
Abstract
Background:
Dobbs v. Jackson Women’s Health Organization (Dobbs) has had far-reaching effects on reproductive health care in the United States. Studies have shown increased demand for permanent contraception following Dobbs. In the Military Health System (MHS), vasectomy incidence increased significantly post-Dobbs. No research has yet evaluated the impact of Dobbs on permanent contraception for women (tubal ligation/sterilization) in the MHS.
Methods:
We queried health care data from the MHS Data Repository to identify active-duty servicewomen (ADSW) ages 18–45 between fiscal years 2020 and 2023. Study analyses included descriptive statistics, monthly incidence rates of tubal ligation/sterilization per 1,000 ADSW overall and at the state level to compare trends in Texas and Virginia, and t-test and chi-square tests to assess demographic differences before and after Dobbs.
Results:
Of the 339,052 ADSW included in the study, less than 2% received tubal ligations/sterilizations during the study period. The majority of these were aged 30–34 years, non-Hispanic White, married, senior enlisted, and in the Air Force. There was an abrupt increase in tubal ligations/sterilizations among ADSW within 2 months after Dobbs, and the rate remained above pre-Dobbs levels for 4 months. No differences were observed in the rate of tubal ligation/sterilizations in Texas and Virginia.
Conclusions:
The trend in tubal ligations/sterilizations among ADSW mirrors the general population. The abrupt increase indicates an association between Dobbs and changes to contraceptive decision-making. It is important to consider these changes to understand the short- and long-term effects of Dobbs on reproductive health care in the MHS and the nation.
Keywords
Introduction
The June 2022 US Supreme Court decision in Dobbs v. Jackson Women’s Health Organization (Dobbs) has had far-reaching effects on reproductive health care beyond restricting abortion access. As of November 2024, 13 states implemented total bans on abortion, and many of these states have also instituted reproductive health policies that limit access to and coverage of contraception.1,2 Many health care providers who provide contraceptive care (including obstetrician-gynecologists) have left highly restricted states, further limiting the ability of women in these states to access the full spectrum of reproductive health care. 2
Women are a growing population in the US military, representing 17.5% of active-duty service members (ADSMs) in 2022. 3 As the proportion of ADSMs who are women grows, so does the population at risk for unintended pregnancy. The Military Health System (MHS) offers access to all common forms of prescription contraception and sterilization for men and women at no cost; however, active-duty servicewomen (ADSW) use highly effective contraceptive methods at a lower rate than the general U.S. population, which is associated with a higher rate of unintended pregnancy. 4 An estimated 54% of pregnancies among ADSW are unintended, compared to 45% in the general U.S. population. 5 Unintended pregnancy is associated with negative impacts on maternal and child health, and poses a significant risk to individual and military unit readiness.5,6 In FY 2019, unintended pregnancy among ADSW resulted in an estimated 4,629,215 lost readiness days. 5 Therefore, contraceptive care is a critical focus for servicewomen’s health care.
ADSW are a unique population in the current U.S. reproductive health care environment. While ADSW are able to receive their reproductive health care at no cost through the MHS, they are not able to decide where they live and serve. Several large military installations are located in states where abortion was banned post-Dobbs, such as Texas, which has the third highest number of stationed ADSMs, after California and Virginia. 7 Approximately 80,000 ADSW live in states where abortion was banned post-Dobbs. 8 The Hyde Amendment prevents the use of federal funds for abortion care except in cases of rape, incest, or if the mother’s life is in danger (covered abortion care). 9 For all other non-covered abortion care, ADSW are not able to receive care at a military treatment facility or be reimbursed through TRICARE, the Department of Defense (DoD) health insurance program. 9 Therefore, like civilian women, ADSW are greatly impacted by the abortion laws in the states where they reside. However, ADSW face additional barriers to abortion care compared to civilian women in that they must receive permission to take time off from work and travel, including providing leadership with their travel plan. 9
Several studies have shown the impact of Dobbs on contraceptive decision-making for men and women in the United States. Demand for permanent contraception (also known as sterilization, including tubal ligations and vasectomies) increased in the months following the Dobbs decision, notably among younger adults.10–12 In states where abortion was banned, tubal ligations/sterilizations in the general U.S. population continued to increase in the 6 months following Dobbs, and prescriptions for oral contraceptive pills and emergency contraceptives declined.11,13 These changes in choice of contraceptive method may reflect concerns about restricted access to abortion and other forms of contraception.
In the MHS, there was a significant increase in vasectomy incidence, particularly among younger men, in the months following Dobbs. 7 Vasectomy incidence post-Dobbs varied by state, with a significantly greater increase in Texas, which immediately implemented an abortion ban, than in Virginia, which did not impose any immediate restrictions on abortion access.1,7 This suggests that the Dobbs decision had a similar impact on contraceptive decision-making for young men in the MHS as it did in the general U.S. population. However, no research has yet evaluated the effect of Dobbs on permanent contraception for women in the MHS. We therefore examined changes to the rate of tubal ligation/sterilization procedures among ADSW after the Dobbs decision.
Methods
We queried health care data from the MHS Data Repository (MDR) to identify ADSW of reproductive age between fiscal years (FY) 2020 and 2023. This period was selected as it allowed continued analysis from the point where Barnhart et al., 2024 ended (FY 2019) up to the most recent and complete data available (FY 2023) at the time of analysis. The MDR is a central data repository for health encounters at military treatment facilities (aka direct care), TRICARE administrative claim data (aka private sector care), and filled prescription data for all MHS beneficiaries, which includes active duty personnel, retirees, and their family members. 14 Unique identifiers, such as but not limited to International Classification of Diseases (ICD) diagnosis and procedure codes and Current Procedural Terminology (CPT) codes, can be used to query MDR data for related health care events and claims.
The study population included all women (determined by sex assigned at birth) ages 18–45 serving in active duty status in the US Army, Air Force, Space Force, Navy, and Marine Corps. ADSW under 18 and over 45 were excluded, consistent with the larger body of contraceptive literature.15–17 Female service members in the National Guard, Reserves, and Coast Guard were excluded from analysis due to their inconsistent access to care. ICD-10 diagnosis and procedure codes and CPT codes were used to identify the incidence of bilateral tubal ligation and sterilization procedures; a full list of codes can be found in Supplementary Data. ADSW who had received a tubal ligation/sterilization prior to the start of the study period were excluded. Monthly incidence rates per 1,000 ADSW were calculated as the number of ADSW with tubal ligation/sterilization divided by the number of eligible ADSW. Tubal ligation/sterilization trends were examined in the total population of identified ADSW and at the state level to compare trends among ADSW in Virginia, which kept its previous abortion policy, and Texas, which implemented a restrictive policy post-Dobbs. In addition to the difference in abortion policies in these two states, Texas and Virginia were chosen for comparison because they have the second and third highest number of stationed active-duty servicemembers and have sizable representative populations from all military services. 7
Study analyses included descriptive statistics on patient demographics (categorical age, race and ethnicity, marital status, rank as a proxy for socioeconomic status [SES], and branch of service), chi-square tests for differences in demographic proportions by tubal ligation/sterilization status, trend lines of monthly tubal ligation/sterilization incidence rates, and two-tailed t-test or chi-square tests to compare demographic differences for tubal ligation/sterilization before and after Dobbs. July 1, 2022 was used as the cutoff to mark the start of the post-Dobbs period. Statistical significance was set a priori to α = 0.05 and all analyses were performed using SAS version 9.4. This study was reviewed and classified as exempt by the Uniformed Services University of the Health Sciences’ Institutional Review Board.
Results
A total of 339,052 ADSW between the ages of 18 and 45 were identified for inclusion in the study from FY 2020 to 2023. Less than 2% (N = 5,679) of ADSW received bilateral tubal ligation/sterilization during this period, of which, the majority occurred in the pre-Dobbs period (N = 3,557; 62.6%). The majority of ADSW with tubal ligation/sterilization were between the ages of 30 to 34 (28.4%), of non-Hispanic White race and ethnicity (45.0%), married (71.6%), in a Senior Enlisted rank (64.0%), and in the Air Force (35.5%) (Table 1).
Demographics of ADSW by Tubal Ligation/Sterilization, Fiscal Years 2020–2023

Statistically significant, chi-square p value <0.05. Chi-square tests were used to assess the difference in proportions between those with/without tubal ligation/sterilization by each demographic factor.
Missing race totaled 2.8% and values are excluded from the table due to low cell counts and to protect the anonymity of patients. “Other” rank includes warrant officers and anyone with incomplete rank or pay grade information.
ADSW, active-duty servicewomen.
There was an abrupt increase in tubal ligations/sterilizations among ADSW within 2 months after Dobbs (2.03 per 1,000 ADSW in August 2022 from 1.51 per 1,000 in June 2022), and the rate remained above pre-Dobbs levels for 4 months after the ruling (ranging from 1.59 to 2.28 per 1,000; Fig. 1). A year after the ruling, the tubal ligation/sterilization rate had returned to pre-Dobbs levels (1.00 per 1,000 in June 2023). In the comparison of rates in Virginia and Texas, both had peaks in rates after Dobbs (VA: 2.33 per 1,000 in August 2022; TX: 2.76 per 1,000 in August 2022), however, these were not higher than peaks previously experienced before Dobbs (highest peak: VA = 2.73 per 1,000, TX = 2.76 per 1,000). All monthly rates can be found in Supplementary Data(Supplementary Table S1).
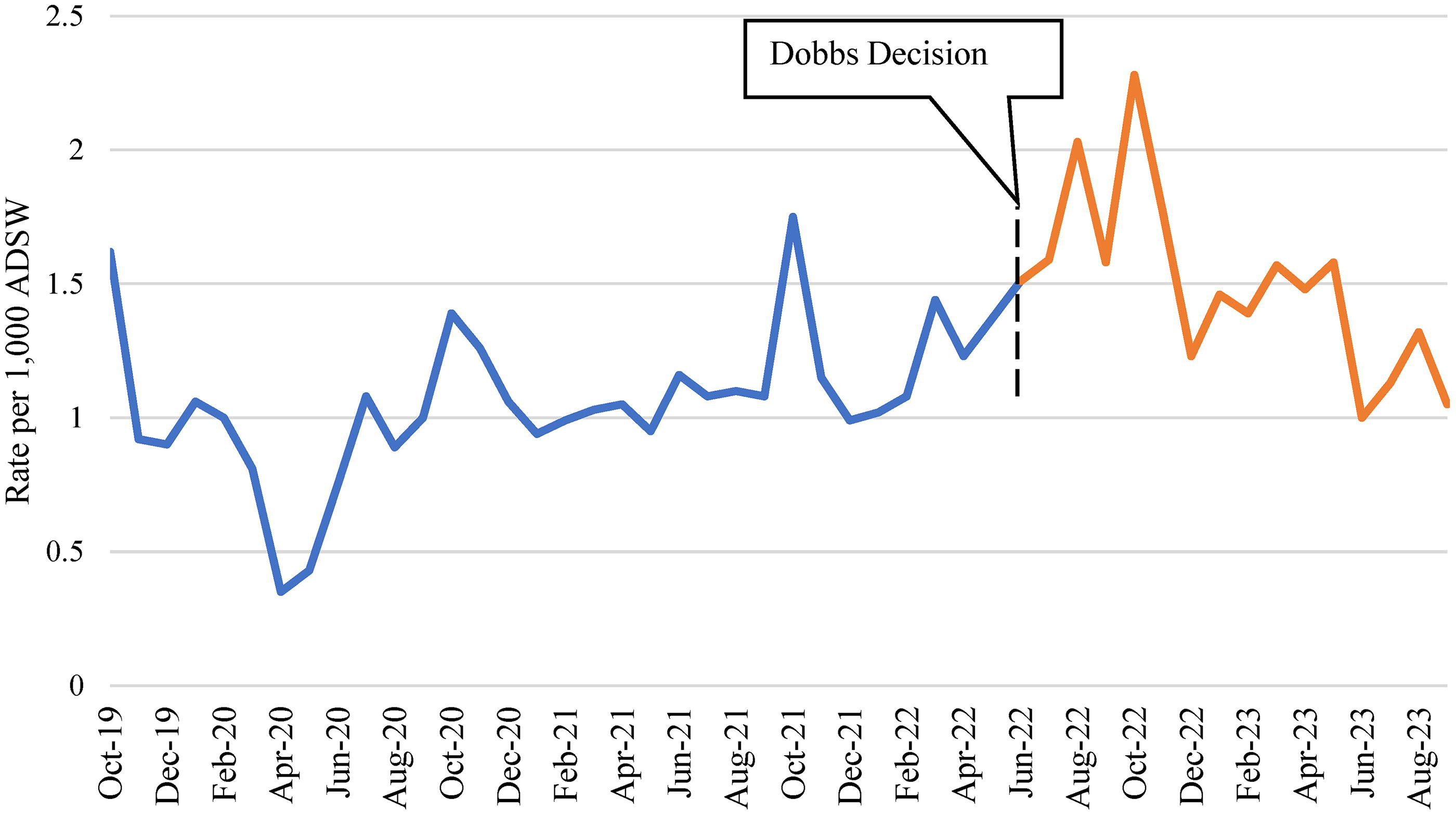
Trend in the Rate of Tubal Ligations Among Active-Duty Servicewomen, FY 2020–2023.
Table 2 details the p value results for t-test and chi-square tests used to compare demographic differences in ADSW with tubal ligation/sterilization in the pre- versus post-Dobbs period. We observed a significant difference in the average age for tubal ligation/sterilization before and after Dobbs, with the average age being slightly younger after Dobbs: 32.1 years before Dobbs compared to 31.4 years after Dobbs (p < 0.0001). Significant differences before and after Dobbs were also observed by rank (p = 0.0024) and branch of service (p = 0.0273). By rank, higher proportions of tubal ligation/sterilization after Dobbs were observed in Junior Enlisted, Junior Officers, and Senior Officers. By branch of service, similar proportions were observed across the services, except for the Marine Corps with a higher proportion of tubal ligation/sterilization observed after Dobbs. No differences were observed by race and ethnicity (p = 0.4202) and marital status (0.0523).
Demographic Differences in Tubal Ligations/Sterilizations Pre- and Post-Dobbs Decision in ADSW, Fiscal Years 2020–2023 (N = 5,679)

Values for Space Force are not presented to protect patient anonymity due to small cell counts. Small cells are defined as any with counts <11.
Discussion
The trend in tubal ligations/sterilizations among ADSW mirrors that of the general population, with a sharp increase in the incidence of these procedures immediately following Dobbs. The abrupt increase indicates an association between the ruling and changes to contraceptive decision-making among ADSW receiving care in the MHS. The average age of ADSW with a tubal ligation/sterilization was significantly younger after Dobbs, which aligns with trends in the general U.S. population of younger women choosing permanent contraception following Dobbs. 10 While the incidence of vasectomies post-Dobbs increased significantly more in Texas than in Virginia, a similar difference was not observed in tubal ligation and sterilization procedures, indicating that state level restrictions on abortion access may not have played a significant role in ADSW’s contraceptive decision-making. 6
Although ADSW have universal health coverage in the MHS, they are not able to decide where they live and serve. After the Dobbs decision, the DoD implemented a policy allowing service members to be reimbursed for the costs of traveling to receive reproductive health care that is not available on base and is not covered by TRICARE, including abortion care and certain fertility treatments. 9 In February 2025, this policy was amended and no longer covers travel for abortion care. 18 This increases the financial burden on ADSW seeking abortion care, who will now have to pay for travel and lodging on top of the cost of the procedure. In states with restrictive post-Dobbs abortion laws, including the closure of family planning clinics and departure of health care providers means that ADSW in these states have to travel even further to the nearest facility providing non-covered reproductive health care.2,13,19 ADSW stationed in Texas, Louisiana, and North Dakota face travel times of over 8 hours to reach the nearest facility that provides abortion care.9,19 ADSW must request and receive permission from leadership to take time off and travel to receive reproductive care not available at their duty location, a process which can take days or weeks, creating additional barriers and potentially resulting in delays in care. 9
Unintended pregnancy can limit the ability of ADSW to fully participate in their military career, and the restrictions introduced by Dobbs have the potential to further increase the number of unintended pregnancies carried to term. 8 An unintended pregnancy during deployment can result in delayed prenatal care and medical evacuation, as well as career repercussions.20,21 Young, Junior Enlisted ADSW have the highest estimated prevalence of unintended pregnancy, and some of the lowest rates of highly effective contraceptive use. 5 We use rank as a proxy for SES among ADSW, with Junior Enlisted being the lowest SES group. Therefore, ADSW with the least resources to travel to receive abortion care are those at highest risk for unintended pregnancy.
Increasing access to contraceptive care and counseling in the MHS is key to reducing unintended pregnancy and the associated negative impacts on ADSW’s lives and careers, particularly in light of the limited access to abortion care that they face. With universal coverage of prescription contraception and sterilization procedures in the MHS, ADSW do not experience the same financial barriers to accessing these services as they do to receiving non-covered reproductive health care. However, barriers to accessing reproductive health care in the MHS remain, with patients reporting difficulty scheduling appointments and taking time off to attend appointments, as well as delays receiving the contraceptive method of their choice.22,23 In 2023, walk-in contraceptive clinics were introduced at military hospitals and clinics in an effort to increase access to reproductive health care in the MHS. 24 No research has yet evaluated the impact of these clinics on the accessibility and uptake of contraceptive care among ADSW.
Best practices for contraceptive care enable reproductive autonomy through patient-shared decision-making and access to culturally appropriate education regarding contraceptive options.25,26 A previous study showed that few ADSW receive contraceptive counseling, and even fewer received counseling prior to deployment. 22 Increasing contraceptive education and access during basic training has been shown to increase the uptake of contraception and reduce rates of childbirth among young, Enlisted ADSW who are most at risk of unintended pregnancy. 23 Expanded access to contraceptive counseling in the MHS would help ADSW, particularly those who are young and less educated, to be aware of their options for preventing pregnancy in order to make informed decisions. Comprehensive contraceptive care should be both available and accessible through the MHS to reduce unintended pregnancy and ensure that ADSW are receiving the best reproductive health care.
Limitations
This study utilized secondary health care claims data to identify incidence rates of tubal ligation and sterilization among ADSW and therefore may underestimate the true incidence due to coding errors. This study also only reflects tubal ligation and sterilization procedures received in the MHS from 2020 to 2023 in an effort to provide a snap shot of trends before and after Dobbs, and therefore does not capture all ADSW that have undergone this procedure prior to the start of the study period. The study period pre-Dobbs contains the early COVID-19 pandemic, when access to in-person care was limited, likely resulting in a decreased amount of tubal ligation/sterilization procedures received during this time.
Conclusion
Incidence of tubal ligation/sterilization procedures among ADSW increased abruptly immediately following the Dobbs decision, mirroring trends in the general U.S. population. This reflects a change in contraceptive decision-making that is likely associated with the ruling. It is important to consider these changes in contraceptive decision-making to understand the short- and long-term effects of Dobbs on reproductive health care in the MHS and the nation. This study highlights that further exploration into the impact of Dobbs in the MHS is needed in order to provide the best reproductive health care for service members and their families. Future research should include qualitative data describing the experiences, beliefs, and intentions of ADSW across the United States concerning their contraceptive choices after the Dobbs decision.
Authors’ Contributions
T.P.K. designed the study. A.B. completed data analysis. All the authors contributed to writing and/or editing of the article and have reviewed the final version prior to submission.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Department of Defense, Defense Health Agency, award #HU00012120089. The funding agency played no role in the design, analysis, or interpretation of findings.
Disclaimer
The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, assertions, opinions, or policies of the Uniformed Services University of the Health Sciences (USUHS), the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF), the DoD, or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Ethics Approval
This study was found exempt from human subjects review by the Institutional Review Board of the Uniformed Services University of the Health Sciences.
Consent for Publication
Institutional clearance obtained.
Data Access
A.B. had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Data Availability Statement
The data that support the findings of this study are available from the United States
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.