
Abstract
Background:
Despite universal coverage of all highly effective contraceptive (HEC) methods in the Military Health System (MHS), active duty service women (ADSW) have higher rates of unintended pregnancy and lower rates of HEC use than the general U.S. population. Between 2016 and 2019, racial minority and lower socioeconomic status (SES) ADSW demonstrated lower odds of HEC use. This study further investigated factors associated with HEC use among ADSW to assess their reproductive health needs.
Methods:
We conducted a cross-sectional study using fiscal year 2020–2023 data from the MHS Data Repository for all ADSW aged 18–45 years. Statistical analyses included descriptive statistics and logistic regression models, adjusted and unadjusted, determining the odds of HEC use overall, by method, and by social characteristics, including race and military rank as a proxy for SES.
Results:
Of the 339,011 ADSW identified, 164,756 (48.6%) used at least one HEC method during the study period. Black (odds ratio [OR] = 0.89; 95% confidence interval [CI] = 0.88–0.91) and Asian/Pacific Islander (OR = 0.88; 95% CI = 0.78–0.82) ADSW demonstrated lower odds of overall HEC use than White ADSW. Junior Enlisted ADSW demonstrated lower odds of overall HEC use than nearly all other ranks.
Conclusions:
The proportion of ADSW using HEC methods has decreased since 2019, while HEC use in the general population has increased. Racial and socioeconomic disparities remain, highlighting the need for future research to investigate reasons for these disparities in order to design effective mitigation strategies to ensure access to contraceptive care for all ADSW.
Background
Despite declining rates of unintended pregnancy over the past decade, nearly half of pregnancies in the United States are unintended, meaning they are either mistimed or unwanted. 1 Racial minorities and young, single women have higher rates of unintended pregnancy, which are correlated with lower rates of effective contraceptive use. 1 –3 Equitable access to the full range of contraceptive options and patient-centered contraceptive counseling are essential for ensuring reproductive autonomy. 4 Studies have shown that access to a preferred method of contraception is associated with more consistent and correct use, which leads to a lower risk of unintended pregnancy. 5 In the general U.S. population, barriers such as cost and access to high-quality care contribute to disparities that racial minorities and women of lower socioeconomic status (SES) experience in using the contraceptive method of their choice. 6,7
Highly effective contraceptive (HEC) methods are those with a failure rate of less than 10%, which includes both short- and long-acting contraceptives. 8 Despite the Military Health System (MHS) offering access to all common forms of prescription contraception at no cost, active duty service women (ADSW) have higher rates of unintended pregnancy than the general U.S. population. 2,3 The MHS is unique within the U.S. health care landscape in that its mission is to promote the health and wellness of servicemembers in order to provide medically ready forces. Unintended pregnancy poses a significant risk to individual and unit readiness. 2 While previous studies have demonstrated successful mitigation of racial disparities for ADSW in the MHS for certain mandatory preventive services, these disparities persist in HEC use despite universal coverage. 9 –11 Black, American Indian/Alaska Native, Asian/Pacific Islander, and Other ADSW have lower odds of HEC use compared with White ADSW. 11
The latest study examining HEC use in ADSW covered Fiscal Years (FY) 2016–2019. 11 The landscape of reproductive health care in the United States has changed since then, with the COVID-19 pandemic limiting access to reproductive health care and the U.S. Supreme Court ruling in the Dobbs v. Jackson Women’s Health Organization case (Dobbs decision) overturning Roe v. Wade. The 2022 Dobbs decision has had an impact on reproductive health care in the U.S. beyond the restriction of abortion services. States with restrictive abortion policies experienced a decline in prescriptions for oral contraceptive pills and emergency contraception. 12 In the MHS, there was an increase in vasectomies received by servicemen in the months following the Dobbs decision. 13 In January 2023, walk-in contraceptive services became available at military hospitals and clinics, making these services more accessible to service members. 14 We anticipate that dynamic changes in access to reproductive health care will continue to manifest as changes in the use of reproductive services. Therefore, we conducted an updated study covering FY 2020–2023 to determine if previously identified disparities in HEC use among ADSW persist in the MHS.
Methods
Using a cross-sectional study design claims data and Defense Enrollment Eligibility Reporting System (DEERS) data from the MHS Data Repository (MDR) were used to identify HEC use among ADSW between FY 2020 and 2023 (October 1, 2019–September 30, 2023). The study population was identified through DEERS and included any ADSW ages 18–45 serving in active duty status in the U.S. Army, Air Force, Space Force, Navy, and Marine Corps. The study population of “women” was determined by sex assigned at birth. Women in the National Guard or Reserves were excluded due to inconsistent access to the MHS. Women over the age of 45 were also excluded, consistent with the larger body of contraceptive literature. 2,6 We were unable to exclude women who were not in need of contraception during the study period, as sexual orientation and sexual activity information are not available in the MDR and prior sterilization was not collected for this study.
The outcome of interest, HEC use, was determined by using the International Classification of Diseases, 10th Revision diagnosis codes, and Current Procedural Terminology codes in the claims data, and filled prescriptions. HEC use was then categorized as a short-acting reversible contraceptive (SARC) use only, long-acting reversible contraceptive (LARC) use only, female sterilization only, and multiple HEC use. SARCs included pills, patches, vaginal rings, and shots/injections. LARCs included implantable rods and intrauterine devices (IUDs). Multiple HEC use was defined as using more than one HEC method within the study period. Demographics, including race, marital status, age (by group), rank, and branch of service, were also analyzed for the study. Since an ADSW could appear in multiple years, they were counted only once in the study period, and their most recent demographics were used. The latest age for each HEC use was retained. For those who did not use any HEC during the study period, the age on their most recent DEERS record was used.
Multivariate binomial logistic regression models were used to calculate the odds for any HEC use, SARC use only, LARC use only, female sterilization only, and multiple HEC use. In order to be able to compare findings across years, the same variables used in the FY 2016–2019 HEC use study were included in our models. 11 These variables were identified a priori in the FY 2016–2019 HEC use study. 11 Each model was adjusted for age group, rank, race, marital status, and branch of service, using the same reference groups as those used in the FY 2016–2019 HEC use study. 11 Statistical significance was set at α < 0.05, and all analyses were performed using SAS, version 9.4. This study was reviewed and determined to be exempt by the institutional review board at the Uniformed Services University of the Health Sciences.
Results
Out of the 339,011 ADSW identified for the study period, 164,756 (48.6%) ADSW used at least one HEC method. Among these, 68,776 (41.7%) used SARC only, 60,132 (36.5%) used LARC only, 2,961 (1.8%) used female sterilization only, and 32,887 (20.0%) used multiple HEC methods (Fig. 1). The largest proportions of ADSW who used a HEC method were ages 20–24, White, married, Junior Enlisted, and serving in the Army (Table 1). Individuals identified as missing data for race and/or rank were excluded from the regression analyses (1,362 [0.4%] and 91 [0.03%] of the total study population, respectively). When stratified by the HEC method, there was a higher proportion of single ADSW using only SARC methods compared with overall HEC users. There was also a higher proportion of Senior Enlisted that used female sterilization only compared with overall HEC users (Table 2).
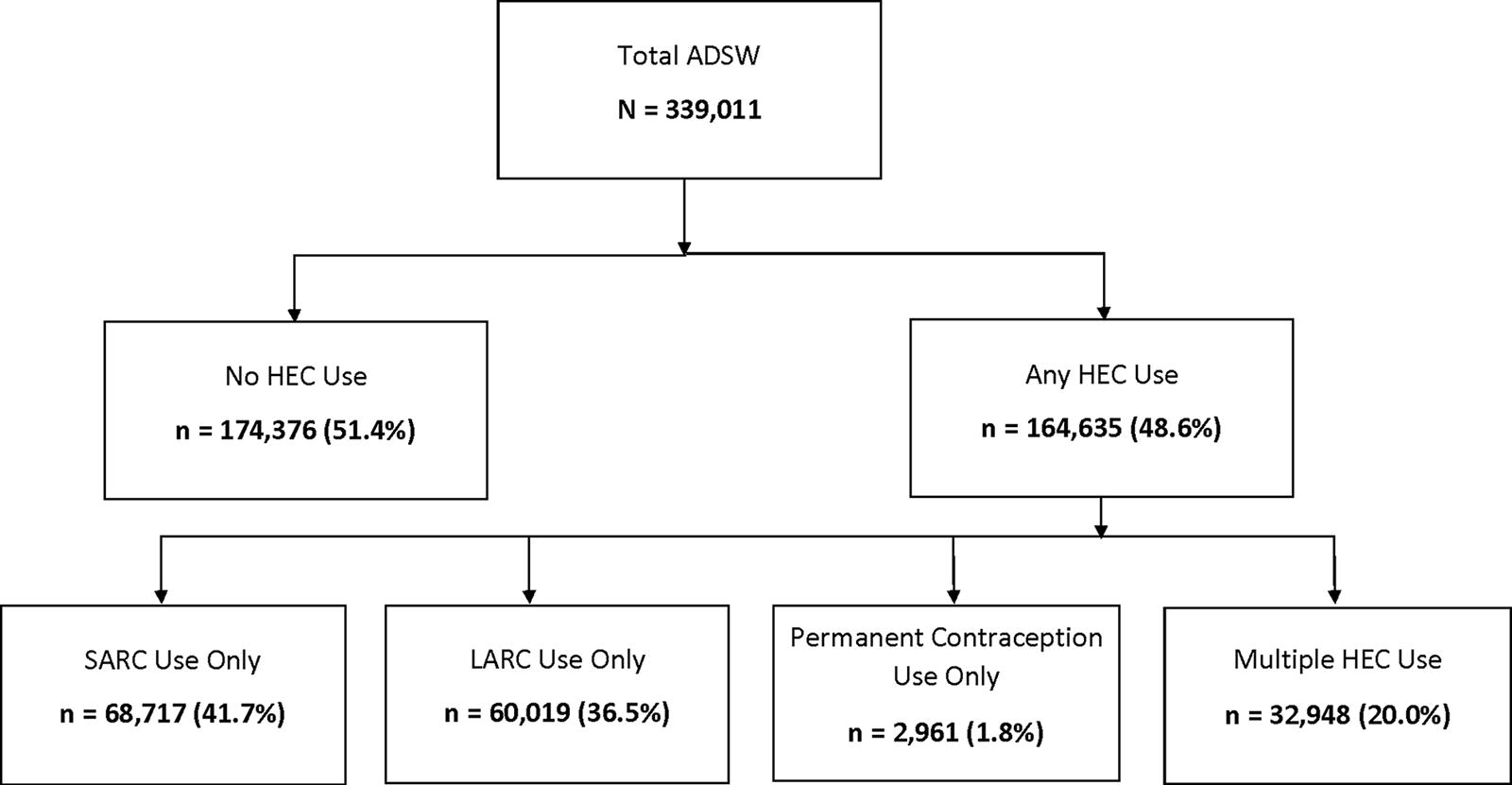
Flowchart of highly effective contraceptive (HEC) use among U.S. active duty service women (ADSW), Fiscal Years 2020–2023. Percentages listed for each contraceptive method are out of ADSW who used any HEC method during the study period. LARC, long-acting reversible contraceptive; SARC, short-acting reversible contraceptive.
Descriptive Statistics of U.S. Active Duty Service Women, Fiscal Years 2020–2023
Values reported as frequencies and percentages: n (%).
Age reported in years.
Definitions: Junior Enlisted—E1–E4; Senior Enlisted—E5–E9; Junior Officers—O1–O4; Senior Officers—O5–O10.
ADSW, active duty service women; HEC, highly effective contraceptive.
Descriptive Statistics of Highly Effective Contraceptive Use Among U.S. Active Duty Service Women, Fiscal Years 2020–2023
Values reported as frequencies and percentages: n (%).
Age reported in years.
Definitions: Junior Enlisted—E1–E4, Senior Enlisted—E5–E9, Junior Officers—O1–O4, Senior Officers—O5–O10.
HEC, highly effective contraceptive; LARC, long-acting reversible contraceptive (implantable rods and intrauterine devices [IUDs]); SARC, short-acting reversible contraceptive (pills, patches, vaginal rings, and shots/injections).
Black (odds ratio [OR] = 0.89; 95% confidence interval [CI] = 0.88–0.91) and Asian/Pacific Islander (OR = 0.88; 95% CI = 0.78–0.82) ADSW demonstrated lower odds of using any HEC method when compared with White ADSW. Married ADSW demonstrated higher odds of using any HEC method when compared with single ADSW (OR = 1.41; 95% CI = 1.39–1.43) (Fig. 2). This was also noted when HEC use was stratified by HEC method for both race and marital status. Almost all the ranks (Senior Enlisted: OR = 2.13; 95% CI = 2.09–2.17, Junior Officer: OR = 2.12; 95% CI = 2.07–2.17, Senior Officer: OR = 2.24; 95% CI = 2.12–2.38, Warrant Officer: OR = 3.08; 95% CI = 2.82–3.37) had higher odds of using any HEC method when compared with Junior Enlisted. However, once stratified by HEC method, Junior Officer ADSW (OR = 0.78; 95% CI = 0.67–0.91) had lower odds of using female sterilization when compared with Junior Enlisted ADSW. ADSW serving in the Air Force/Space Force had higher odds of using any HEC method when compared with ADSW serving in the Army (OR = 1.21; 95% CI = 1.19–1.23) (Table 3).
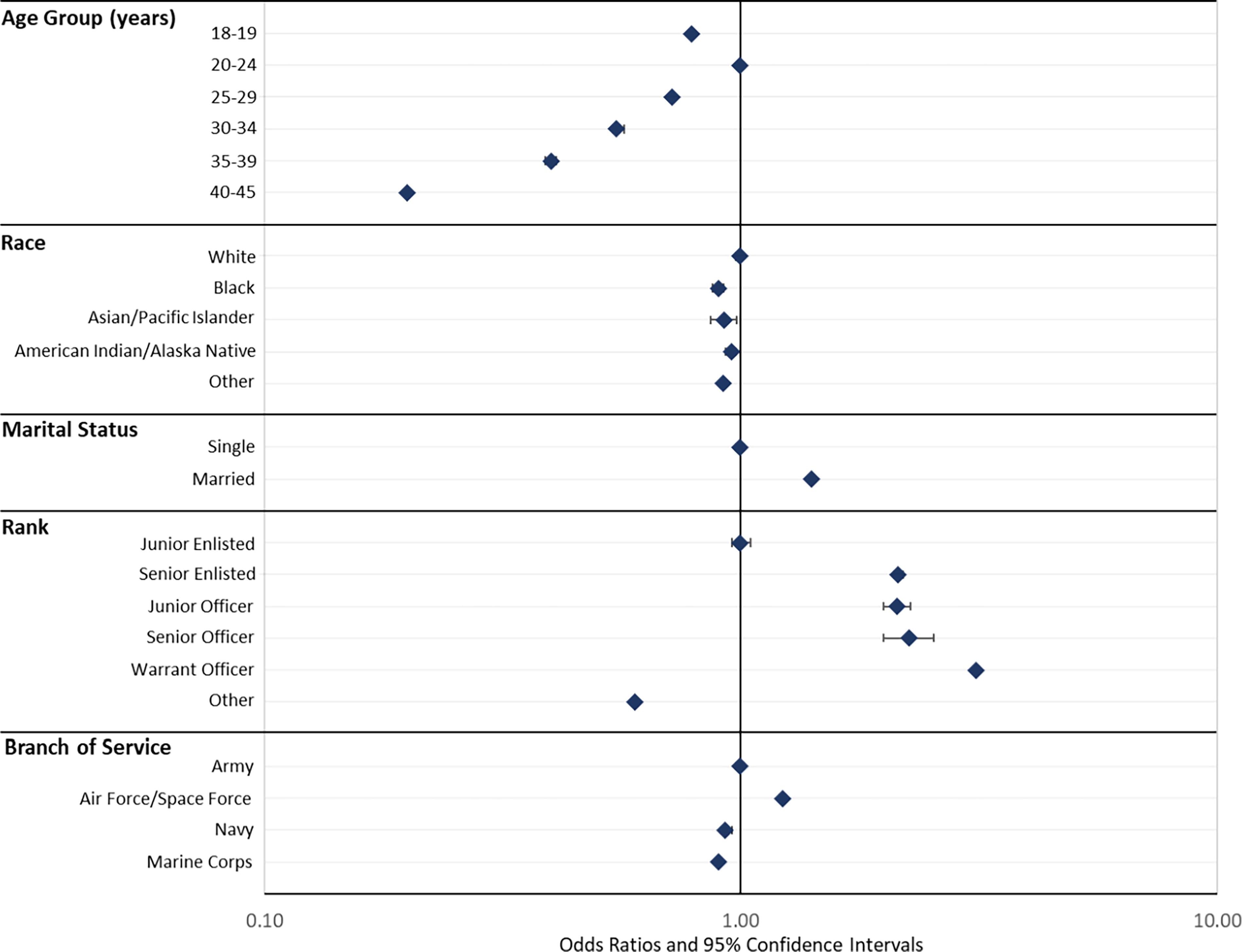
Forest plot of adjusted odds ratios for highly effective contraceptive use among U.S. active duty service women, Fiscal Years 2020–2023. Model reference groups are plotted on the 1.00 odds ratio value line. Diamonds indicate the odds ratio value with bracketed lines indicating the associated 95% confidence interval.
Adjusted Logistic Regression of Highly Effective Contraceptive Use Among U.S. Active Duty Service Women, Fiscal Years 2020–2023 a
Regression model adjusted for age group, race, marital status, rank, and branch of service.
Age reported in years.
Definitions: Junior Enlisted—E1–E4; Senior Enlisted—E5–E9; Junior Officers—O1–O4; Senior Officers—O5–O10.
CI, confidence interval; HEC, highly effective contraceptive; LARC, long-acting reversible contraceptive (implantable rods and intrauterine devices [IUDs]); OR, odds ratio; SARC, short-acting reversible contraceptive (pills, patches, vaginal rings, and shots/ injections).
Discussion
Overall, HEC use among ADSW has decreased since 2019 and disparities persist in terms of race and rank. We found that 48.6% of ADSW aged 18–45 used a HEC method in FY 2020–2023 compared with 59.7% in FY 2016–2019. 11 In contrast, the proportion of women in the general U.S. population aged 20–44 using moderately or most effective contraceptive methods increased from 60.3% between 2015 and 2017 to 62.2% between 2017 and 2019. 15 One of the Healthy People 2030 (HP2030) family planning targets is for 65.1% of women in this age group at risk for unintended pregnancy to use moderately or most effective methods of contraception. 15 The MHS is required to provide health care services in support of force health protection and readiness on both an individual and a population level, necessitating the use of metrics for population-level goals in order to maintain a lethal force while at the same time balancing the needs and preferences of individual ADSW. In the general U.S. population, HEC use in this age group is increasing toward the HP2030 target, while HEC use among ADSW is trending in the opposite direction. This suggests that ADSW may experience different barriers to accessing HEC methods or have different preferences when it comes to their methods of choice than the general U.S. population.
Women are a growing population in the U.S. military, representing 17.5% of active duty service members (ADSMs) in 2022 and have been able to serve in all occupational specialties since 1 January 2016. 16 As the proportion of ADSMs who are women continues to rise, so does the population at risk for unintended pregnancy as the vast majority of ADSW are of childbearing age. 16 Unintended pregnancy is associated with negative impacts on maternal and child health, and among service members can affect individual medical readiness and can limit their ability to fully participate in their military career. 17 Unintended pregnancy during deployment can result in delayed prenatal care, medical evacuation, and career repercussions. 18,19 Previous studies have shown that many ADSW preferred LARC methods while deployed not only because of the reliability of these methods for pregnancy prevention but also for ease of use and a desire for menstrual suppression. 19 However, limited access to contraceptive care during deployment can create a barrier to ADSW being able to use the method of their choice. 18,19 Therefore, contraceptive care remains a critical focus for military health care.
Logistical barriers remain in the MHS when it comes to accessing reproductive health care: patients have reported difficulty scheduling appointments, inability to take time off to attend appointments, and delays in receiving the contraceptive method of their choice. 20 The 2023 introduction of walk-in contraceptive clinics was intended to increase access to reproductive health care in the MHS; however, this change is so recent that its effects have not yet been documented in the literature. Future research is needed to investigate the impact of walk-in contraceptive clinics on these barriers to accessing reproductive health care in the MHS.
In addition, recent studies have shown that the 2022 Dobbs decision has impacted patients’ contraceptive choices in both the military and civilian health systems, particularly in states with more restrictive post-Dobbs abortion laws. 21 In states with the most restrictive post-Dobbs abortion laws, access to contraception was limited by the closure of a large number of family planning clinics. Texas saw a 28% decline in fills for oral contraceptive pill prescriptions in the year after Dobbs. 12 An estimated 80,000 ADSW live and serve in states where abortion was banned post-Dobbs. 22 While the ruling does not affect the availability of contraceptive services in the MHS, recent studies have shown changes in service members’ contraceptive choices in states with restrictive abortion laws post-Dobbs. In the MHS, vasectomy incidence increased post-Dobbs, particularly among young, unmarried men, and the increase was greater in Texas, where abortion was banned post-Dobbs, than in Virginia, where it was not. 13 Further research is needed into the impact of Dobbs on the reproductive health care of ADSW.
In the general U.S. population, Black women have a higher rate of unintended pregnancy and a lower rate of contraceptive use than White women. 1 Similarly, in our study, Black and Asian/Pacific Islander ADSW had lower odds of overall HEC use than White ADSW. These disparities were also noted in a previous study examining HEC use among ADSW during FY 2016–2019. 11 Previous studies have demonstrated successful mitigation of racial disparities for preventive services (cervical cancer screening and mammography screening) in the MHS. 9,10 However, these preventive services are mandatory readiness requirements for ADSW in the MHS, while contraceptive use is a preference-sensitive decision made by the individual ADSW based on her needs and desires. The persistence of racial disparities in HEC use among ADSW highlights the need to investigate preference and other factors beyond cost and coverage contributing to lower HEC use in racial minorities.
Studies suggest that implicit biases continue in reproductive health care in the United States, with racial minority women and women with a lower SES being recommended LARCs more often than White and middle-class women. 23,24 Awareness of these biases and of historical racial injustices in reproductive health care can contribute to Black and Hispanic women’s lower rates of contraceptive use. 24 Previous studies have shown that many racial minority women prefer not to use methods that are provider-controlled, such as LARCs, which require insertion by a provider. 25,26 In our study, all racial minority groups had higher odds than White women of using SARCs, which are typically considered less effective methods of contraception than LARCs but are generally user-controlled. Further research should investigate contraceptive preferences and reasons for nonuse among ADSW in order to determine the extent to which preference contributes to the difference in HEC use between White and racial minority ADSW.
Lower-income women have higher rates of unintended pregnancy rates compared with higher-income women in the general U.S. population. 27,28 Cost is a major barrier to accessing the contraceptive method of their choice. The 2015–2017 National Survey of Family Growth found that 22% of women at risk for unintended pregnancy would prefer to use a different contraceptive method, and 39% of nonusers would start using a method if cost were not a factor. 29,30 We use rank as a proxy for SES, with Junior Enlisted being considered the lowest SES group. Young, Junior Enlisted ADSW experience the highest rates of unintended pregnancy, and in this study, as in the FY 2016–2019 study, Junior Enlisted had the lowest rates of HEC use. 11,17 This finding mirrors that of the general U.S. population despite universal coverage at no cost. Further research is needed into pregnancy desires and intentions as well as contraceptive preferences and barriers to use in this subgroup of ADSW.
Optimal contraceptive care enables reproductive autonomy, giving women the power to make and act on decisions about contraception, pregnancy, and childbearing.
4,31
Best practices include patient-shared decision-making and access to culturally appropriate education regarding their contraceptive options.
4,32
Increasing contraceptive education and access during basic training has been demonstrated to increase the uptake of contraception among young, Enlisted ADSW, indicating that there is an unmet need for contraception in this population. However, a previous study noted that only a quarter of ADSW received any contraceptive counseling, and even fewer received counseling prior to deployment.
3,20
A previous study found that differences in contraceptive education and access policy at entry-level training were associated with differences in rates of contraceptive use by service branch.
8
While there are more similarities across branches since the transition to the
Limitations
This study only reflects contraception provided by the MHS, and therefore may not capture all ADSW that are using HEC methods. Data on sexual activity or sexual partners were not reported, so we were not able to exclude ADSW who were not sexually active, had a partner who had received a vasectomy, or had a same-sex partner during the study period and were therefore not at risk for unintended pregnancy. We did not exclude ADSW who had had a sterilization procedure prior to the start of the study period in order to keep our exclusion criteria consistent with the previous study for comparison purposes. 11 Data pertaining to the duration of use of a specific HEC method, contraceptive adherence, discontinuation, or failure were not reported. For individuals identified as using multiple HEC methods during the study period, it was not reported whether they were using them simultaneously or consecutively. The dataset did not include qualitative information, so we were not able to determine reasons for contraceptive use or nonuse.
Conclusions
Despite universal coverage of all HEC contraceptive methods at no cost in the MHS, HEC use among ADSW has declined since 2019 and racial and socioeconomic disparities persist. This study highlights that further efforts are needed to identify barriers to the use of family planning services in the MHS, particularly among racial minorities and low-SES ADSW. Future research should include qualitative data describing the experiences, beliefs, and intentions of ADSW concerning contraceptive use and family planning services in order to develop appropriate interventions to reduce disparities.
Footnotes
Acknowledgments
The authors express gratitude to Amanda Banaag for serving as a consultant and quality reviewer on the data analysis for this study.
Authors’ Contributions
A.K.: Writing—original draft, writing—review and editing, interpretation of findings. S.S.M.: Data curation, interpretation of findings, formal analysis, visualization. H.M.B.: Conceptualization, methodological development, writing—review and editing. C.C.: Conceptualization, interpretation of findings, project administration, supervision, writing—review and editing. T.P.K.: Conceptualization, supervision, data acquisition, methodological development, interpretation of findings, funding acquisition, writing—review and editing. All authors contributed to the writing and/or editing of the article and have reviewed the final version prior to submission.
Ethics Approval
This study was found exempt from human subjects review by the institutional review board of the Uniformed Services University of the Health Sciences.
Consent for Publication
Institutional clearance was obtained.
Data Sharing
The data that support the findings of this study are available from the United States Defense Health Agency. Restrictions apply to the availability of these data, which were used under federal data user agreements for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of the Defense Health Agency.
Disclaimer
The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, assertions, opinions, or policies of the Uniformed Services University of the Health Sciences (USUHS), the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF), the DOD, or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
This study was funded by the Department of Defense, Defense Health Agency, award #HU00012120089. The funding agency played no role in the design, analysis, or interpretation of findings.