
Abstract
Background:
Tele-mental health services have the potential to reduce barriers to postpartum mental health care, particularly for Medicaid-insured individuals who face geographic and logistical challenges. In January 2019, Massachusetts Medicaid became one of the few states to implement payment parity for tele-mental health services before the COVID-19 pandemic, ensuring equal coverage for tele-mental health and in-person visits. This policy change provides a unique opportunity to evaluate whether payment parity improves postpartum mental health service utilization. This study aimed to estimate the impact of Massachusetts Medicaid’s coverage of tele-mental health services at parity with in-person visits on postpartum mental health service utilization among Medicaid-insured birthing individuals.
Methods:
A difference-in-differences (DD) analysis using the Massachusetts All-Payer Claims Database from January 1, 2016, to March 10, 2020. This study compared Medicaid and privately insured individuals before and after Massachusetts implemented tele-mental health payment parity in January 2019.
Results:
Among the 138,669 individuals in the sample, 81,494 were covered by Medicaid, and 57,175 were privately insured. Postpartum tele-mental health use was minimal across the sample (0.07%). The adjusted DD analysis indicated no statistically significant increase in tele-mental health utilization among Medicaid enrollees compared to privately insured individuals (adjusted difference: 0.08 percentage points; 95% CI: −0.02 to 0.17).
Conclusion:
The implementation of tele-mental health payment parity did not significantly increase tele-mental health utilization among Medicaid-insured birthing individuals in Massachusetts. Despite policy changes, systemic barriers likely limited the uptake of tele-mental health services, highlighting the need for additional interventions to improve access to postpartum mental health care.
Introduction
Birthing people during the postpartum period are notably vulnerable to the onset or exacerbation of mental health conditions. These conditions, including depression, anxiety disorders, and psychosis, affect one in five birthing individuals. 1,2 These disorders profoundly affect physical health, the maternal-infant relationship, and infant development. 3 –6 However, these conditions remain substantially underdiagnosed and untreated. 7,8 Lack of treatment can lead to an increased risk of severe health outcomes, including psychiatric emergencies requiring hospitalization, alcohol and drug use, social relationship problems, and persistent depression. 9 –11 Given the large population affected by postpartum mental health conditions and the severity of negative impacts, there is an urgent need for enhanced access to treatment.
There are multiple barriers to receiving adequate mental health care during the postpartum period, including insufficient insurance coverage, inefficient care delivery systems, and workforce maldistribution. 12 During this time, birthing individuals often have fewer interactions with health care providers and may not receive adequate mental health support. 13,14 Recognizing these challenges, several medical authorities and professional organizations like the American College of Obstetricians and Gynecologists and the US Preventive Services Task Force have developed guidelines aimed at improving the screening and referral processes for mental illness in this population. 15 –17 These efforts are a step toward mitigating the effects of perinatal mental conditions, particularly for those at increased risk, such as low-income birthing people covered by Medicaid and those from minoritized racial and ethnic groups.
Treatment strategies for many mental health disorders—including depression and anxiety, the most common disorders in the postpartum period—include psychotherapy and/or medication (e.g., antidepressants) as first-line treatment. 18 Although obstetric or primary care clinicians may prescribe or manage medications during pregnancy and the immediate postpartum period, birthing people often need access to mental health specialty care to receive adequate care including psychotherapy and/or ongoing medication management. 19,20 This need for specialized care highlights a significant gap in the continuum of care for this vulnerable population.
Telehealth has emerged as an important delivery method in overcoming geographical and logistical barriers. By facilitating remote consultations, telehealth may address transportation and geographic barriers to specialists. 21 In the context of mental health care, tele-mental health can also help mitigate privacy concerns and stigma, 22 which may be particularly pronounced during the perinatal period. 23,24 However, access barriers remain, including insurance coverage of telehealth, internet connectivity issues, and disparities in digital literacy. The COVID-19 pandemic has accelerated the adoption of telehealth, suggesting its potential to improve health care delivery by offering an alternative to in-person visits.
In January 2019, the Massachusetts Medicaid program became one of the few states to implement parity for tele-mental health coverage with in-person visits prior to the COVID-19 pandemic. 25 This policy aimed to improve access to essential mental health services, including those needed during the postpartum period. During the COVID-19 pandemic, most states expanded their Medicaid coverage of telehealth for mental health services (“tele-mental health”). While many state policies were designated as temporary, several states have continued to cover telehealth services beyond the expiration of emergency declarations. 26
In this study, we estimate the effect of Massachusetts Medicaid’s coverage and reimbursement of tele-mental health services, provided at parity with in-person visits, on the receipt of postpartum mental health services. The evidence from our analysis of Medicaid coverage of tele-mental health services prior to the pandemic provides insights into the outcomes of payment policy without significant implementation support. This may be informative in the development of policy in other state Medicaid programs that aim to improve access to mental health services, particularly for perinatal populations at high risk of adverse outcomes.
Methods
Data and sample
We used the Massachusetts All-Payer Claims Database (MA APCD, versions 8 and 10), which includes medical claims and health insurance enrollment information for Medicaid, Marketplace plans, and most private insurers in the state. In the database we used, diagnoses and procedure codes related to substance use disorder were redacted. We identified individuals who had a live birth from January 1, 2016, to December 11, 2019, using International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes and Current Procedure Terminology (CPT) Codes. 27 We used this end date so that each individual’s 3-month postpartum observation period ends by March 10, 2020, when Massachusetts declared a state of emergency in response to COVID-19. This period enables us to eliminate any potential confounding effects the pandemic had on health care utilization patterns among birthing individuals. We limited our analysis to individuals aged 18–44 years at delivery who resided in Massachusetts and were continuously insured by a reporting plan from delivery through 3 months postpartum. Finally, we restricted the sample to those who were continuously insured by either Medicaid or private insurance from the month of delivery through 3 months postpartum, ensuring that they did not switch insurance types during this period. 28
Measures
Our primary outcome of interest was a binary measure of any tele-mental health use in the 3 months postpartum. Tele-mental health use was identified using CPT codes, Healthcare Common Procedure Coding System (HCPCS), modifiers, and place of service (POS) codes that indicated telehealth services (Supplementary Table S1) with a principal ICD-9/ICD-10 diagnosis of any mental illness (Supplementary Table S2). We examined two additional outcome measures: binary measures of (1) any outpatient mental health visits and (2) any telehealth use (Supplementary Table S3) within 3 months postpartum. We used an inclusive measure of outpatient mental health services visits, identified using CPT codes, HCPCS codes, revenue codes, and POS codes (Supplementary Table S4) with a principal ICD-9/ICD-10 diagnosis of any mental illness (Supplementary Table S2).
We accounted for covariates recognized in existing literature as risk factors for postpartum mental illness. 29,30 These factors included diabetes, hypertensive disorders of pregnancy, and prenatal mental illness. Additionally, we included two indicators of socioeconomic status based on the patient’s 5-digit ZIP code of residence: whether individuals resided in an area where the median household income was within the lowest quartile 31 and whether they lived in an area of concentrated poverty, defined as having a poverty rate exceeding 30%. 32 Finally, we also included maternal age (categorical) and delivery mode (cesarean vs. vaginal).
Empirical analysis
We performed descriptive analysis and used chi-squared tests to make statistical comparisons between individuals covered by private insurance and those covered by Medicaid. Our empirical analysis employed a difference-in-differences (DD) design. This approach compared outcomes among births covered by private insurance (control group) and Medicaid (treatment group) before and after the policy implementation in January 2019. We first estimated a DD model without covariates (“unadjusted”) using logistic regression and reported marginal effects. 33 We then estimated a DD model controlling for covariates (“adjusted”) including age (categorical), mode of delivery (cesarean vs. vaginal), pregnancy complications (diabetes, hypertensive disorders of pregnancy, and prenatal mental illness), secular trends (calendar year), quarter indicators (e.g., January-March) to account for seasonality, and socioeconomic status based on the patient’s 5-digit ZIP code of residence.
Our DD design relies on the assumption that, prior to the policy implementation in January 2019, the trends in outcome measures for the Medicaid and privately insured groups exhibited common trends. To assess the validity of this common trend assumption, we estimated an event study regression for each outcome measure (Fig. 1). Overall, before January 2019, the differences between Medicaid and privately insured groups were minimal (i.e., near zero) and not statistically significant at a 95% confidence level for either any tele-mental health services use or any telehealth services use. However, the event study for any outpatient mental health visits suggests that Medicaid and privately insured groups may have followed different trends during the pre-implementation period. Therefore, we interpret our findings for any outpatient mental health visits with caution. Details of the DD specification (Supplementary Data) and event study (Supplementary Data) are provided in the online Supplement.
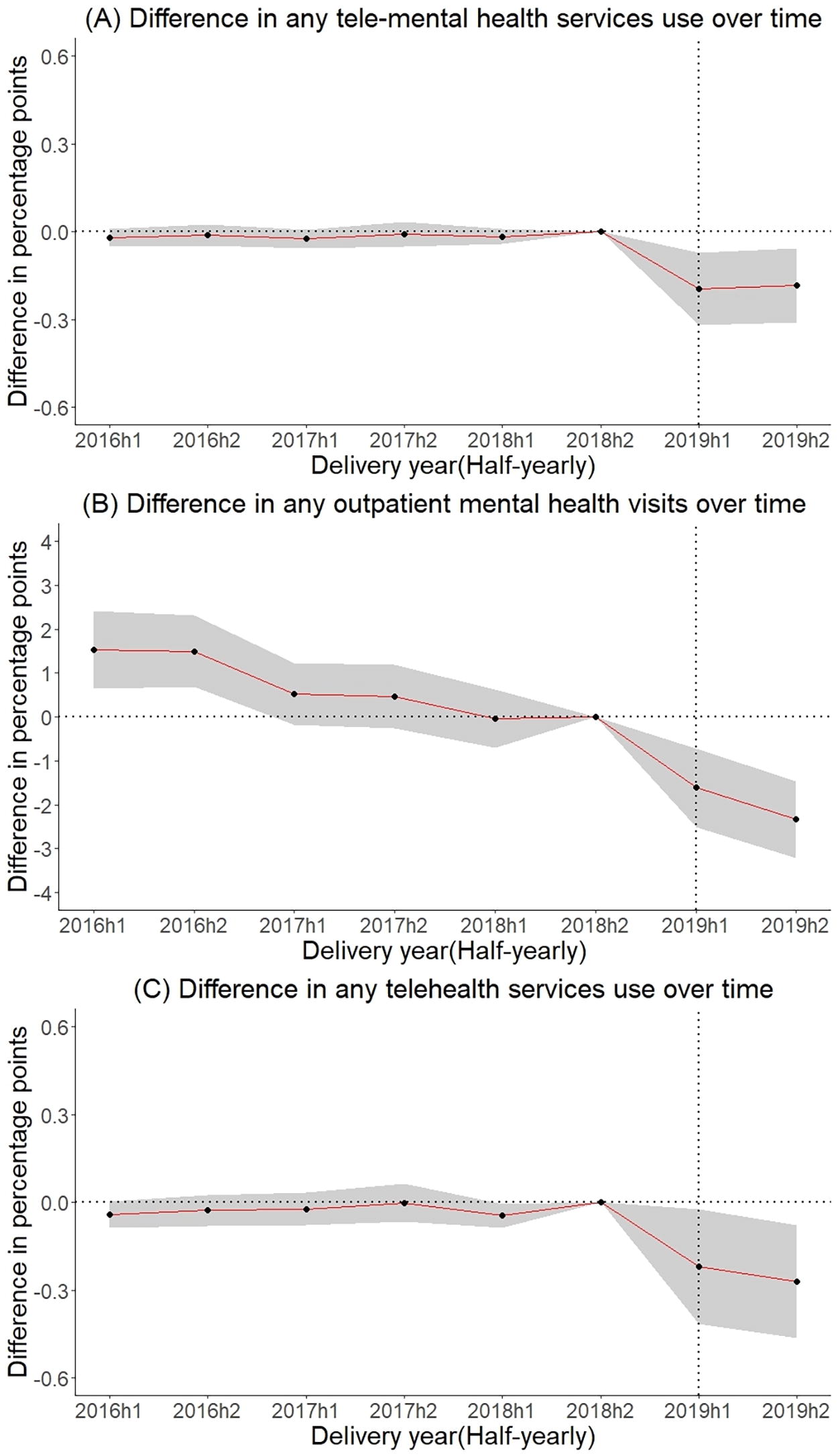
Event Study: Pre-trend analysis of outcomes. Medicaid vs. privately insured patients. Each point indicates the half-yearly difference in the outcome between Medicaid and privately insured groups, relative to the base time point, the second half year of 2018 (i.e., one half year before the policy implementation). The gray area depicts 95% confidence intervals. The event study specification shows the coefficient of Medicaid with half-yearly dummy variables, controlling for maternal age (categorical), delivery mode, pregnancy complications (hypertensive disorder, diabetes, and prenatal mental illness), and socioeconomic status (residence in the lowest median income ZIP codes and poverty-concentrated ZIP codes).
To further assess the robustness of our results and address concerns regarding potential changes in cohort characteristics over time and any imbalances between Medicaid and privately insured groups across pre- and post-policy periods, we employed propensity score weighting with the DD framework, as suggested by Stuart et al. 34 Specifically, we classified individuals into four distinct groups based on insurance type (Medicaid vs. private insurance) and timing (pre- vs. post-policy implementation). Using multinomial logistic regression, we estimated the probability (i.e., propensity scores) of each individual being in the groups based on observed characteristics. Propensity scores were subsequently utilized to construct inverse probability of treatment weights. Individuals in the reference group (private insurance and pre-policy implementation) received a uniform weight of 1, while individuals in other groups were assigned weights proportional to their probability of belonging to the reference group relative to their actual group. Applying these propensity weights enhanced the comparability of our groups.
We conducted a sensitivity analysis examining the outcome measures within 6 months postpartum (versus 3 months in our main analysis). While major postpartum mental illness often emerges within the early postpartum period, typically within the first few weeks after childbirth 35 and the comprehensive postpartum visit within 8 weeks includes depression screening as a recommended component, 36 extending the observation period to 6 months allows us to capture mental health services use resulting from conditions that may develop or be diagnosed later. This broader timeframe also ensures that our analysis accounts for the delayed onset of conditions and ongoing treatment needs beyond the immediate postpartum period.
We employed robust standard errors clustered at the 5-digit ZIP code level to account for correlations among births within the same geographic area and correlations due to multiple births to the same individual. We performed analyses using SAS, version 9.4 (SAS Institute Inc.), and Stata/MP, version 18 (Stata Corp LLC.).
Results
The analytic sample included 138,669 births, with 57,175 covered by private insurance and 81,494 covered by Medicaid (Supplementary Fig. S1). Over the full study period, use of tele-mental health services and telehealth services during the 3-months postpartum period was minimal (Table 1). Overall, 0.07% of the overall sample received tele-mental health services, and 0.29% used any telehealth services. Overall, 8.85% of individuals had any outpatient mental health visit, which was less common among individuals with Medicaid (8.05%) than those with private insurance (10%). Diabetes, hypertensive disorders, and cesarean rates were similar across insurance types. However, rates of prenatal mental illness were higher among those with Medicaid (19.8%) than those with private insurance (17.3%). Individuals with Medicaid were also significantly younger than those with private insurance.
Characteristics of Analytic Sample, Overall and by Insurance Type
p-values calculated using chi-squared tests for binary and categorical variables.
The unadjusted DD model indicates that the implementation of Massachusetts Medicaid coverage of tele-mental health services was negatively associated with all three outcome measures among Medicaid enrollees compared to those with private insurance (Table 2), although not statistically significant for tele-mental health use. The unadjusted estimate for tele-mental health use was very small (0.20 percentage point [pp] decrease, 95% confidence interval [CI]: −0.29 pp to 0.07 pp), and for outpatient mental health services visits, it was −3.23 pp (95% CI: −4.01 pp to −2.46 pp). For any telehealth services use, the unadjusted DD estimate was −0.23 pp (95% CI: −0.42 pp to −0.05 pp).
Unadjusted Difference-in-Differences: Effect of Massachusetts Medicaid Coverage of Tele-Mental Health Services on Postpartum Mental Health and Telehealth Service Utilization
N = 138,669.
Estimation of difference-in-difference models was performed through logistic regression. Average marginal effects are reported, with 95% confidence intervals calculated using the delta method.
p < 0.05.
p < 0.01.
p < 0.001.
The adjusted DD model (Table 3) showed different estimates from those in the unadjusted model in terms of the effects’ magnitude and statistical significance. There were no significant changes in the probability of any tele-mental health visit among both Medicaid enrollees and those with private insurance from pre- to post-policy implementation. The DD estimate shows a relative increase of 0.08pp (95% CI: −0.02 pp to 0.17 pp) for Medicaid enrollees compared to those with private insurance, but this difference was not statistically significant.
Adjusted Difference-in-Differences: Effect of Massachusetts Medicaid Coverage of Tele-Mental Health Services on Postpartum Mental Health and Telehealth Service Utilization
N = 138,669.
Estimation of difference-in-difference models was performed through logistic regression, and average marginal effects are reported, with 95% confidence intervals calculated using the delta method. The regression model controlled for patient characteristics—age (categorical), delivery mode (cesarean vs vaginal), pregnancy complications (diabetes, hypertensive disorder of pregnancy, and any prenatal mental illness), socioeconomic status based on 5-digit ZIP code (residence in ZIP code with lowest-quartile median income and residence in ZIP code with concentrated poverty), quarter indicators, and secular-trends.
p < 0.05.
p < 0.01.
p < 0.001.
In the analysis of outpatient mental health visits, Medicaid enrollees experienced a nonsignificant decrease, while those with private insurance experienced a significant increase from 9.97% to 12% (2.04 pp increase, 95% CI: 1.21 pp to 2.86 pp). The DD estimate indicates a statistically significant decrease of 2.55 pp (95% CI: −3.28 pp to −1.83 pp) for Medicaid enrollees compared to those with private insurance. For any telehealth services, there were statistically significant increases for both Medicaid enrollees (0.06 pp, 95% CI: 0.02 pp to 0.11 pp) and those with private insurance (0.23 pp, 95% CI: 0.08 pp to 0.39 pp). However, the adjusted DD estimate was also not statistically significant (−0.17 pp; 95% CI: −0.39 pp to 0.05 pp), indicating minimal change from pre- to post-implementation among Medicaid enrollees compared to those with private insurance.
As described in the Methods section, we assessed whether our propensity score-weighted analysis addressed potential cohort effects and ensured comparability of the population over time. After applying propensity score weights, we examined the balance of covariates across the four groups defined by insurance type (Medicaid vs. private) and policy period (pre- vs. post-policy implementation). Supplementary Table S5 presents the descriptive statistics (mean and variances) for each covariate by insurance type and policy period, while Supplementary Table S6 provides standardized mean differences (SMD) and variance ratios (VR) comparing each group to the reference (private insurance and pre-policy implementation period). After applying propensity weights, all covariates exhibited excellent balance across groups, with SMD values below the commonly accepted threshold of 0.1 and VR values near 1.0, 37 indicating minimal covariate differences and supporting the robustness of our propensity-weighted DD. Based on the good covariate balance achieved, we conducted a propensity score-weighted DD analysis as a robustness check. Results from this analysis (Supplementary Table S7) closely mirrored our primary findings (Table 3) in direction, magnitude, and statistical significance. Specifically, the propensity score-weighted estimates showed no statistically significant DD increase in any tele-mental health visits among Medicaid enrollees relative to privately insured individuals. Similarly, the patterns for outpatient mental health visits and any telehealth services remained consistent with the primary results. These findings confirm the robustness of our main results, indicating that they are not sensitive to potential differences in cohort composition.
The sensitivity analysis (Table 4) extended the observation period from 3 months postpartum to 6 months postpartum. The results of sensitivity analysis were very similar to the primary analysis in overall patterns. For both tele-mental health services use and any telehealth services use, the changes among Medicaid enrollees, compared to those with private insurance, remained statistically insignificant. However, the magnitude of the decrease in outpatient mental health visits was more pronounced in the sensitivity analysis, with a larger negative DD estimate, suggesting that the extended observation period captured a more substantial relative reduction in outpatient mental health visits. Again, this change was related to increases in visits among those with private insurance with unchanged rates among those with Medicaid.
Sensitivity Analysis: Effect of Massachusetts Medicaid Coverage of Tele-Mental Health Services on Postpartum Mental Health and Telehealth Service Utilization (6 Months Postpartum Outcomes)
N = 72,215.
Sample restricted to those who had a live birth from January 1, 2016 to September 12, 2019 in order to observe a 6-month postpartum window for each individual up until March 10, 2020 when Massachusetts declared a state emergency in response to COVID-19. Estimation of difference-in-difference models was performed through logistic regression, and average marginal effects are reported, with 95% confidence intervals calculated using the delta method. The regression model controlled for patient characteristics—age (categorical), delivery mode (cesarean vs. vaginal), pregnancy complications (diabetes, hypertensive disorder of pregnancy, and any prenatal mental illness), socioeconomic status based on 5-digit ZIP code (residence in ZIP code with lowest-quartile median income and residence in ZIP code with concentrated poverty), quarter indicators, and secular-trends.
p < 0.05.
p < 0.01.
p < 0.001.
Discussion
Overall, our analysis indicates that the implementation of parity in payment for tele-mental health services for Medicaid enrollees prior to the COVID-19 pandemic did not lead to a significant increase in postpartum use of these services, either among Medicaid enrollees overall or as compared to privately insured individuals. Despite the policy change aimed at enhancing access, utilization remained minimal, suggesting that financial incentives alone were insufficient to increase service use. This result underscores the complexity of addressing mental health service utilization, where financial incentives must be complemented by broader systemic changes.
In the post-pandemic period, many states have recognized the value of telehealth and have made temporary telehealth policies permanent. For example, the Centers for Medicare and Medicaid Services (CMS) extended telehealth flexibilities for Medicare and encouraged states to adopt policies that ensure continued reimbursement for telehealth services. 38 This emphasis on flexibility is particularly important for Medicaid beneficiaries, as it maintains support for telehealth as a viable option, potentially increasing access for this vulnerable population. Similarly, Massachusetts and other states have continued to support telehealth reimbursement at parity with in-person visits to maintain access to care for vulnerable populations. 39
One study found that at the outset of the pandemic, only 43% of outpatient mental health treatment facilities in the U.S. reported offering telehealth services, with access particularly limited in facilities accepting Medicaid in Northeast. 40 This low availability for Medicaid enrollees may contribute to our findings that Medicaid enrollees did not show a significant uptake of tele-mental health services. This suggests that in addition to the relatively low availability of telehealth services, structural and systematic barriers may have prevented Medicaid enrollees from using these services effectively. Another research with a national sample showed sharp increases in tele-mental health availability after the onset of the COVID-19 pandemic, with the number of outpatient mental health treatment facilities offering telehealth increasing by 77% from January 2020 to January 2021. However, disparities in telehealth use persist, with lower uptake among Medicaid enrollees who face additional barriers such as digital literacy and provider readiness. 41
The minimal changes in uptake of tele-mental health services among Medicaid enrollees highlights that payment parity alone is insufficient to enhance service utilization. This low utilization likely stems from barriers for both providers and patients. Providers may face challenges offering tele-mental health services due to a lack of training or incentives. 42,43 Patients, on the other hand, may struggle with digital literacy, internet access, and awareness of telehealth options. 44 Effective implementation, therefore, requires a comprehensive approach that includes improving digital literacy and internet access for patients, while also incentivizing and training providers. Addressing these barriers can create a more supportive environment for the utilization of tele-mental health services.
Notably, we observed greater telehealth uptake among privately insured individuals than among Medicaid enrollees, a difference that may reflect the disparate impact of these barriers. While the previously described challenges (e.g., digital literacy and internet access) affect many postpartum individuals, they likely fall more heavily on those insured by Medicaid, who often have fewer resources and provider options. Consequently, payment parity alone may be inadequate to boost tele-mental health utilization for Medicaid-insured populations, underscoring the need for more targeted solutions beyond reimbursement policy.
Study limitations
This study has several limitations that should be considered when interpreting the findings. First, our study focused on Massachusetts. As a result, the findings may not be generalizable to other states with different Medicaid policies, health care infrastructures, or socioeconomic conditions. However, as the Massachusetts health care system is generally considered to be of high quality, 45 uninsurance rates are low, and broadband access is relatively high 46 the fact that tele-mental health reimbursement parity was not effective at raising utilization rates in Massachusetts suggests that other states are also likely to face substantial barriers. Second, we were unable to capture important contextual factors such as patient preferences, provider capacity, and technological readiness, all of which could influence the uptake of tele-mental health services. These unmeasured factors may potentially explain the minimal increase in utilization following the policy change. Finally, our post-policy implementation period ends in March 2020, just before the onset of the COVID-19 pandemic. Although this allows us to isolate the effect of tele-mental health reimbursement policy from the confounding effect of pandemic-related changes, it limits our ability to examine the longer-term impact of the policy, particularly in light of the widespread adoption of telehealth during the pandemic.
Conclusion
While payment parity for tele-mental health services in Medicaid is a significant step, our findings indicate that it must be accompanied by broader efforts to address existing barriers. Further research should explore the role of socioeconomic factors, technological barriers to access to telehealth, and other potential barriers that might influence the effectiveness of telehealth as a delivery model for mental health services during the postpartum period. This study sets the foundation for future investigation and policy adjustments that could more effectively support birthing individuals’ mental health during the critical postpartum period.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Institute for Health Care Management (NIHCM) Foundation. Dr. Geissler reports funding from the National Institute of Mental Health (R34MH123628). The funders had no role in study design, analysis, interpretation of data, or in the preparation, review or approval of the article, or the decision to submit the article for publication. The article’s contents are solely the responsibility of the authors and do not represent the official views of the NIHCM Foundation or the National Institute of Mental Health.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.