
Abstract
Background:
Hepatitis C virus (HCV) infection affects between 1% and 2.5% of pregnant people in the United States and has maternal and fetal sequelae. Direct-acting antivirals are a highly effective curative strategy for HCV, yet data on their use in pregnancy are limited. Thus, family planning counseling of pregnancy-capable people seeking treatment for HCV is imperative. We aimed to examine whether and how pregnancy-capable people with HCV received family planning counseling from their clinicians during their treatment of HCV.
Methods:
This retrospective cohort study included all female patients between 18 and 50 years of age with HCV who sought care at a large, multihospital medical system between 2016 and 2020. Outcomes included whether patients who sought care for HCV received family planning or preconception counseling and the type of counseling they received. Analysis was conducted using descriptive statistics.
Results:
In this analysis of 194 people meeting inclusion criteria, 146 sought treatment for HCV, of whom 16 were currently pregnant. Of those seeking treatment, 24% discussed the uncertainty of treatment safety during pregnancy with their clinician, 23% received contraceptive counseling, 7% received preconception counseling, and 10% discussed family planning goals. Of the participants who were pregnant, 74% discussed the risks of treatment during pregnancy, and 67% had a postpartum treatment plan.
Conclusions:
In this cohort of pregnancy-capable people with HCV, patients infrequently received counseling about reproductive planning before or during their HCV treatment. Although most patients who were pregnant received counseling on treatment recommendations, few were referred to maternal–fetal medicine subspecialists.
Introduction
Hepatitis C virus (HCV) infection, which affects between 1% and 2.5% of pregnant people in the United States, can result in both maternal and fetal consequences. 1 In the antepartum period, people with HCV have a greater risk of gestational diabetes and intrahepatic cholestasis of pregnancy. 2,3 In the postpartum period, they may experience acceleration of liver fibrosis and disease progression. 4 Infants born to mothers with HCV viremia have higher rates of small-for-gestational-age birth, neonatal intensive care unit admission, and a 5–15% risk of perinatal acquisition of HCV. 5,6
In 2011, direct-acting antivirals (DAAs) were initially approved for use in the United States and now feature two primary regimens that treat all known genotypes of HCV. DAAs are highly effective, with cure rates approaching 100%. 7 Pregnant individuals have been largely excluded from investigations on the use of DAAs for treatment of HCV. 8 Although studies are ongoing to investigate their safety in pregnancy and early reports suggest they are likely safe and well-tolerated, 9 the use of DAAs during pregnancy remains limited. Current guidelines regarding treatment during pregnancy advise shared decision-making about undertaking or continuing DAA treatment during pregnancy, 10 and experts in perinatal HCV have called for expansion of treatment programs, with close attention to patient and clinician education. 8
Given the potential perinatal and long-term consequences of HCV during pregnancy, as well as limited data and nuanced guidelines regarding treatment during pregnancy, counseling pregnancy-capable individuals with HCV about family planning is imperative. As with all individuals with a chronic disease, comprehensive family planning care includes both provision of effective contraception for those who desire it, as well as discussion of preconception care, referral to experts (e.g., maternal–fetal medicine) when indicated, optimization of chronic disease status prior to pregnancy, review of pregnancy risks and timing, and discussion of options for timing of treatment with regard to pregnancy plans. 11,12,13,14
Despite the importance of family planning care, little is known about this type of care among individuals with HCV. Our team’s prior qualitative work exploring barriers to HCV treatment during pregnancy identified that few people had discussions about pregnancy planning prior to undertaking treatment. 15 Given limited data on this topic, the importance of patient-centered care regarding HCV treatment, and our prior qualitative findings, we designed the present study to more fully evaluate the receipt of counseling about contraception, preconception care, and other aspects of family planning among pregnancy-capable individuals with HCV. We also aimed to study the rates of pregnancy-specific counseling and referrals for patients who were pregnant at the time of diagnosis of HCV or during discussion of treatment options. We hypothesized that the minority of pregnancy-capable individuals with HCV seeking HCV care received adequate counseling about reproductive life planning.
Materials and Methods
This is a retrospective cohort study conducted in a large, Midwestern, multihospital medical system that includes nine hospitals (including one large academic tertiary care center, one community tertiary care center, and seven affiliated community hospitals) and their affiliated ambulatory practices. Ambulatory services for people with HCV in this system include access to adult and pediatric infectious disease, maternal–fetal medicine, hepatology, and psychiatrists. A Women’s Infectious Disease Program, housed at the academic tertiary care center, provides joint infectious disease (adult and pediatric) and maternal–fetal medicine care to pregnant or preconception individuals with HCV, HIV, and other infectious diseases.
Those eligible for this analysis included female patients with HCV who were seen for any type of health care interaction within this health care system from May 2016 to May 2020. The eligibility period ended in 2020 due to the interruptions in health care that occurred with the COVID-19 pandemic, but chart abstraction occurred through 2023. Patients who were eligible for inclusion had their medical records reviewed for any HCV treatment-related encounters through December 2023. The institution’s electronic data warehouse was used to identify females between 18 and 50 years of age with HCV based on an antibody test or clinical diagnosis at any time in their electronic medical record, regardless of viral load, who had any interaction in the health care system (including emergency department, obstetric care, or outpatient specialty or primary care services). HCV diagnosis was made based on laboratory studies available in each patient’s chart that demonstrated a positive HCV antibody result and subsequent follow-up testing (viral load and/or viral genotyping). The age range included individuals up to age 50 given the rising age of pregnancy in the United States, 16,17 as well as the need to provide effective contraception until confirmation of menopause for all individuals who do not desire pregnancy. 18 The electronic medical records of these patients were then reviewed to identify documented aspects of clinical care and counseling. After identifying all patients with any laboratory test qualifying for a diagnosis of HCV, HCV-related encounters were identified by manually searching through the chart to find appointments, emergency department visits, or admissions during which the patient’s diagnosis of HCV was documented. No standardized system-wide protocol for the reproductive health care of these patients was in existence at the time of these encounters.
Data collection included the sociodemographic and clinical characteristics of the included participants (including pregnancy status), as well as HCV treatment history and viral loads. Outcomes of interest included information on whether those participants who sought treatment for HCV received counseling on the risks or uncertainty of treatment during pregnancy, preconception counseling, contraception counseling, and family planning goals (including if and when patients desired to conceive). Information about who performed counseling (both specialty and clinician type) additionally was collected. The data were collected by two reviewers based on a shared manual of definitions. For this analysis, we made an a priori decision to focus on whether counseling discussions regarding contraception and family planning had been documented for participants when they sought counseling about or initiated HCV treatment, as our goal was to evaluate whether reproductive life planning was assessed in the context of decision-making about HCV treatment. Patients were determined to have sought out treatment based on their presence at an encounter where treatment for HCV was discussed with a medical provider; they were not required to have initiated or completed treatment in order to be included in this cohort. The care pathways for those who did not seek HCV treatment were described, but as most of these encounters occurred in the emergency department or other nonambulatory settings where treatment about HCV was not discussed, the receipt of family planning counseling was not reported for those individuals. For patients who were pregnant at the time of their first HCV-related interaction with this health care system, outcomes that were assessed included whether discussions of treatment for HCV, recommendations for postpartum contraception, and referrals to maternal–fetal medicine specialists were documented.
Data were summarized using frequencies and counts for categorical variables, and medians with interquartile ranges for continuous variables. Sociodemographic and clinical characteristics were stratified based on whether participants sought treatment for HCV. Among those who sought treatment, the proportions who had documented counseling and referrals for the above outcomes were reported. The proportions of patients with documented referrals and counseling were also examined in the subset of people who were pregnant at the time of their initial HCV-related appointment. All descriptive statistics were conducted in R version 4.1.2. 19 As this was an exploratory, descriptive study of all available individuals in the study period, significance testing and a power analysis were not performed.
This study was approved by the institutional review board of Northwestern University.
Results
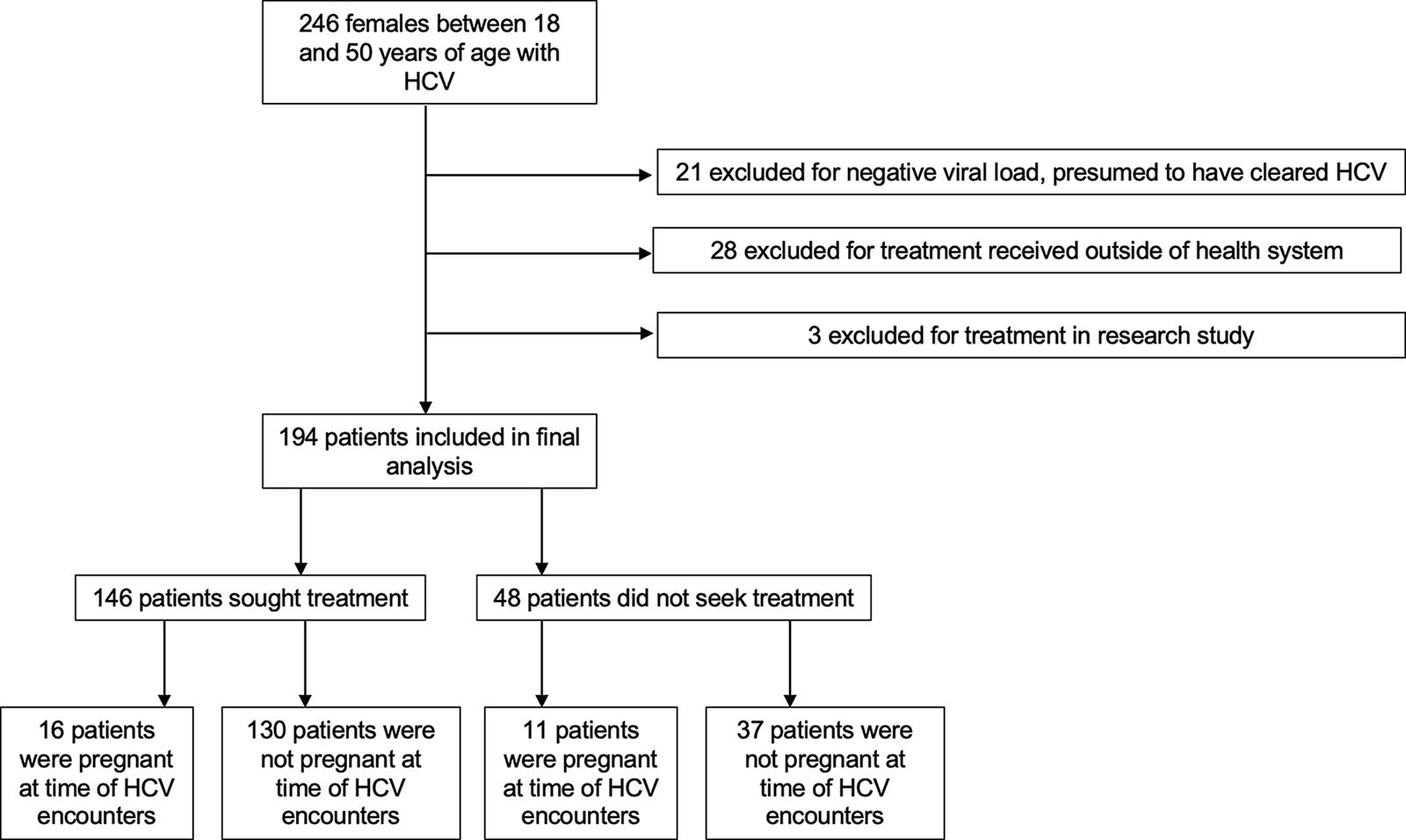
During this time period, 246 female individuals with documented HCV based on a positive HCV-antibody test received health care in this hospital system. Of those, 21 were HCV-antibody positive with a negative viral load (due to either self-resolution of HCV or prior successful treatment) and thus did not meet criteria for treatment; 28 were treated outside of the health system and their treatment plans, counseling, and viral loads could not be reviewed; and 3 were treated as part of a research study and information on their lab values and treatment course was not available. Therefore, 194 patients with a positive HCV-antibody test and positive viral load were included in the final analysis. Of these, 146 participants sought treatment, and 48 did not have documented encounters that discussed treatment for HCV. In the total cohort of 194 individuals, 27 participants were pregnant at the time of their HCV-related encounters, and of those, 16 sought treatment (Fig. 1).
Study participants.
The median age of all participants included in the study was 33 years. Out of all included participants, 41% had commercial insurance; 90% of those with commercial insurance sought HCV treatment. For participants who sought treatment, patients reported the most common mode of HCV acquisition was unknown (38%), followed by intravenous drug use (23%) and perinatal acquisition (17%). For those who did not seek treatment, the most common mode of patient-reported HCV acquisition was intravenous drug use (52%), followed by unknown mode of acquisition (38%) and blood transfusion (6%) (Table 1).
Sociodemographic Characteristics of Pregnancy-Capable Individuals Who Did and Did Not Seek Treatment for Hepatitis C Virus
N (%).
IQR, interquartile range.
Most participants included in the study had a history of a prior pregnancy, with a median number of live births of 1 in the group that sought treatment versus 2 in the group that did not seek treatment. A minority were pregnant at their first HCV-related encounter (11% among those who sought treatment versus 23% among those who did not seek treatment). Seventy-five percent of participants who did not seek treatment had substance use diagnoses and 48% had mental health diagnoses versus a respective 32% and 29% of those participants who sought treatment (Table 2).
Clinical Characteristics of Pregnancy-Capable Individuals Who Did and Did Not Seek Treatment for Hepatitis C Virus
Data displayed as N (%) or median (interquartile range [IQR]).
Not including HCV or HIV.
Unknown values: four participants who sought treatment, one participant who did not seek treatment.
Unknown values: three participants who sought treatment, one participant who did not seek treatment.
Unknown values: zero participant who sought treatment, one participant who did not seek treatment.
Unknown values: one participant who sought treatment, three participants who did not seek treatment.
Unknown values: 27 participants who sought treatment, 43 participants who did not seek treatment.
BMI, body mass index; HCV, hepatitis C virus.
Of the patients who sought treatment with a hepatologist, infectious disease clinician, or obstetrician/gynecologist, 24% had documentation of a discussion with their clinician about the risk or uncertainty of treatment during pregnancy, 7% had documentation of preconception counseling or a referral, 23% had documented discussions that included information about the need for contraception use during HCV treatment, 14% were offered or recommended a specific form of contraception, and 10% included a documented discussion about family planning goals (Table 3). After stratification by the type of provider, 100% (n = 2) of patients who were counseled by an obstetrician/gynecologist during their HCV-related encounters had documentation of counseling on the need for contraception during treatment course versus 27% (n = 28/102) of those who received treatment counseling from a hepatologist, 21% (n = 3/14) from an infectious disease specialist, and 15% (n = 4/26) from a general gastroenterologist. The majority (88%) of patients who were counseled about treatment subsequently initiated treatment with DAAs, with 89% achieving a sustained virological response (Table 3).
Family Planning and Preconception Counseling Among Reproductive Age People Who Sought Treatment for Hepatitis C Virus
Data displayed as N (%) or median (interquartile range [IQR]).
DAAs, direct-acting antivirals.
In this cohort, 27 individuals were pregnant at the time of their HCV-related encounter, none of whom initiated treatment during their pregnancy. Most (74%) had a documented discussion with their clinician (infectious disease specialists, obstetricians, hepatologists, or general gastroenterologists) about the risks and uncertainties of treatment during pregnancy. Only 48% of pregnant participants were referred to a maternal–fetal medicine subspecialist for care as documented by referrals placed by primary providers and by visits with subspecialists within the electronic health record, and only 30% had a documented discussion with their clinician regarding the recommendation for postpartum contraception during treatment with DAAs. Most (67%) had a documented plan for treatment after pregnancy and breastfeeding were completed (Table 4). Thirty-three percent subsequently returned to their providers after delivery for postpartum treatment and achieved a sustained virologic response. The remainder had no documentation of further treatment available in their patient charts.
Counseling and Management of Pregnant Patients with HCV
Data displayed as N (%).
HCV, hepatitis C virus.
Discussion
We identified that a minority of nonpregnant individuals with HCV received comprehensive counseling about reproductive life planning when being counseled about or initiating their treatment for HCV. Furthermore, among pregnant individuals, although a majority received counseling about HCV treatment during pregnancy, a minority received referrals to specialized obstetric care for their more individualized counseling during their antenatal care, and a minority received appropriate postpartum counseling and treatment. In this study, the suboptimal performance of counseling on contraception and family planning demonstrates the gap in care that exists for pregnancy-capable individuals seeking care for HCV. This finding is particularly important for patients who have difficulty accessing health care services or attending outpatient appointments, as these health care interactions may be critical time points in which patients are able to engage in their care.
Although the treatment of HCV during pregnancy remains an area of rapid expansion in research, respect for patient autonomy necessitates shared decision-making between clinicians and pregnancy-capable individuals with HCV regarding family planning and the use of contraception. 20 Patients should be informed of current evidence-based practices regarding HCV treatment and empowered to discuss treatment planning and timelines in relation to their reproductive lives, particularly because treatment is often deferred or refused if a patient were to become pregnant.
Current studies are underway to evaluate the effects of DAAs during pregnancy and breastfeeding, 9,21,22 which may ultimately lead to changes in guidelines for treatment in this patient population. At this time, clinicians should discuss the growing but currently limited evidence for treatment during pregnancy, as well as review and provide effective methods of contraception if DAA use is desired by the patient. However, this study demonstrates that physicians are not typically counseling their pregnancy-capable patients on the utilization of effective forms of contraception during treatment of HCV. Even for clinicians who recommended the use of contraception while taking a DAA, few documented that a method of contraception was offered or that a referral to a gynecologist or primary care provider was made for further contraception care. Importantly, most clinicians who initiate treatment of DAAs are nonobstetricians/gynecologists. When an obstetrician/gynecologist was performing counseling about HCV, documentation on contraception counseling was typically included, although it should be recognized that the number of patients was small in this group. This finding regarding clinical care provision highlights that all clinicians should participate in shared decision-making with their patients about their family planning desires, provide patients with referrals, or participate in multidisciplinary discussions with their colleagues to ensure that patients are being properly cared for and counseled.
It is increasingly acknowledged that the inclusion of pregnant and postpartum people in HCV treatment planning will be necessary to achieve HCV eradication goals globally. Patients who are diagnosed with or seek care for HCV during their pregnancy benefit from receiving the most updated guidance on management of their condition during and after pregnancy. In addition, postpartum contraception is a mechanism to prevent a short-interval pregnancy, 23 and discussions about its initiation after birth may provide patients who desire to postpone treatment of HCV to the postpartum period time to optimize their disease status before a subsequent planned conception. Thus, for pregnant individuals presenting for care for HCV, counseling about not only pregnancy considerations (i.e., whether to undertake treatment during pregnancy and the potential risks and benefits) but also postpartum family planning should be key elements of HCV care.
A strength of this analysis is that scant literature has evaluated the intersections of health care between HCV and family planning needs. This evaluation from a large, diverse health care system identified areas for potential interventions and quality improvement initiatives. However, there are limitations to note. This study is a retrospective cohort study that is limited by the available clinical documentation; data are limited to documented discussions included in clinicians’ notes and may not capture every discussion that took place during HCV-related encounters if, for example, clinicians used standard note templates without including edits to their documentation about further counseling discussions.
Similar studies have been conducted on risk management discussions and contraception counseling with the use of teratogenic drugs such as isotretinoin, which is used to treat acne but can have teratogenic effects. 24 Even when counseling is mandated, studies demonstrate wide discrepancies on contraception counseling (6.1–98%) and use during treatment (1.7 − 100%). 25 In a study that specifically assessed primary care physicians’ comfort with identifying medications with potential teratogenic effects and contraceptive counseling in these instances, only 58.4% of physicians correctly identified category D or X medications, and most of the surveyed physicians reported that their training was insufficient in preparing them to counsel patients on contraceptive methods. 26 Although DAA medications are not thought to be teratogenic, these data nonetheless suggest that family planning counseling in the context of chronic disease treatment varies widely and that further work is needed to expand provider comfort with these topics.
Recent updates in HCV testing guidelines demonstrate an increased awareness for the need to properly treat HCV. The Centers for Disease Control and Prevention (CDC) and the U.S. Preventive Services Task Force revised their guidelines in 2020 to include recommend universal HCV screening for pregnant people; subsequently, the American College of Obstetricians and Gynecologists released updated guidelines that follow suit in 2023. 27 –29 In 2023, the CDC released a new set of guidelines recommending testing for HCV for all perinatally exposed infants at ages 2 and 6 months. 30 In addition, the option for treatment with DAAs during pregnancy is increasingly considered by patients and clinicians alike, as supported by the American Association for the Study of Liver Diseases guidelines that emphasize shared decision-making. 10
Conclusions
Given the rapid advancement of options for people with HCV, full consideration of reproductive life planning in the context of HCV treatment and the current state of knowledge regarding DAAs during pregnancy should be an essential component of whole-person care. Further initiatives to educate and empower clinicians to engage in shared decision-making discussions with their patients regarding family planning and reproductive health during treatment for HCV should be included in the broader efforts toward viral hepatitis elimination.
Footnotes
Authors’ Contributions
Data collection was performed by D.M. and E.L. Statistical analysis was performed by N.L. All authors assisted in the authorship and editing of this article. Funding acquisition was obtained by W.A.G., R.J., and L.M.Y.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
R.J. reports personal fees from AstraZeneca, personal fees from Seqirus, personal fees from Dynavax, personal fees from Sanofi, personal fees from Pediatric Infectious Diseases Society, grants from GSK, and personal fees from Gilead, outside the submitted work. D.M., E.L., N.L., W.A.G., and L.M.Y. disclose no conflicts of interest. Data are not publicly available, but interested parties with appropriate oversight may contact the authors for data access.
Funding Information
Research reported in this publication was supported, in part, by the National Institutes of Health’s National Center for Advancing Translational Sciences (UL1TR001422), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (3UG1 HD040512-20S1), and the CDC 200-2022-15052 (75D30122C15052).