
Abstract
Background:
Bacterial vaginosis (BV) is one of the most common vaginal conditions and is associated with significant obstetric and gynecological risks. Previous studies have demonstrated an association between menses and the vaginal dysbiosis underlying the development of BV. Given this association, we hypothesized that increased vaginal bleeding, such as abnormal uterine bleeding (AUB) caused by adenomyosis, might increase the risk of developing BV.
Objective:
This study assesses whether AUB in patients with adenomyosis was associated with BV diagnoses.
Methods:
We performed a retrospective study of 372 patients diagnosed with adenomyosis between 2016 and 2020 at a tertiary care center. Characteristics of patients who developed BV within 3 years of adenomyosis diagnosis were compared to patients without subsequent BV diagnoses.
Results:
The prevalence of BV in patients diagnosed with adenomyosis between 2016 and 2020 was 19.4%. Patients who developed BV following their diagnosis of adenomyosis had higher rates of menorrhagia than those who did not develop BV (p < 0.01). While patients with BV were primarily diagnosed with adenomyosis by radiological findings, patients without BV were mostly diagnosed with adenomyosis by post-hysterectomy histopathologic evaluation. Treatment of adenomyosis-related symptoms was significantly different between the two study groups. There was also a positive association between the prevalence of menorrhagia and the number of BV episodes, demonstrating a relationship between AUB and BV.
Conclusions:
This study provides evidence for an association between the menorrhagia caused by adenomyosis and a diagnosis of BV. Based on these findings, prospective studies are needed to assess the contribution of abnormal uterine bleeding pathologies to the development of BV.
Background
Bacterial vaginosis (BV) is the most common vaginal condition in women of reproductive age. 1 Internationally, the prevalence of BV can range from 20% to 60%, 2 with a prevalence of 29.2% in the United States. 3 Of note, prevalence varies based on race and ethnic group, with the African American race historically being considered a risk factor. 2 BV has been reported to impact 51.4% of non-Hispanic Black Americans, as compared to 23.2% of non-Hispanic White Americans. 3
Aside from bothersome symptoms including vaginal irritation, pelvic pain, and abnormal vaginal discharge, BV increases the risk of significant obstetric and gynecological complications, including: preterm birth, spontaneous abortions, intraamniotic infections, premature rupture of membranes, pelvic inflammatory diseases, and post-hysterectomy vaginal cuff dehiscence. 4 While there are standard antimicrobial treatments for bacterial vaginosis, such as the use of metronidazole, the recurrence rate is high, estimated to be between 50% and 80% within 12 months of completing treatment. 2,5 Given the high rates of recurrence and significant complications associated with BV, it is imperative to understand the underlying etiology of BV and improve the efficacy of BV treatments.
It is established that BV is characterized by a state of vaginal dysbiosis - a dysregulation of the vaginal microbiome. This dysbiosis is characterized by a decrease of the typically predominant Lactobacilli species and the increase of anaerobic bacteria species 6,7 such as Prevotella bivia, Gardnerella vaginalis, Atopobium vaginae, and Megasphaera type I. 8 It has been observed that the vaginal microbiome has a significant shift during menses, 9 with an overall increase in the microbial diversity and decrease in Lactobacilli species accompanied by an increase in Gardnerella vaginalis. 10,11 In one study, recurrent BV episodes were most likely to occur within 10 days of menses, despite receiving standard-of-care metronidazole therapy. 12 In another study, patients with self-reported irregular bleeding were more than twice as likely to develop BV. 13 When considering the previously established literature, it can be interpreted that vaginal bleeding and menstruation affect the vaginal microbiome in a way that predisposes patients to the development of BV. The impact of vaginal bleeding on the microbiome is likely secondary to the iron content of heme, as the availability of iron can improve the growth of specific vaginal flora. 14 The impact of iron on the microbiome has been studied in the context of other organ systems—for instance, the ingestion of iron has been shown to impact the gut microbiome in different study populations. 15,16 It is unknown whether conditions with increased exposure of blood to the vaginal canal, such as abnormal uterine bleeding (AUB), thereby incur a greater risk of BV to patients.
Different pathologies may contribute to AUB, some of which are structural within the uterus and others functional (i.e., coagulopathies, use of anticoagulants, ovulatory dysfunction). Of these possible etiologies, adenomyosis is a structural cause of AUB that can affect the vaginal microbiome. 6,17,18 While the true prevalence of adenomyosis in the general population remains unclear, adenomyosis has been detected in 8.8 to 61.5% of hysterectomy pathology specimens and 20.9% of women who had indications for transvaginal ultrasound. 19 Two-thirds of patients diagnosed with adenomyosis report symptoms, the most common symptoms including menorrhagia, dysmenorrhea, dyspareunia, and pelvic pain. 19 Alternatively, patients may be completely asymptomatic and only diagnosed during the work-up or surgical management of other gynecological disease processes. Patients with adenomyosis have been demonstrated to have significant differences in their vaginal microbiome compared to patients without adenomyosis; 6,17,18 and these differences can be impacted by the menstrual cycle. 6 It is unclear if the microbiome associated with adenomyosis may increase the propensity for BV development and/or recurrence.
Considering the adverse sequelae, widespread prevalence, and high recurrence rate of BV, we sought to characterize whether there was an association between adenomyosis and the development of BV. In this study, we examined the relationship between characteristics of adenomyosis, a form of AUB with previously reported vaginal microbiome changes, and the occurrence of BV.
Materials and Methods
Study design and data collection
This was a Johns Hopkins Medicine Institutional Review Board-approved (IRB00375447) retrospective cohort study. An EPIC Electronic Medical Record query was designed to identify patients aged ≥18 and diagnosed with adenomyosis within the Johns Hopkins Medical system. Adenomyosis diagnosis was defined by International Classification of Diseases ninth or tenth revision clinical modification (ICD-9-CM and ICD-10-CM) coding (Appendix A). The query was performed by a data extraction specialist from the Johns Hopkins Core for Clinical Research Data Acquisition.
A random sample of 1,187 patient charts from a total extracted population of 2,849 patients underwent chart review. To ensure that the sample of patients for chart review represented the general study population, 30% of each racial group were randomly selected for chart review. Subjects were excluded if they did not have a confirmed adenomyosis diagnosis, if their adenomyosis diagnosis was before 01/01/2016 or after 12/31/2020, or if they did not receive gynecological or obstetric care at Johns Hopkins Medicine at least 1 year prior to their adenomyosis diagnosis. Based on these exclusions, 372 subjects with a confirmed adenomyosis diagnosis met the inclusion criteria for cohort analyses (Supplementary Fig. S1). Diagnosis of adenomyosis was established by MRI, ultrasound, and/or histopathologic evaluation of hysterectomy specimens. Patient IDs and collected data were securely stored on the Secure Analytic Framework Environment virtual desktop.
Demographic and medical history
Two study team members conducted a chart review to collect additional information on the demographics and medical history of patients with adenomyosis. Data gathered during chart review included gynecologic symptoms at the time of adenomyosis diagnosis, method of adenomyosis diagnosis, comorbidities, tobacco use, medical and surgical managements utilized, and episodes of BV following adenomyosis diagnosis. Demographics included age, race/ethnicity, tobacco use (never versus ever tobacco use), and nulliparity. Race/ethnicity was subsequently categorized as Non-Hispanic Black/African American (“Black or African American”), Non-Hispanic White (“White”), and Non-Hispanic Other (Asian, American Indian or Alaska Native, and other). Medical history at the time of adenomyosis diagnosis included body mass index (BMI), comorbidities, and gynecological surgical history. Comorbidities abstracted included obesity, hypertension, diabetes, infertility, endometriosis, and fibroids. Surgical history included the history and number of Cesarean sections prior to adenomyosis diagnosis, as well as reported hysterectomy or myomectomy after adenomyosis diagnosis. Gynecologic symptoms at the time of adenomyosis diagnosis were reported as the presence of menorrhagia, anemia, pelvic pain, dysmenorrhea, abdominal bloating, or dyspareunia.
Statistical analysis
Characteristics of patients who developed BV within 3 years of adenomyosis diagnosis (N = 72) were compared to patients without subsequent BV diagnosis (N = 300) using the Student’s t-test for continuous variables and the chi-squared test for categorical variables. Among patients that reported medical treatment for vaginal bleeding (N = 212), we additionally compared BV status by treatment type using chi-squared tests. Multivariable logistic regression models were used to estimate odds ratios (OR, 95% confidence intervals [CI]) for BV comparing subgroups defined by demographic and medical history characteristics. Models were adjusted for race/ethnicity and tobacco use. All statistical analyses were conducted using R statistical software (version 4.4.1).
Results
Demographics and comorbidities
In the cohort of 372 patients, 72 (19.4%) were diagnosed with BV within 3 years of adenomyosis diagnosis. Of the 72 patients with BV, 14 (19.4%) had ≥3 episodes of BV. Patients who were diagnosed with BV after adenomyosis diagnosis were more likely to report their race as Black or African American (84.7% versus 61.5%) and less likely to identify as White (1.4% vs 27.4%) (p < 0.001, Table 1). There was no significant difference in age or BMI at the time of adenomyosis diagnosis between patients who ultimately developed BV within the following 3 years compared to those who did not. Nulliparity, history of cesarean section, and history of endometriosis were also not associated with development of BV (Table 1). There was no difference in an existing diagnosis of fibroids, another form of AUB, at the time of diagnosis between the two groups.
Demographics Table
Values reported are N (%), except for age, and BMI, for which median (interquartile range [IQR]) are also reported.
Reference group for calculation of odds ratio (OR = 1.00) is “No.”
Only “yes/no” diagnosis of endometriosis or fibroids will be included. Grade/subtypes will not be included.
Adenomyosis diagnosis
Adenomyosis can be diagnosed through imaging modalities (ultrasound or MRI) or by histopathologic evaluation of the uterus following hysterectomy. 20 Patients who developed BV were more likely to be diagnosed through imaging (both ultrasound and MRI) (52.8% and 45.8%, respectively, p < 0.01) compared to histopathologic evaluation of post-hysterectomy samples (1.4%) (Fig. 1A). This was significantly different compared to patients without BV, who had higher rates of diagnosis by pathological evaluation (56%, p < 0.001).
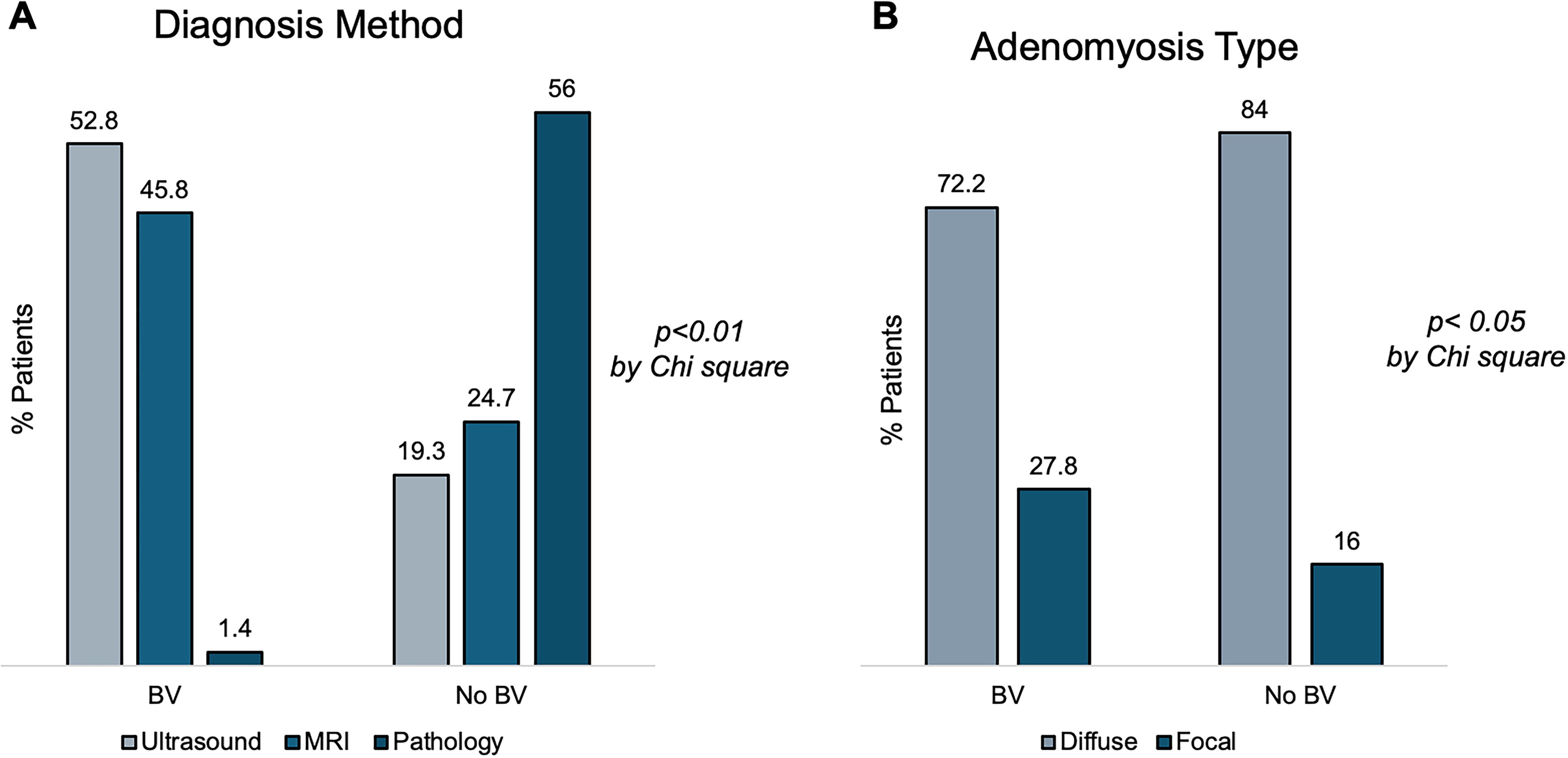
Methodology of Adenomyosis Diagnosis and Subtype.
Aside from differences in how adenomyosis can be diagnosed, there are different subtypes within the adenomyosis diagnosis. Adenomyosis can present as a diffuse subtype and a focal subtype 20 based upon involvement of the internal myometrium (diffuse) or sole involvement of the external myometrium with or without adenomyosis lesions (focal). Adenomyosis subtype was categorized as diffuse or focal based upon radiologic and histopathologic reports. A higher proportion of adenomyosis in patients with BV could be classified as focal compared to patients without BV (27.8% versus 16%) (p < 0.05, Fig. 1B). However, most cases that could be categorized were the diffuse subtype for both groups.
Symptomatology
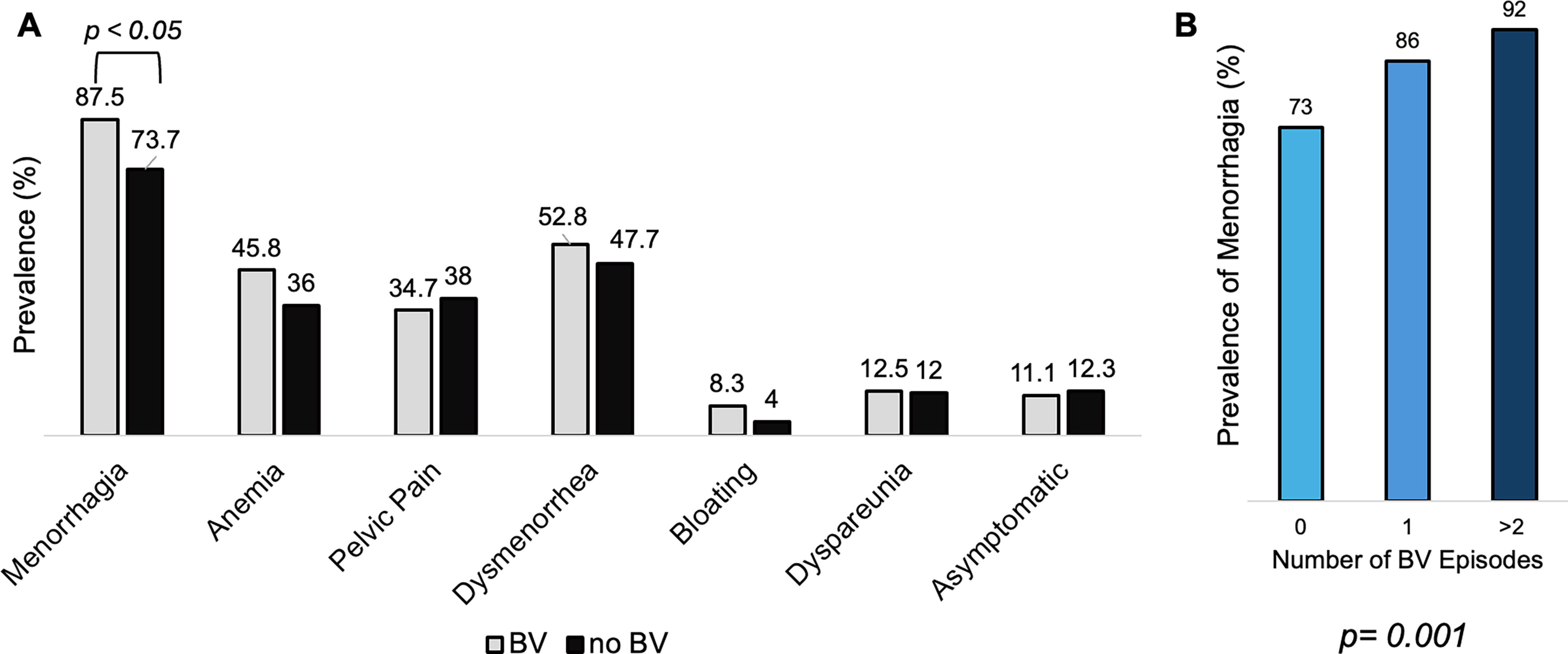
Since the method of diagnosis differed for patients who developed BV, we next sought to determine if there were differences in symptoms reported by patients at the time of adenomyosis diagnosis that were associated with the development of BV. Among patient self-reported symptoms, only menorrhagia was more likely to be reported by patients who subsequently developed BV within 3 years of their adenomyosis diagnosis (87.5% versus 73.7%, p = 0.014, OR 2.63 [95% CI 1.28–6.06] when adjusted for race/ethnicity and tobacco use) (Fig. 2A and Supplementary Table S2). However, the significant difference in reports of menorrhagia did not result in a significant difference in diagnosis of anemia between patients with or without BV.
Symptoms of Adenomyosis and Association with Bacterial Vaginosis.
Patients were then stratified into groups based upon the number of BV episodes following adenomyosis diagnosis (none, 1, or ≥ 2), and rates of reported menorrhagia were then compared between these groups. The prevalence of menorrhagia was positively associated with an increasing number of BV episodes (p = 0.001). Patients who experienced ≥ 2 episode of BV had the highest prevalence of reported menorrhagia (92%) (Fig. 2B). Patients with BV and menorrhagia had a range of 1–11 BV episodes in the 3-year-period after adenomyosis diagnosis (but prior to hysterectomy), whereas patients without menorrhagia had 1–4 BV episodes during this period. Six patients with menorrhagia and one patient without menorrhagia had more than 3 episodes of BV. While there can be differences in the symptomatology of adenomyosis at presentation between patients, data indicated that menorrhagia was associated with the occurrence of BV. These findings support the hypothesis that increased exposure to vaginal bleeding in AUB can predispose patients to BV.
Treatment of adenomyosis
Symptomatic treatment of adenomyosis involves addressing vaginal bleeding symptoms and dysmenorrhea/pelvic pain. Between patients who developed BV and those who did not, there was no difference in the use of medical treatment for pain symptoms (Supplementary Table S3). There are multiple treatments to address the abnormal uterine bleeding associated with adenomyosis. Some treatments involve exogenous hormones, such as oral combined oral contraceptives or progesterone formulations. Additional treatments involve gonadotropin-releasing hormone analogs, tranexamic acid, and aromatase inhibitors. There was a significant difference in the medical treatments used for adenomyosis-related bleeding between patients who developed BV versus those who did not (76.4% versus 52.5%, p < 0.001, Table 2). Patients with BV were more likely to receive medical treatment for bleeding symptoms compared to those who did not have BV (76.4% versus 52.5%, p < 0.001). Patients who had BV were more likely to use progestin intrauterine devices (33.3% versus 20%, p = 0.023) (Table 2).
Treatment of Vaginal Bleeding Associated with Adenomyosis
Adenomyosis may also be treated surgically with a hysterectomy, which should resolve both bleeding and most abdominal pain symptoms. Even though menorrhagia was the only significant difference in adenomyosis symptoms at the time of diagnosis for patients with BV versus those without BV, there was a difference in the rate of surgical intervention. Patients without BV were more likely to undergo hysterectomy compared to those who developed BV (12.5% versus 78.7%, p < 0.001) (Table 2). Regarding other gynecological surgical interventions, rates of myomectomies were also different between the two groups. Despite similar rates of fibroid co-diagnosis between the two groups (Table 1), patients who were later diagnosed with BV were more likely to undergo a myomectomy (11.1% vs 3.1%, p < 0.01) (Table 2).
BV treatment
Across all BV episodes, various treatments were used, including oral and vaginal metronidazole, clindamycin, and tinidazole (Supplementary Table S4). Most patients (N = 52, 72.2%) were prescribed oral metronidazole for treatment of the first BV episode after adenomyosis diagnosis (Supplementary Table S4). An extended metronidazole regimen for subsequent BV episodes was only prescribed for patients who had a history of menorrhagia. Oral clindamycin was also prescribed for patients with menorrhagia with >1 episode of BV. Oral metronidazole continued to be prescribed for patients after ≥3 episodes of BV.
Discussion
We observed significant differences in the diagnosis, symptomatology, and treatment of adenomyosis in patients who subsequently developed BV, compared to patients who did not develop BV following an adenomyosis diagnosis. Rates of menorrhagia were significantly higher in patients who developed BV as compared to patients who did not. Treatment for bleeding symptoms differed significantly between patients who developed BV compared to those who did not. These findings support the hypothesis that increased vaginal bleeding may predispose patients to the development of bacterial vaginosis. While there were differences in the treatment of bleeding symptoms, there were no differences in the treatment of the pain symptoms of adenomyosis. Considering these findings in the context of the changes in the vaginal microbiome with adenomyosis, 6,17,18 it appears that one cause of vaginal microbiome shifts reported in women with adenomyosis could be due to the increased exposure of abnormal uterine bleeding rather than intrinsic features of adenomyosis.
Of note, there were differences in the demographics between patients who developed bacterial vaginosis and those that did not (Table 1, p < 0.001). Consistent with previous literature, a large majority of patients with bacterial vaginosis identified as Black or African American. 2 Additionally, patients with BV had a younger median age compared to patients who did not develop BV (41 versus 45, p < 0.001) (Table 1). Despite the significant difference in age, both age ranges are pre-menopausal compared to the general population. Thus, hormonal changes and amenorrhea associated with menopause are unlikely to be a confounding variable between the differing rates of menorrhagia between patient groups.
In our study, patients with BV were more likely to be diagnosed with adenomyosis by radiological approaches, while patients without BV were more likely to be diagnosed by histopathologic evaluation of post-hysterectomy specimens. Multiple factors could account for the differences in diagnostic modality between these patient groups, including racial disparities in the evaluation and treatment of AUB, 21 differing symptoms and their impact on patients’ quality of life, and the equivocal nature of diagnosing adenomyosis. A likely explanation for this difference is the higher rate of menorrhagia in adenomyosis patients with BV, as compared to patients without BV. As part of the evaluation for abnormal uterine bleeding, affected patients may undergo laboratory tests and imaging to identify potential nonstructural and structural (such as adenomyosis) etiologies. 22 In our cohort, patients with BV had higher rates of AUB, likely prompting radiological evaluation that ultimately facilitated the diagnosis of their adenomyosis. Patients without BV had lower rates of AUB, potentially delaying their adenomyosis diagnosis until they underwent hysterectomy for myriad reasons.
Subtypes of adenomyosis have previously been demonstrated to correlate with bleeding profiles. Diffuse adenomyosis with involvement of the internal myometrium has been associated with heavy menstrual bleeding 23,24 when compared to adenomyosis that only impacts the external myometrium (i.e., focal adenomyosis). Given this known association, it was not surprising that a majority (72.2%) of patients who developed BV had diffuse adenomyosis involving the internal myometrium. However, it is of note that patients with BV had higher rates of focal adenomyosis (27.8% versus 16%). This may be a consequence of the high rates of radiographical diagnoses in the BV group that allowed for the assessment of established criteria for distinguishing between forms of adenomyosis. High rates of gross pathological examination in patients without BV may not have allowed for the sensitive detection of focal adenomyosis.
In comparing treatment approaches between the two patient groups, it was notable that patients with BV who had higher rates of menorrhagia also had high rates of receiving medical treatment for vaginal bleeding. Given that this group of patients experienced more abnormal uterine bleeding symptoms, higher rates of bleeding treatment use were expected. However, it was unexpected that patients with BV would be more likely to undergo a myomectomy compared to a hysterectomy—especially since there was not a significant difference in fibroid diagnoses between the two groups (Table 1). The significant differences in the rates of hysterectomies (12.5% in patients with BV vs 78.7% in patients without BV, p < 0.001) between the two groups could indicate different patient counseling among these two groups. The higher rates of medical treatment or surgical approach with myomectomy in patients with BV may be due to the racial differences between the two groups—such as the higher rate of Black patients in the BV group. There is substantial evidence in the literature that patients with Black racial identity have less access to minimally invasive hysterectomies. 25 Black patients who were more likely to develop BV may have been unable to access surgical treatment.
Data from this study demonstrates that factors present at the time of adenomyosis diagnosis (i.e., menorrhagia, ability to diagnose adenomyosis by imaging) are associated with at least one episode of BV infection within 3 years of adenomyosis diagnosis. Identification of these risk factors in patients may provide insight into why some patients are more likely to develop BV. While this study is the first to report an association between adenomyosis and BV, its design as a retrospective cohort study and sample size of 372 patients limits the in-depth characterization of this association. We were unable to make definitive conclusions regarding a reduction in BV episodes after hysterectomy, which would have theoretically removed the source of AUB, as only ten patients with BV after diagnosis underwent hysterectomy. Furthermore, comparisons between patients with BV who endorsed menorrhagia and those who did not were limited given the sample sizes (63 BV patients with menorrhagia, 9 BV patients without menorrhagia). Future prospective studies could standardize patient questionnaires and methods of diagnosis to eliminate variability that occurs with chart-review studies. Despite these weaknesses, this study helps to lay the foundation of introducing a new paradigm into the treatment of recurrent BV: addressing the underlying exposure of vaginal bleeding may address the vaginal dysbiosis predisposing patients to bacterial vaginosis.
Conclusions
Patients with a diagnosis of adenomyosis who developed BV experienced higher rates of menorrhagia and were less likely to undergo hysterectomy. While many patients receive a diagnosis of adenomyosis based upon pathological review following hysterectomy, patients with higher menorrhagia rates that subsequently developed BV were more likely to be diagnosed by radiological evaluation. Intrinsic characteristics of adenomyosis at the time of diagnosis (including diagnostic method) may be indicative of an increased likelihood to ultimately develop other gynecological conditions, including BV. The results from this study raise the possibility that modifiable risk factors, such as improvement of abnormal uterine bleeding with medical or surgical approaches, might reduce the incidence of BV in high-risk populations. Prospective studies are needed to further characterize the relationship of BV and vaginal dysbiosis with uterine pathologies leading to abnormal uterine bleeding.
Footnotes
Acknowledgments
The authors thank Dr. Satin and the Department of Gynecology and Obstetrics at Johns Hopkins University School of Medicine for their support of the Core for Clinical Research Data Acquisition (CCDA) EPIC Data Core.
Authors’ Contributions
A.N.V.-S.: Methodology, investigation, visualization, data curation (equal), writing—original draft (equal), writing—review and editing (equal). A.Z.: Methodology, investigation, visualization (supporting), data curation (equal), writing—original draft (equal), writing—review and editing (equal). Y.W.: Formal analysis. M.R.J.: Formal analysis (lead). S.O. and K.V.: Formal analysis. M.B.: Data curation. A.M.P.: Writing—review and editing (supporting). B.S.: Conceptualization, methodology, supervision, project administration, writing—review and editing (supporting). J.H.S.: Conceptualization, supervision, resources writing—review and editing (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported, in part, by the Howard and Georgeanna Jones Endowment.
Supplementary Material
Supplementary Tables
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.