, our findings align with previous research that encompassed larger and more diverse samples, including both genders and individuals from various racial and demographic backgrounds across the United States. 11 –13 Another limitation arises from our inability to control the timing of previous vaccinations. This is particularly relevant considering the 1998 adjustment in the vaccination schedule, which changed the administration of the second dose to ages 4–6 years from the previous 6–12 years. 18 This adjustment is crucial in studies involving women of reproductive age when considering waning long-term immunity following their second dose.
Conclusions
In conclusion, rubella immunity did not infer measles immunity within our population. In the event of a measles outbreak, immunity to measles cannot be assumed solely based on known rubella immunity. Although most of the population has received MMR immunization, the risks of measles in pregnancy and serious infection in nonimmune newborns suggest clinicians should test for measles immunity in the event of possible exposure even if rubella immunity has been established. 19 Prior vaccination guidance was based upon an assumption of historically high herd immunity rates; however, vaccination guidelines may need to be reevaluated as population acceptance of vaccination recommendations changes. Moreover, considering the escalating risk of measles outbreaks in the United States, coupled with increasingly insufficient vaccine coverage, incorporating measles serology into prenatal testing could help identify and manage pregnancies at risk more effectively.
Footnotes
Acknowledgments
The authors thank Nikhita Ravikanti, MD, for critical review and contributions during the article writing process and Bruce Tjaden, MD, for support during the data collection process.
Authors’ Contributions
R.M.: Conceptualization (supporting), investigation (lead), visualization (lead), writing—original draft (lead), and writing—review and editing (supporting). K.M.C.: Investigation (supporting), writing—original draft (supporting), and writing—review and editing (supporting). H.O.: Formal analysis (lead), methodology (supporting), visualization (supporting), writing—original draft (supporting), and writing—review and editing (supporting). J.K.: Conceptualization (supporting), data curation (lead), investigation (supporting), methodology (supporting), project administration (lead), visualization (supporting), writing—original draft (supporting), and writing—review and editing (supporting). D.W.: Visualization (supporting) and writing—review and editing (supporting). D.A.G.: Conceptualization (supporting), investigation (supporting), visualization (supporting), writing—original draft (supporting), and writing—review and editing (supporting). L.T.: Conceptualization (lead), investigation (supporting), methodology (lead), project administration (supporting), supervision (lead), visualization (supporting), writing—original draft (supporting), and writing—review and editing (lead).
Author Disclosure Statement
The authors report no conflicts of interest or disclosures.
Funding Information
No funding was received for this article.