
Abstract
Rationale:
Obstructive sleep apnea (OSA) during pregnancy is linked to negative maternal and neonatal outcomes. Diagnosing OSA in this population is particularly challenging. Portable monitoring devices (PMD) present a potential alternative to polysomnography (PSG), but their effectiveness in pregnant women is uncertain.
Objective:
To evaluate diagnostic accuracy of a PMD to detect OSA in pregnant women.
Methods:
A prospective study of 136 middle-aged pregnant women (34 ± 4 years) in their third trimester of pregnancy (34 ± 3 weeks) who underwent laboratory type III PMD and PSG simultaneously.
Results:
Using an apnea-hypopnea index (AHI) ≥5 event/h by PSG, OSA was diagnosed in 10.3% of women (mild OSA: 86%; moderate OSA: 14%). An acceptable positive correlation was found between both tests in the AHI (r = 0.787; p < 0.001) and oxygen desaturation index (ODI) (r = 0.806; p < 0.001). The agreement limits between PSG and type III PMD were −4.1 to 5.4 for AHI and −6.0 to 4.5 for ODI. The sensitivity and specificity of type III PMD for an AHI ≥5 events/h were 57.1% and 99.2%, respectively, with a positive predictive value (PPV) of 88.9% and a negative predictive value (NPV) of 95.3%. On a receiver operating characteristic curve, the best cutoff point of AHI by type III PMD to identify OSA according to PSG criteria was 2.25 events/h. The sensibility and specificity for this point were 85.7% and 88.5%, respectively, with a PPV of 46.2% and NPV of 98.2%.
Conclusions:
A type III PMD with an AHI cutoff of 5 events/h could be a good alternative for OSA diagnosis in pregnant women. Additionally, an AHI ≥2.25 event/h demonstrates good diagnostic performance, but its low positive predictive value suggests that it is more appropriate as a screening tool. Further studies are needed to validate this sleep study tool in pregnant women, particularly in home settings.
Introduction
Obstructive sleep apnea (OSA) is a disorder characterized by the presence of repetitive episodes of total or partial airflow interruption in the upper airway during sleep despite increased respiratory effort. 1 Women present a specific OSA phenotype, 2 and prevalence of OSA during pregnancy increases due to some physiological changes, such as weight gain, hormonal changes, or modifications in the upper airway. 3,4 Previous studies suggest a possible association between OSA with adverse pregnancy outcomes, such as insulin resistance, gestational diabetes, preeclampsia, 5 –13 and fetal-related outcomes, such as preterm birth and neonatal low weight 12,13 (Fig. 1).
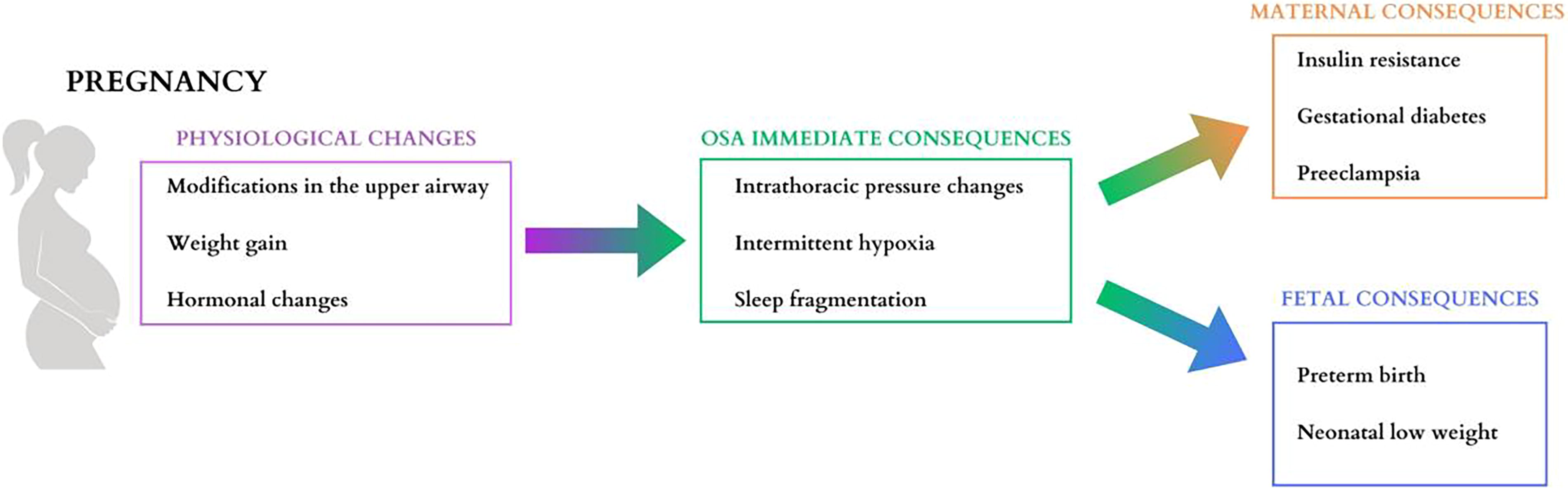
Physiological changes induced by pregnancy that contribute to obstructive sleep apnea (OSA) and their maternal and fetal consequences.
Snoring and daytime somnolence are remarkable OSA symptoms, although with a poor predictive value for its diagnosis during pregnancy. 10,14 –16 There are some questionnaires and clinical models for screening OSA during pregnancy that could be useful in identifying patients at high risk for the disease. However, these tools have a low level of precision in diagnosing OSA at any level of the apnea-hypopnea index (AHI) compared with sleep polysomnography. 10,15,17,18 Furthermore, most of them were limited as they included small samples of high-risk pregnant women, mostly with obesity. Although promising, these risk prediction tools must be prospectively validated in large groups of pregnant women to avoid the influence of important confounding factors, such as obesity, ethnic background, and maternal age. Currently, the definitive diagnosis of OSA during pregnancy should be still based on polysomnography (PSG). 11 However, PSG is an expensive resource-intensive test that requires an overnight hospital stay, which contributes to underdiagnosis of OSA in pregnant women.
For these reasons, portable monitoring devices (PMD) are an alternative for simplified OSA diagnosis. However, poor sleep quality and disturbed sleep are extremely common during pregnancy, 19 and PMD could potentially underestimate the true burden of the sleep-respiratory disease in this population. The two main limitations of PMD stem from the absence of electroencephalogram signals, which prevent the accurate detection of the total sleep time (TST) and arousal-related hypopneas, leading to an underestimation of the AHI.
In the past years, several type II and III PMD have been successfully validated against PSG in the general population. 20 –22 However, very few studies have focused on pregnant women. 23 –28 Many of these studies were limited by small sample sizes and predominantly included women with pre-pregnancy obesity, making the findings less applicable for diagnosing OSA during pregnancy using PMD.
Given the growing evidence of increased OSA prevalence and its association with significant adverse maternal and perinatal outcomes, further research is needed to develop simpler, more efficient, and highly accurate diagnostic methods for OSA diagnosis. Larger studies are essential to clarify the influence of key confounding factors such as obesity, age, and comorbidities. To this aim, we designed a study to evaluate the accuracy of a type III PMD in comparison to traditional lab-based PSG during the third trimester of pregnancy.
Materials and Methods
Study design and participants
A prospective cohort study was performed at two university hospitals, namely, Son Espases and Araba, in Spain. Consecutive singleton adult pregnant women in the third trimester were included. Participants were excluded if they fulfilled at least one of the following exclusion criteria: (1) unwillingness or inability to participate in the study; (2) previous OSA; (3) previous diabetes mellitus, pulmonary, heart or kidney diseases; (4) multiple gestation; (5) imminent delivery due to maternal-fetal disease; and/or (6) any other concurrent severe medical condition that in the opinion of the investigator would interfere in the study.
The Institutional Ethic Committee of the Balearic Islands approved the study (IB1510/10PI) and all subjects gave their written informed consent.
The strengthening the reporting of observational studies in epidemiology (STROBE) standards for reporting observational studies were followed.
Clinical variables
In all subjects anthropometric, clinical, and sleep data were collected based on the same set of information using questionnaires and direct measurements that included age, body mass index (BMI), comorbidities, alcohol intake, and tobacco consumption. Neck, waist, and hip circumferences were measured at the levels of the cricothyroid membrane, at the point equidistant between the iliac crest and the lowest rib, and at the point of greater trochanter, respectively. Office blood pressure was measured by a random-zero sphygmomanometer with the woman seated for at least 5 minutes. Recorded values were the mean of three readings. Episodes of subjective asphyxia, snoring, bed partner-reported sleep breathing pauses, nocturia, morning headache, and morning tiredness were collected in five degrees of intensity (never, sometimes, frequently, almost always, and always); subjective nocturnal sleep time and daytime sleepiness (Epworth sleepiness scale [ESS]) 29 were recorded over the previous 4 weeks.
Polysomnography
Overnight-attended PSG (Grael PSG-EEG 4K, Compumedics, Abbotsford, Australia; Alice 5, Philips Respironics, Inc., PA, USA) was performed in the sleep laboratory and manually scored using conventional criteria. 30,31 Six electroencephalograms (EEG), two electrooculograms, and two chin electrodes were used to obtain the neurobiological signals. Sleep was analyzed using the standard criteria for epochs of 30 seconds. Breathing was monitored using nasal cannulas (pressure-based airflow), oronasal thermistors, and thoracoabdominal effort bands. Simultaneously, oxyhemoglobin saturation (SpO2) was monitored with a pulse oximeter. Apnea was defined as the absence of airflow (>90% reduction) for at least 10 seconds and a hypopnea as a discernible airflow reduction (>30% and <90%) for at least 10 seconds with a ≥3% drop in SpO2 or related arousal. AHI was established as the number of apneas/hypopneas per hour of sleep. OSA was defined when AHI was ≥5 event/h. AHI in supine was calculated as the number of apneas/hypopneas in supine divided by TST in supine position. The mean SpO2, minimum SpO2 (lowest value recorded during sleep), TST spent with SpO2 < 90% (T90), and the number of ≥3% drops in SpO2 per hour of sleep (oxygen desaturation index [ODI]) were also computed.
Portable monitoring device
We used an Alice PDX (Philips Respironics, Murrysville, PA) polygraph, a type III PMD, which included nasal cannula (pressure-based airflow with snore detection), oronasal thermistor (oronasal temperature differences), thoracic and abdominal gauges (thoracic and abdominal effort), oximeter probe (SpO2 and pulse rate), and body position.
The technician set up both the conventional PSG and type III PMD, to be performed simultaneously. Airflow was measured using a single nasal cannula with a Y-shaped splitter, allowing the airflow signals to be recorded by both devices. All sleep studies were analyzed manually by sleep experts.
All sleep studies, both PSG and PMD, were analyzed by the same sleep expert at each center using standardized scoring criteria in accordance with the guidelines of the American Academy of Sleep Medicine (AASM). 30 This ensured consistency in the analysis and minimized the potential for systematic bias between devices. The type III PMD data were analyzed using adapted scoring criteria based on the AASM guidelines for full PSG. Respiratory events were manually scored using the aforementioned criteria but without the final arousal criteria for hypopnea, and the number of apneas and hypopneas were divided by the recording time to calculate AHI.
Statistical analysis
Descriptive results were expressed as mean ± standard deviation or percentages, depending on the nature of the variables. The paired t test and Pearson’s correlation were used to compare and correlate continuous variables from PSG and type III PMD, respectively. Agreement between the variables obtained from PSG and type III PMD was evaluated using the Bland and Altman method. In this method, the x-axis represents the mean value or the variables from both PSG and type III PMD, while the y-axis shows the difference between these values. The limits of agreement between the methods were calculated as the overall mean of the differences ± 1.96 times the standard deviation. The diagnostic validity of several type III PMD AHI cutoff points was evaluated with respect to an AHI ≥5 event/h on standard PSG, and the corresponding receiver operating characteristic (ROC) curve was generated. Youden’s index was applied to determine the optimal cutoff point. Diagnostic properties such as sensitivity, specificity, positive and negative predictive values, and their respective 95% confidence intervals were calculated. Cutoff points that optimized sensitivity and specificity of the type III PMD were also determined. Agreement in AHI measurements between type III PMD and PSG was evaluated using overall agreement and the kappa statistic. Finally, all variables obtained from the type III PMD were entered into a stepwise forward multiple logistic regression analysis to identify independent factors associated with a diagnosis of OSA according to conventional polysomnographic criteria (AHI ≥5 events/h). Differences were considered statistically significant at a two-tailed p-value of <0.05. Statistical analyses were performed using SPSS version 26 (IBM Corporation, Armonk, NY, USA).
Results
Characteristics of participants
As shown in the flowchart of the study (Fig. 2), a total of 136 women in their 34 ± 3 weeks of pregnancy were included in the study. The mean age of the participants was 34 ± 4 years with a pregestational BMI of 23.8 ± 4.3 kg/m2 and a gestational BMI at the time of inclusion of 27.6 ± 4.1 kg/m2. During pregnancy, the mean weight gain was 10.1 ± 4.8 kg. A total of 5.9% were former smokers, and none reported alcohol consumption. General characteristics and lifestyle characteristics are summarized in Table 1.
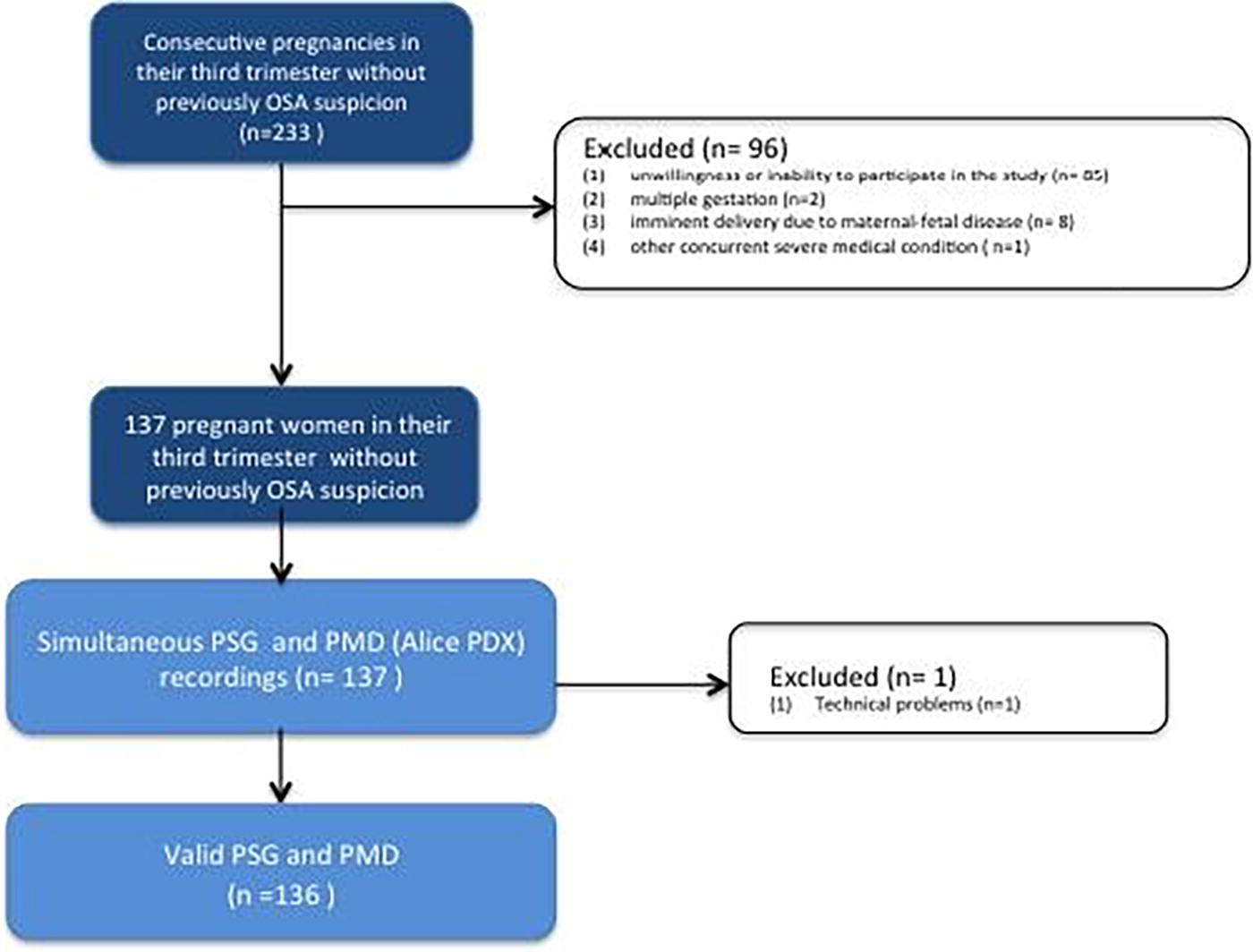
The flowchart of patient selection and causes of exclusion. OSA, obstructive sleep apnea; PMD, portable monitoring device; PSG, polysomnography.
General Characteristics and Lifestyle Characteristics of the Studied Population
Frequencies and percentages have been obtained for the categorical variables and mean (SD) for the continuous variables.
BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure; SD, standard deviation.
Regarding OSA symptoms, 54.5% of the included participants reported snoring, 20.7% experienced choking episodes, and 7% reported witnessed apneas. In terms of daytime symptoms, most participants did exhibit daytime hypersomnolence, with a mean ESS of 6 ± 3, although 63.9% reported restless sleep and 17.9% of morning headaches. Nocturia was present in 94.1% of the population, but its relationship with sleep disturbances or pregnancy could not be determined. In terms of upper airway findings, 40.9% of the women were classified as having class III-IV on the Mallampati scale. Other pathological characteristics were infrequent. Table 2 presents the sleep-related symptoms and physical examination findings.
Sleep Symptoms and Physical Examination Related to Obstructive Sleep Apnea (OSA) in Pregnant Women
Frequencies and percentages have been obtained for the categorical variables and mean (SD) for the continuous variables.
ESS, Epworth sleepiness scale; SD, standard deviation.
Comparison of the main variables from PSG and PMD
PSG outcomes showed a mean TST of 319 ± 67 minutes, with a predominance of light (stage N1 and N2) sleep (64 ± 11%) over deep (stage N3) sleep (23 ± 10%) and a percentage of rapid eye movement (REM) sleep at 13 ± 5%. OSA was diagnosed in 10.3% of the women, the majority of whom had mild OSA (85.7%), while only 14.3% had moderate OSA, and no severe OSA cases were found.
Main results of the sleep variables obtained from the PSG and type III PMD studies are summarized in Table 3. The study time in minutes was 435 ± 41 versus 439 ± 75, respectively. The type III PMD provided significantly higher values for central, obstructive, and mixed apnea indexes compared with PSG while exhibiting a lower hypopnea index. The AHI was slightly lower with type III PMD than with PSG, with no significant differences when measured in the supine position. Regarding oximetry, although no significant differences were detected in T90, the mean oxyhemoglobin saturation was higher with PSG than with type III PMD, while the minimum SpO2 and desaturation index were significantly greater with type III PMD compared with PSG.
Principal Characteristics of the Sleep Studies and Differences Between the Data Obtained from Polysomnography or Portable Monitoring Device
AHI, apnea-hypopnea index; ODI, oxygen desaturation index; OSA, obstructive sleep apnea; PMD, portable monitoring device; PSG, polysomnography; SD, standard deviation; SpO2, oxygen saturation; T90, % of time with oxygen saturation below 90%.
Correlation and concordance between PSG and PMD
When analyzing the correlation between the main variables of the sleep study, an acceptable correlation was found for the AHI (r = 0.787; p < 0.001) and the ODI (r = 0.806; p < 0.001) measured by both tests.
Bland and Altman’s concordance analysis identified the following agreement limits between PSG and type III PMD: −4.1 to 5.4 for AHI, −8.7 to 9.4 for supine AHI, −1.0 to 0.7 for central apnea index, −1.0 to 0.8 for obstructive apnea index, −3.8 to 5.6 for hypopnea index, −14.9 to 12.5 for T90, −6.0 to 4.5 for ODI (Fig. 3), −3.4 to 4.4 for mean SaO2, and −6.9 to 8.6 for minimum SpO2. In turn, we also evaluated the potential drift between the variables from type III PMD and PSG studies, appreciating a greater discordance in the AHI, T90, ODI, and mean SpO2 as their values rose (p < 0.001 in all cases).
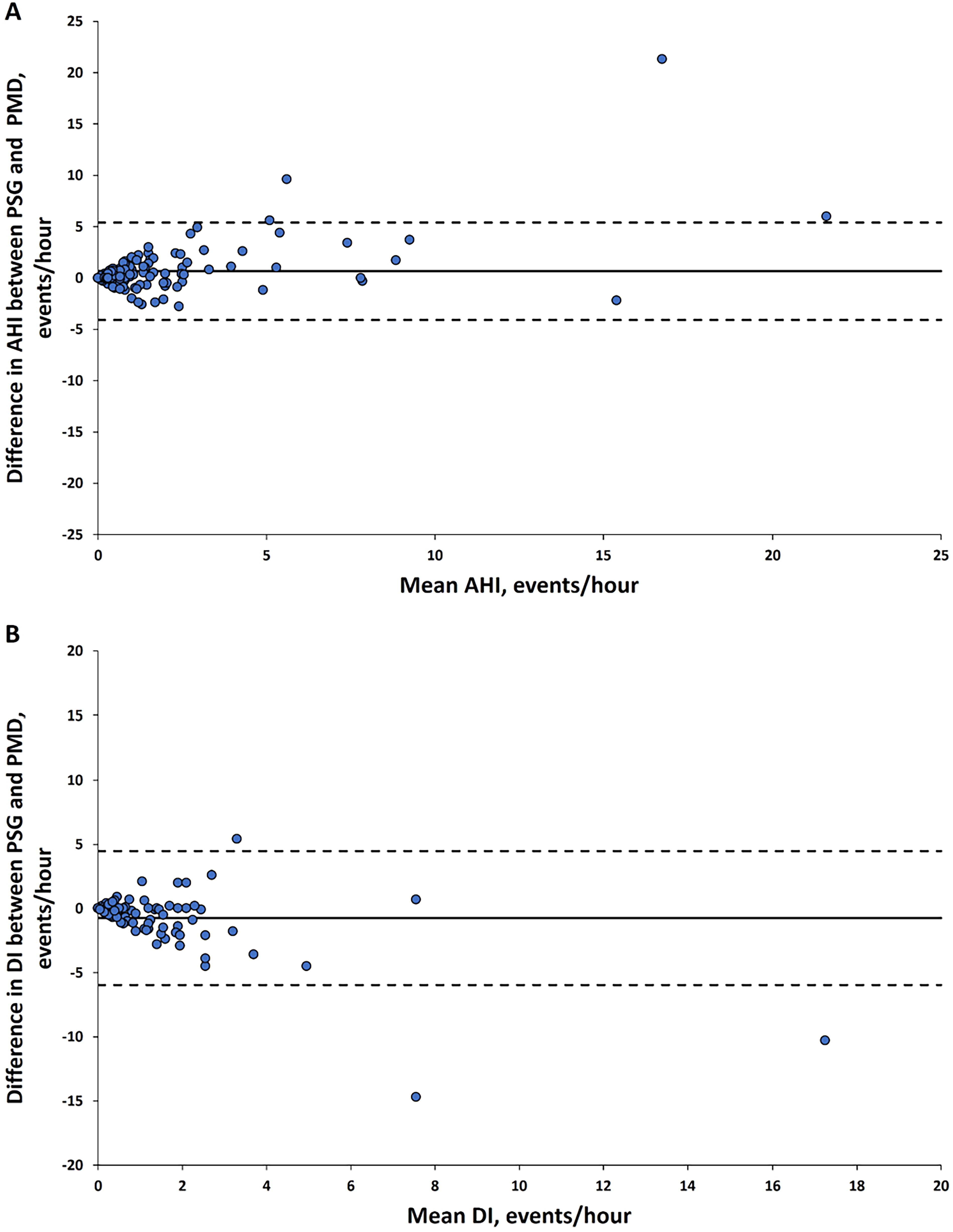
Bland Altman plots concordance analysis between the main parameters of sleep studies.
Diagnostic performance of PMD for OSA detection
In the PMD study, the sensitivity and specificity for an AHI ≥5 events/h were 57.1% and 99.2%, respectively, with a positive predictive value of 88.9% and a negative predictive value of 95.3%. A ROC curve was analyzed to predict OSA (AHI ≥5 events/h in PSG), identifying a cutoff point of AHI = 2.25 events/h in type III PMD. The sensitivity and specificity for this cutoff point were 85.7% and 88.5%, respectively, with a positive predictive value of 46.2% and a negative predictive value of 98.2%. Additionally, the concordance between this cut point and PSG criteria (AHI ≥5 events/h) was assessed, yielding a kappa value of 0.538.
In the multivariate analysis to identify OSA (PSG AHI ≥5 events/h) using type III PMD, the AHI and minimum SpO2 variables were retained, with Nagelkerke’s r 2 values of 0.632 and 0.678, respectively (Table 4).
PMD Parameters Independently Associated with the OSA Diagnosis in a Multivariate Logistic Regression Analysis
AHI, apnea-hypopnea index; B, regression coefficient; CI, confidence interval; OR, odds ratio; SE, standard error; SpO2, oxyhemoglobin saturation.
Discussion
OSA during pregnancy is an increasingly concerning topic due to its negative implications for both the mother and the neonate. This study evaluates a type III PMD as a viable alternative to PSG for detecting OSA in pregnant women, a group where diagnosis can be challenged by symptom variability and the influence of factors such as obesity and age. The underdiagnosis associated with the inconvenience and high costs underscores the need for validating of PMD in this population. Our results reveal that 10.3% of the pregnant women evaluated were diagnosed with OSA, predominantly with mild cases. This prevalence is significant, as it exceeds that of women of similar age from the same geographic area (3.4%). Furthermore, identifying these cases could be crucial to prevent maternal and neonatal complications, such as lower Apgar scores and birth weights.
We observed statistically significant differences between PSG and type III PMD in central, obstructive, mixed apnea, hypopnea indexes, and AHI. These differences can be attributed to several factors: respiratory indexes in type III PMD are influenced by a higher denominator (total recording time) compared with PSG (total sleep time); hypopnea events defined by arousal criteria are exclusive to PSG, leading to fewer hypopneas detected in type III PMD; events beginning during wake epochs are excluded in PSG but may be counted in type III PMD; and scorer variability between devices may introduce minor inconsistencies. Importantly, the observed differences were minor (<0.9 events/h) and unlikely to be clinically significant. Regarding oximetry, the minimum SpO2 value was slightly higher in type III PMD (by 1%), a discrepancy likely explained by variations in oximeter technologies.
Few studies have addressed this topic, often with important limitations, 23 –28 mainly related to small sample sizes and a high probability of OSA and obesity among participants. O’Brien et al. 23 conducted a prospective cohort study with 31 pregnant women, averaging 30.2 ± 7.1 years in age, 33.4 ± 3.0 weeks in gestational age, and 31.9 ± 8.1 kg/m2 in BMI. They compared ambulatory PSG with the Watch-PAT 200 device, concluding that Watch-PAT demonstrated high sensitivity and specificity in detecting OSA (AHI ≥5 on full PSG) in pregnant women, suggesting potential for conducting diagnostic ambulatory studies in this population. However, it may overestimate respiratory disturbance index (RDI), especially at higher levels.
Sharkey et al. 24 assessed the validity of the Apnea Risk Evaluation System (ARES) in a small sample of pregnant women. They found that the ARES provided the best balance between sensitivity (1.0 for PSG RDI, 0.91 for PSG RDI) and specificity (0.5 for PSG AHI, 0.8 for PSG RDI) for detecting OSA, demonstrating a reasonable consistency with PSG. However, the study primarily included severely obese women with a high pretest clinical probability of OSA. A more extensive validation study compared level III Alice PDX with attended PSG during late pregnancy, involving 149 participants in the third trimester of gestation but showing low agreement in AHI scores. 25 Our study included a well-characterized population of 136 pregnant women, consecutively enrolled without previously OSA suspicion. The mean pregestational BMI was 23.8 kg/m2, with a weight gain of 10.1 kg during pregnancy, indicating that our population was more representative of a general pregnancy cohort. This reinforces the diagnostic test’s validity in detecting OSA, because it demonstrates its effectiveness in a broader population of pregnant women, including those without previously suspected OSA or overt clinical risk factors such as obesity. By evaluating a more typical cohort, the results suggest that the test could have broader applicability in routine clinical practice, extending beyond high-risk cases and serving as a valuable tool for earlier detection of OSA in pregnant women.
In the past 5 years, efforts have continued to validate ambulatory studies in pregnant women for the diagnosis of OSA. Facco et al. 26 recruited a total of 43 obese pregnant women to evaluate a type III PMD performance finding high intraclass correlation and categorical agreement among PMD-auto scores, PMD-tech scores, and in-lab PSG results.
Moreover, Wang et al. 27 evaluated 92 pregnant women (average age 34.5 ± 4.3 years, gestational age 25.4 ± 8.9 weeks, BMI 29.9 ± 4.7 kg/m2) with suspected OSA using the Nox T3 portable monitor, followed by overnight PSG and a laboratory PMD within 1 week. The PMD achieved 91% sensitivity, 85% specificity, 84% positive predictive value, and 92% negative predictive value compared with PSG.
More recently, Clements et al. 28 assessed self-applied, unattended PSG using the Somte PSG V2 in pregnant women during early to mid-gestation. Specifically, the home-based Somte setup included EEG (F3/F4, M1/M2), electrooculography (E1/E2), chin EMG, electrocardiogram, airflow (pressure transducer), snore, airflow (thermistor), respiratory effort (abdomen and thoracic), oximeter, and position sensor, enabling reliable detection of respiratory effort related arousals (RERAs) and subsequent calculation of RDI.
Twenty-four participants completed both Somte and attended PSG tests, showing no significant difference in AHI and RDI measurements. Somte demonstrated high diagnostic accuracy, with an area under the ROC curve of 0.94 for AHI and 0.95 for RDI. However, technical issues were noted, and Somte may not detect all OSA cases, especially when RDI is used as a diagnostic criterion. Thus, while Somte could serve as a viable alternative to PSG in this population, caution is warranted regarding its limitations. The strength of the referenced study lies in its inclusion of EEG channels in a PMD, which allowed for the detection of respiratory effort-related sleep arousal and calculation of the RDI. In contrast, the PMD used in our study did not include EEG channels. These studies have the limitation that diagnostic tests were conducted at different times. In our study both tests (PSG and PMD) were undergone at the same time in the sleep laboratory, addressing the intrinsic changes occurring constantly during pregnancy and along nights that could be responsible for different sleep results over time. Moreover, although incorporating EEG signals into a self-applied, unattended PMD is promising, certain limitations should be considered. Only 24 women were ultimately included, while 133 patients declined to participate. Furthermore, despite the availability of a study coordinator for technical phone support during setup and data collection, 14% of women were excluded due to system start-up failures, and technical difficulties resulting in signal loss or dropout were reported in 54.2% of studies. These issues highlight the challenges associated with the application of this device.
Our study demonstrates a satisfactory correlation in key severity parameters for OSA (AHI and ODI) when measured by type III PMD, enabling the identification of patients with an AHI ≥5 event/h with PSG. An AHI cutoff point of 2.25 event/h using type III PMD showed good concordance with an AHI ≥5 events/h measured on PSG. However, its limited positive predictive value makes it more suitable for excluding rather than confirming OSA, supporting its utility as a screening tool. This correlation exhibited increasing variability at higher AHI and ODI values, likely reflecting the absence of severe OSA cases in our study population. Therefore, it seems reasonable to apply an AHI cutoff point of 5 events/h with type III PMD to confirm OSA diagnosis in pregnant women. These findings suggest that, in the absence of PSG, the type III PMD could serve as a valid tool for identifying OSA in this population, with potential improvements in diagnostic performance among individuals with a higher pretest probability of OSA.
The main strengths of this study were (1) its multicenter and prospective design, including women at the same pregnancy stage; 2) its large sample size; 3) the use of a consistent protocol with simultaneous measurement of sleep parameters via PSG and type III PMD conducted in a hospital setting; and 4) the shared respiratory flow measurement across both methods (PSG and type III PMD) using a Y-shaped design of the nasal cannula and the reception of a single signal.
Yet, as any study, it has some potential limitations that deserve to be commented on. First, the inclusion of patients with mild-to-moderate OSA limits further concordance analysis between PMD and PSG. Second, because our study included mainly Caucasian women in their third trimester, our results may not be directly applicable to other ethnic groups or to different gestational trimesters. Third, as positive predictive value and concordance are dependent on OSA prevalence, the positive predictive value and kappa index of PMD may be higher in other high-risk OSA populations. Fourth, PMD was performed in a hospital setting, while unattended and self-application of PMD would be applied at home by pregnant women. Fifth, a potential discomfort may arise from wearing duplicate equipment simultaneously, including effort bands, pulse oximeters, and thermistors for both the PSG and type III PMD systems. This setup, while necessary for simultaneous data collection, may have affected the participants’ sleep quality and overall experience during the study. Finally, regarding the event scoring criteria, our study utilized the 2007 and 2012 AASM scoring criteria. While these criteria have been widely validated, it is important to acknowledge that newer AASM criteria, such as version 3.0 (2022), may influence the scoring and calculation of the AHI.
This work demonstrates type III PMD can accurately diagnose OSA in their third trimester of pregnancy (34 ± 3 weeks). While the results are encouraging, further research is needed to validate PMD in diagnosing OSA in pregnant women, particularly in home settings. Additional studies could help establish clear protocols and optimize the use of these technologies in clinical practice. In conclusion, this study provides preliminary evidence that PMD may be a valuable alternative for diagnosing OSA in pregnant women.
Conclusions
PMD could be a viable alternative for OSA diagnosis in pregnant women when PSG is not available. An AHI cutoff point of 2.25 events/h measured by type III PMD demonstrated good concordance with an AHI ≥5 events/h as determined by full PSG. Further studies are necessary to establish this sleep study tool in pregnant women, particularly for home use.
Footnotes
Acknowledgments
The authors thank all the pregnant women for their willingness to participate in the study. Besides, the authors thank Meritxell Arqué for her assistance in the fieldwork of the study.
Authors’ Contributions
S.R.-P., A.A.F., O.M., and F.G.-R.: Conceptualized, administered, and supervised the study. A.A.F.: Designed the study protocol with the help of F.G.R. and A.A.F., F.G.R.: Analyzed the data. Funding acquisition was the responsibility of A.A.F. M.C., A.A.R., M.C., M.P.G., and M.D.P. contributed to patient recruitment and data collection. All authors were involved in further drafts of the manuscript and revised it critically for content. All authors approved the final version of the manuscript. The corresponding author attests that all listed authors meet authorship criteria.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was partially supported by grants from SEPAR‐2010‐820, Ministerio de Economía y Competitividad (PI10/00495), Ministerio de Ciencia, Innovación y Universidades (PI19/00875).