
Abstract
Introduction:
Cervical cancer remains a significant public health challenge despite being largely preventable through early screening and treatment and is one of the largest causes of cancer-related deaths among women aged 20–39. New York State, with its diverse population, may have unique differences and disparities that can impact cervical cancer screening rates.
Methods:
Using the 2022 NYS Behavioral Risk Factor Surveillance System, we analyzed data from 3,968 participants. Bivariate analysis and logistic regression assessed the associations between demographic, general health, economic, and health behavior with cervical cancer screening.
Results:
Among the predictors of screening, we found that younger women were significantly less likely to screen compared with older women (aOR: 2.03; confidence interval [CI]: 1.67–2.46). Disparities were also observed by race (aOR: 1.55; CI: 1.27–1.89), income (aOR: 1.81; CI: 1.33–2.47), as well as type of insurance (aOR: 0.71; CI: 0.56–0.89). Health behaviors, such as having a prior checkup (aOR: 1.42; CI: 1.13–1.79) or flu vaccination (aOR: 1.32; CI: 1.10–1.57), were strongly associated with adherence, whereas personal economic barriers and general health challenges were largely not significant.
Discussion:
This study highlights health behaviors and engagement with the medical system as a significant predictor, suggesting that promoting trust in health care may enhance screening rates. The study also identified systemic barriers, such as insurance type and provider access, as determinants of cervical cancer screening.
Conclusion:
Addressing cervical cancer screening disparities in NYS requires interventions that consider behavioral and systemic factors. In particular, emphasizing trust in health care systems. These findings highlight areas of improvement in screening.
Introduction
Cervical cancer (CC) is an often-treatable disease, especially if caught early. However, not everyone screens for CC when recommended, which may cause it to be detected later, when the cancer is more progressed. In 2021, in the United States, among women aged 20–39, CC made up 11% (506/4,530) of cancer-related deaths and was the second leading cause of cancer death for women in this age group. 1 Screening rates for CC have not improved, and nationally rates of adherence have decreased.2,3 It is critical to ensure that more women who are recommended to screen for cancer do so, as it will save lives. Compared with other cancers, cervical cancer screening is the most impactful on the number of life years gained at 9.9–10.6 million in the United States, and full adherence to screening recommendations would increase the life years gained to 11.4–12.3 million. 2 One study in the state of New Mexico estimated that screening every 3 years prevented over 80% of CC stage 2 or greater. 4
Current guidelines suggest that women aged 21–29 should have a cervical cytology test (Pap smear) every 3 years. 5 Women aged 30–65 may screen with Human Papillomavirus (HPV) testing every 5 years, co-testing with a Pap smear and HPV test every five years, or test via Pap smear alone every 3 years. 5 HPV testing is often preferred over a Pap smear. A study comparing clinician-collected Pap tests versus HPV tests by self-sampling or urine sampling found reduced psychological distress in patients receiving HPV testing. 6 While routine testing is fairly simple, there are many women that do not screen for CC. In order to ensure CC screening adherence, there needs to be a greater understanding of the disparities related to screening, and there are many variables that may prevent women from desiring or having the ability to screen.
Women living in rural communities may be less likely to screen than those in urban communities. 7 Women who are low-income or have unmet needs such as food and shelter are also more likely to need CC screening. 8 Furthermore, those without insurance are much less likely to screen, and those with public insurance, such as Medicaid, are also less likely than those with private insurance.3,9 These disparities, fundamentally, are disparities between those who do not have the ability to screen or have a much more difficult time. It has been shown that for those who cannot screen but wish to, there is significant benefit from programs that take a more active approach in patient health and assist patients in being able to screen for CC.8,10 Furthermore, clinics that offer Pap smear at non-traditional hours, such as weekends, have high fill rates and assist patients who may traditionally not screen. 11
Non-Hispanic Black women overall screen at much lower rates than women of other racial groups for CC. 12 Racial and ethnic minorities are also likely to have never screened in comparison to White women. 13 Those who are Non-Hispanic Black are more likely to report having many (more than five) reasons for not being able to screen. Among the most common reasons cited, aside from cost and not having insurance, were having no time, being afraid, forgetting, or not having a doctor. 14 This is especially relevant when considering that Black women have a much higher incidence of CC and worse survival outcomes. 15
The state of New York (NYS) has an especially unique and diverse population. Women’s health disparities exist in many forms and are uniquely expressed in the state. For example, in NYS, factors of structural racism have been shown to impact severe maternal mortality rates. 16 Qualitative research from focus groups in Buffalo, NY, indicates that health equity is critical for cancer care and that interventions need to be culturally relevant and appropriate. 17 NYS is a Medicaid expansion state that has better access to women’s health services than non-expansion states. Despite that, women may still face barriers to care, as they face barriers to enrollment in Medicaid, for example, lack of knowledge or understanding eligibility, may not qualify for Medicaid but qualify for other NYS-specific programs, may face periodic disenrollment, may be ineligible due to their immigration status. The Affordable Care Act (ACA) requires public and private plans to cover cervical cancer screenings without any out-of-pocket expenses; however, this does not apply to follow-up care, for example, colposcopies. NY ranks 10th in overall women’s health and 5th in health outcomes yet 27th on quality and prevention. 18
This study focuses on cervical cancer screening in the NYS population. The NYS prevention agenda of 2019–2024 has a specific plan entitled “Promote Healthy Women, Infants, and Children Action Plan.” 19 Improving cancer screening rates for women falls under Goal 1.1 to “Increase use of primary and preventive health care services among women of all ages, with special focus on women of reproductive age.” 19 With this study, we intend to ascertain where public health efforts for improving screening should be implemented in order for the prevention agenda to succeed.
In this study, we will identify novel behavioral factors associated with CC screening in NYS. Our findings highlight cervical cancer screening disparities in NYS that require interventions that consider behavioral and systemic factors, including emphasizing trust in health care systems. These findings should inform on areas of improvement in screening.
Methods
The data used in this study come from the NYS 2022 Behavioral Risk Factor Surveillance System (BRFSS) survey. 20 All analysis, interpretations, and conclusions reached are the authors’ own. All statistical analysis was done via the IBM SPSS package version 29.
Adherence to cervical cancer screening was defined following the National Cancer Institute’s guidelines regarding cervical cancer screening, which recommends getting a first Pap test at age 21, followed by Pap testing every 3 years and at age 30, an HPV test or HPV-pap co-test every 5 years, or a Pap test every 3 years until age 65. 5
Initially, there were 17,800 participants in the BRFSS. Participants were excluded from the initial analysis if their sex at birth was male, had a hysterectomy, or were not in the age range of 24–65, as well as if data in these categories were missing. Women aged 21–23 were excluded from the analysis given that there is not enough time for participants in that age range who have not screened to be classified as nonadherent. Participants were also excluded if data were missing regarding whether they were screened for cervical cancer. The final number in the initial analysis was 1,719 who had not followed screening guidelines and 2,249 who had (n = 3,968). Participants aged 24–29 who had not screened within 3 years were considered nonadherent, while participants aged 30–65 were considered nonadherent if they had not screened within 5 years of a HPV test or HPV-pap co-test or within 3 years of a Pap test.
A supplementary analysis was done by limiting the sample to women aged 30–65. In this analysis, women aged 30–65 were included and participants were considered nonadherent if they had not screened within 5 years of a HPV test or HPV-pap co-test or within 3 years of a Pap test. This is consistent with both the National Cancer Institute and the American Cancer Society’s guidelines. 21
Initial bivariate analyses were conducted prior to the regression to see the unadjusted effects as well as to identify confounders. Following this, a binary logistic regression was performed using the included variables to assess which factors are associated with screening in a multivariable model after including confounders. Confounding variables include demographic data such as age, race, income, Hispanic origin, sexual orientation, gender, education, marriage status, and location. These variables have been seen to be significant in the scientific literature and were therefore included following bivariate analyses. Research variables included an assortment of data regarding general health, economic and health indicators, and health behaviors. The total number of participants included in the regression was 2,536 after participants were excluded if they had missing data.
Results
Table 1 reports on the bivariate analyses between independent variables and screening adherence, defined as 3 years since a Pap test or 5 years since an HPV or HPV-pap co-test for women above 29. Younger women (24–39) were less likely to screen than older women (40–65). Only 42.2% of young women were screened compared with 64.3% of older women (p < 0.001). Almost all other demographic variables, including race, income, Hispanic origin, sexual orientation, education, marriage status, and location (nonmetropolitan/metropolitan), were significantly associated with CC screening in the bivariate models (p < 0.05 for location, p < 0.001 for rest); gender was not significant (p = 0.056). Among the largest factors included education, where only 29.0% of women who did not complete high school were screened, and 59.1% of those who did complete high school or an equivalent (GED) screened. Among those with the highest levels of income at $100,000+, screening was very high at 72.1%, especially compared with those with an income of $0–34,999 at 42.1%. Furthermore, 63.0% of White women were screened, while only 44.5% of non-White women were. Similarly, 60.4% of non-Hispanic women were screened, while only 41.5% of Hispanic women did.
Bivariate Analyses of Factors Associated with Screening Adherence
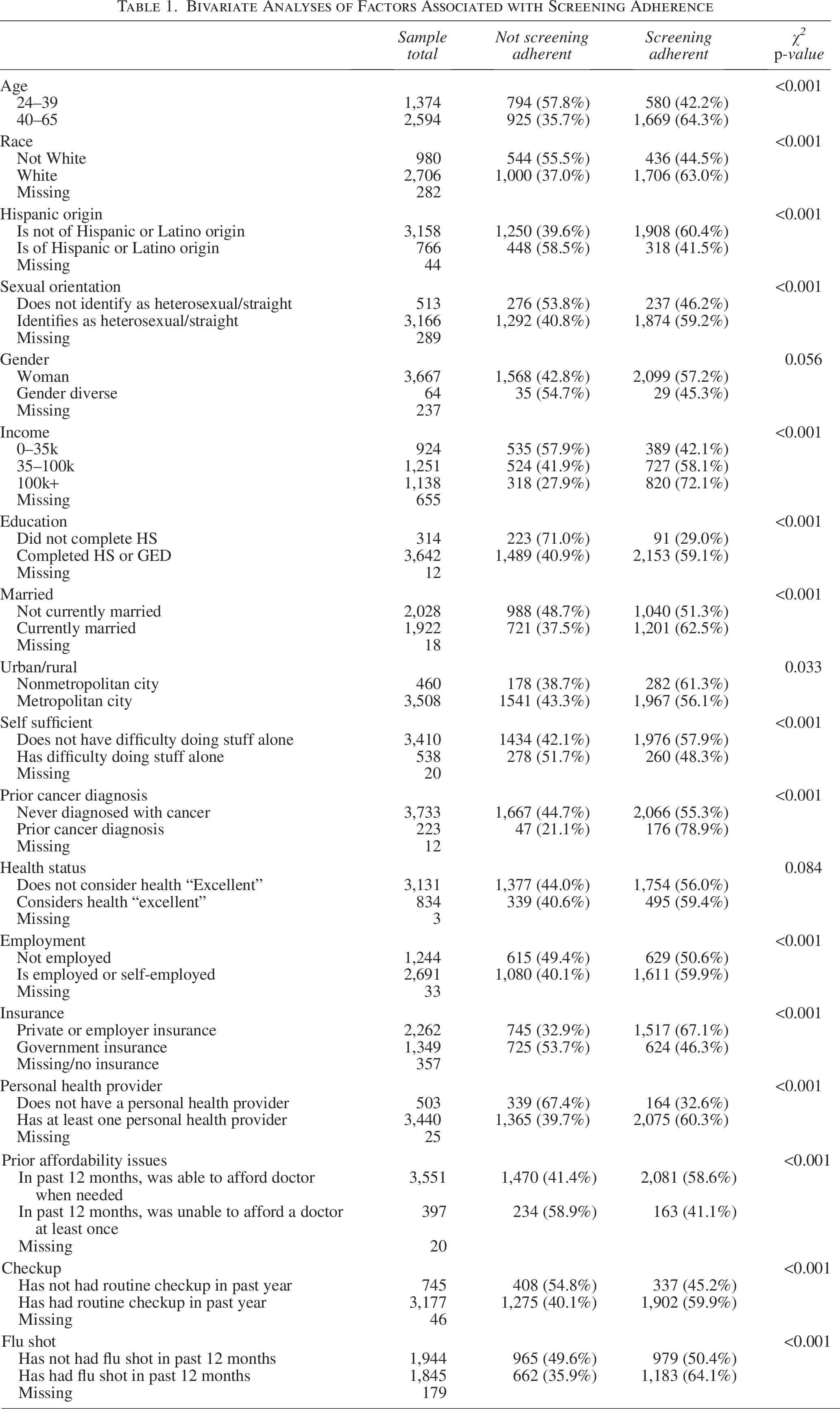
Most other predictive variables were found to be significant. This includes data regarding the participants' general health, such as if they felt self-sufficient (p < 0.001), however, not whether considered their health to be excellent (p = 0.084). Furthermore, participants with economic or health indicators, such as not being employed, on government insurance, and not having a personal health provider, all screened at lower rates (p < 0.001 for all). Lastly, participants engaging in health behaviors such as an annual checkup and annual flu shot screened at higher rates than those who did not (p < 0.001).
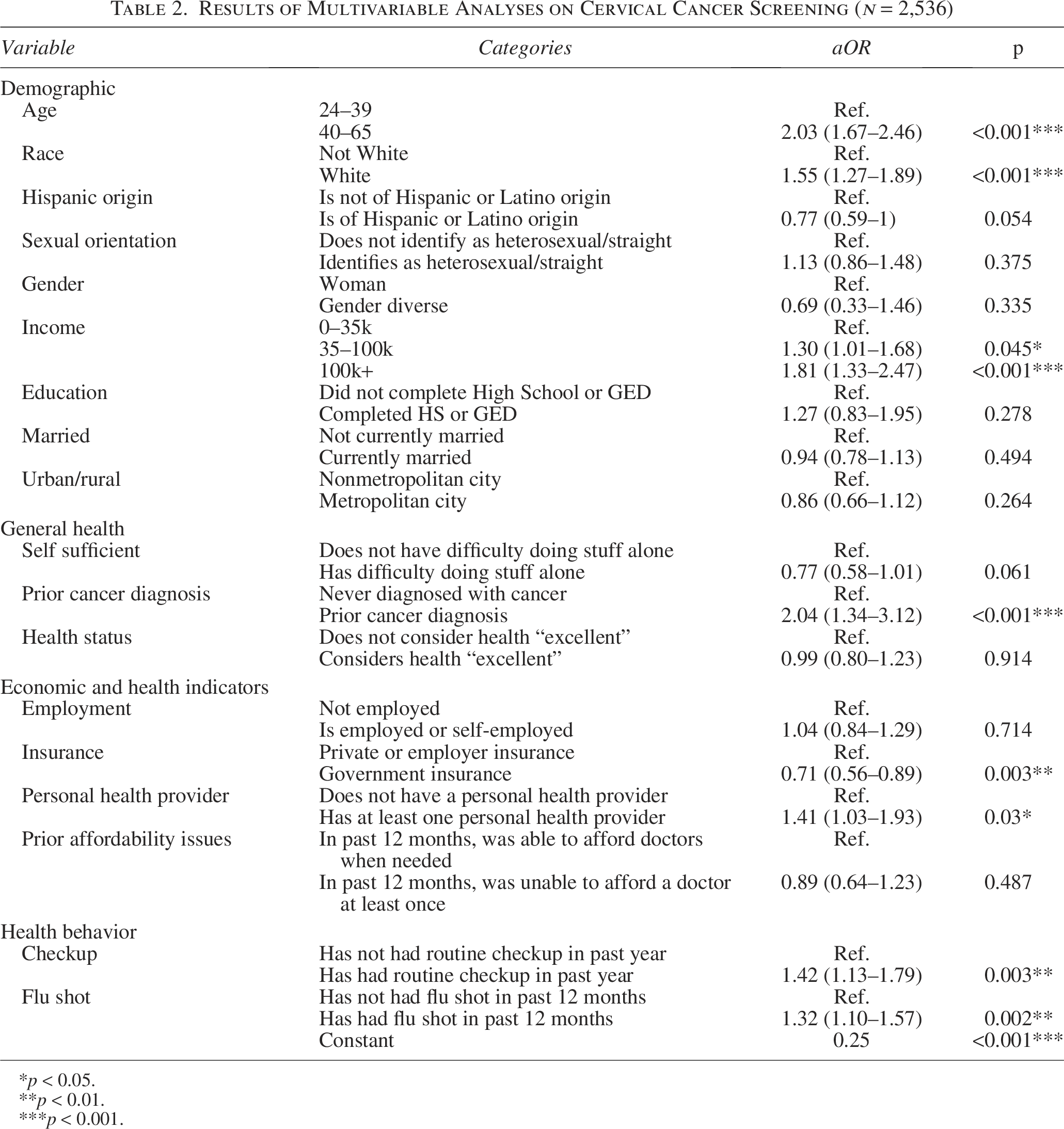
Following this analysis, all variables were included in a logistic regression. The full regression can be seen in Table 2. The model has a Nagelkerke R2 of 0.16. Additionally, the Hosmer-Lemeshow test yields a p-value of 0.552, suggesting that the model provides a good fit to the data, as the p-value is greater than the commonly used threshold of p > 0.05.
Results of Multivariable Analyses on Cervical Cancer Screening (n = 2,536)
p < 0.05.
p < 0.01.
p < 0.001.
The regressors among confounding demographic data that remained significant included age (aOR: 2.03; CI: 1.67–2.46), race (aOR: 1.55; CI: 1.27–1.89), and income (aOR: 1.30; CI: 1.01–1.68 for $35–$100k; aOR: 1.81; CI: 1.33–2.47 for $100k+). In terms of general health, the only significant predictor of CC screening was a prior cancer diagnosis (aOR: 2.04; CI: 1.34–3.12). Furthermore, the only economic and health indicators that remained significant were insurance status (aOR: 0.71; CI: 0.56–0.89) and having a personal health provider (aOR: 1.41; CI: 1.03–1.93). Lastly, prior health behaviors, such as a prior checkup (aOR: 1.42; CI: 1.13–1.79) and prior flu shot (aOR: 1.32; CI: 1.10–1.57) within the past year were both significantly associated with screening for CC.
An additional regression was performed consisting of those aged 30–65 to determine if any factors do not remain statistically significant in this sub-population. The full regression can be seen in Supplementary Table S1. No significant differences were seen between regression model and the original model.
Discussion
In this study, crucial factors have been identified to associate with CC screening. These variables fall into three overall categories, as well as a fourth category of demographic indicators. The three categories include the general health of the patient, the economic indicators (and subsequent ability or lack thereof to participate in health care), and the health behaviors of the patient (their willingness to participate in health care). Each category presents one possible hindrance for screening, and all are somewhat independent of one another.
Somewhat surprisingly, our study found that the ability to be alone and function alone was not a significant factor for screening. Similarly, if one did or did not consider their health excellent was not significantly associated with screening. While these factors were significantly associated with screening without confounders or covariates, in the full regression they are not. This indicates that the burden of health difficulties likely on its own may not be enough to prevent one from screening for cervical cancer. A report in 2013 indicates that women with disabilities are less likely to have a Pap test. 22 However, while the study controls for some factors in their model, others are missing, such as employment status or if there was a prior cancer diagnosis. It is also evident that lack of screening from disability status is at least in part due to other barriers, such as cost and access. 23 Other studies have found that the association of having a disability with screening was entirely gone when adjusted by relevant demographics, 24 which we found as well. If disability does indeed impact screening, the effect is minor. However, we did find that those who did have a prior diagnosis did screen at significantly higher rates. A prior cancer diagnosis has been shown to influence screening in many cancers, and this study supports that finding. 25 Therefore, in terms of general health, it appears that difficulties from personal health do not impact screening, or do so minimally, but a higher awareness of cancer due to prior health does.
Among the economic and health indicators, insurance status was a strongly associated variable of CC screening. Those with public health insurance were much less likely to screen for CC, highlighting a crucial need to target those with public health insurance when implementing screening campaigns. Those who had at least one personal health provider were also more likely to screen, while employment status and affordability issues were not statistically significant predictors. Overall, among the economic and health variables, the systemic issues (government insurance, access to a provider) proved to be significantly associated with screening, while the personal issues (employment, affordability issues) were not. This may suggest that participation in CC screening is prevented due to, in part, perceived and real hardships that are systemic in nature and affect communities rather than individuals. Community and neighborhood level interventions have been shown to be important, especially those that leverage the social determinants of health.26,27 This may extend to social perceptions of health care and cancer screening as well.
Lastly, both health behavior variables were found to be significantly associated with CC screening. This includes having a prior checkup within the last year as well as a flu shot. Both of these behaviors indicate to some degree, a willingness to operate within the current medical system. This is especially significant when considering that our model has adjusted for measures of access, such as insurance status and geographic location, as well as education, which may be associated with health literacy. The data suggest that the same people who do not participate in standard health care practice (e.g., getting a flu shot) will not utilize other services of health care (e.g., CC screening), even when controlling for all the relevant variables that have been included. Thus, health behavior is a crucial component associated with CC screening.
Certain demographic variables did remain significant. Age was found to be a strong predictor of CC screening, where older women screened at much higher rates. A report from the NYS Department of Health found similar results in 2020, where age was positively associated with screening rates. 28 However, this differs from other studies that find age is inversely correlated with screening nationally, 29 suggesting differences between NYS and the United States. It must be noted that for women not at risk for other cancers, CC is the first and only cancer that is routinely screened for until age 40, which may influence screening adherence in younger women. The especially large effect of age is quite high, and reflects a unique lack of younger women following CC screening guidelines in NYS. Additionally, disparities were identified across income and race, where those who are White and those with a higher income were found to screen at higher rates. These trends have been seen in the literature,12,30,31 and our findings identify that these issues exist in NYS as well.
The study does have a few limitations. The BRFSS is a survey where participants self-report, and participants may report inaccurately, participants may also not be sure if they have screened, giving us an incomplete picture. Furthermore, the BRFSS is a telephone survey with no compensation, so participants may be biased toward those who are capable and willing to participate in such a survey. The BRFSS does not distinguish between individuals undergoing routine screening and those receiving follow-up for abnormal results, which may partially bias the analysis. While we attempted to include all relevant confounding variables in our analysis, however due to the nature of the BRFSS and which questions are asked, there may be confounding demographic data that were not included.
Cumulatively, the results presented indicate that CC screening may be associated with trust and willingness to engage in the medical system, rather than solely economic barriers. We found that general health and ability to act alone did not associate with cancer screening, only a prior cancer diagnosis, which likely stems from an increased awareness of the cancer risks. We found that the main factors among economic factors that were associated with screening were those that stem from societal systemic issues rather than personal finances. We found that other health behaviors, such as flu vaccination and routine checkup, were significantly associated with screening. This suggests that those who are not screening for CC may be acting based on a decreased awareness of risk and a lack of willingness to partake in the medical system, rather than on ability. Similar findings have been seen in other studies. It has been seen in other studies that medical mistrust and distrust leads to delays in cancer screening.32,33 In one very large study done after a controversy in Ireland regarding screening, trust in the screening system, especially due to discrimination, was found to be an issue preventing women from screening. 34
We believe that these results suggest a novel finding in the realm of CC screening and can be particularly useful in NYS. NYS has the fourth highest incidence of CC in the United States, and therefore developing successful screening campaigns and interventions is especially important. 1 Our study found that while CC screening has typically been regarded as an issue of access, which is certainly true, it does not tell the full story. Divides across age, race, and income highlight that certain populations require targeted interventions to ensure equity in CC screening. In particular, campaigns that target younger women would be especially beneficial. Furthermore, we have identified that a history of nonparticipation in the medical system is associated with CC screening, which may indicate that medical mistrust is a large concern in NY. In a state such as NY, where cancer screening programs are available to all, it is important to consider the outlook and beliefs regarding the health system as a whole. We believe that our research indicates a strong need for public health efforts in NY targeting medical mistrust and concerns with health care to improve CC screening.
Authors’ Contributions
Methodology: A.S. and M.W. Formal analysis: A.S. Writing—original draft: A.S. Writing—review and editing: M.W. Visualization: A.S. Supervision: M.W.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.