
Abstract
Background:
Chlamydia trachomatis (CT) infections are among the most prevalent sexually transmitted infections (STIs), particularly affecting young adults. In women, CT can cause pelvic inflammatory disease, infertility, and ectopic pregnancy, justifying routine vaginal swab screening. However, due to diverse sexual practices, CT can colonize multiple anatomical sites, including the pharynx. Pharyngeal CT carriage in women is underdiagnosed and may contribute to ongoing transmission.
Objectives and Methods:
This study aimed to assess the rate of pharyngeal CT carriage, describe the rate of isolated pharyngeal CT carriage, and identify factors with pharyngeal CT carriage. We conducted a retrospective study at Montpellier University Hospital (France) and the public STI clinic of the city, including all cisgender women who provided at least one pharyngeal sample for CT testing between May 1st, 2018, and June 30, 2023.
Results:
A total of 567 women (median age 24 years) contributed 666 samples. Pharyngeal CT carriage was found in 2.8% of the population. Most cases were concurrent with vaginal CT, but 5 women had isolated pharyngeal carriage, representing 0.9% of the study population and accounting for 11.1% of detected cases. Young age and a history of CT infection appeared to be independently associated with pharyngeal CT carriage in multivariate mixed model analysis.
Conclusion:
We observed a pharyngeal CT carriage rate consistent with the literature, which was low but not insignificant. Notably, 11.1% of CT infections would have been missed without pharyngeal screening, underscoring the importance of considering extragenital testing.
Introduction
Chlamydia trachomatis (CT) is one of the most common bacteria responsible for sexually transmitted infections (STIs), particularly among young adolescents and adults. 1,2 In 2020, the worldwide incidence of new CT infections was 129 million annually. 1 In France, in 2021, screening for CT infections led to the diagnosis of nearly 120,000 infections. 3 Occitanie is one of the regions with the highest positivity rate in France. 4 The epidemiological control and screening of these infections represent a major public health challenge, both for the quality of life of patients and to potentially reduce healthcare costs associated with complications. The Haute Autorité de Santé (HAS) recommends systematic screening for sexually active women aged 15 to 25 years. 2 More broadly, screening is recommended for sexually active individuals or in certain at-risk situations. 2,5 In France, screening is typically performed via vaginal swabs in women 2 and the reference detection method is nucleic acid amplification testing (NAAT). 2,6,7
Extragenital sites appear to contribute to the human-to-human transmission of CT, partly through oro-genital intercourse, which is rarely protected by condoms. 8 Furthermore, extra-genital infections are often asymptomatic. 9 –11 Pharyngeal and rectal swabs for CT and Neisseria gonorrhae (NG) are part of STI screening in men who have sex with men (MSM) in most developed countries, based on their sexual practices. 6,12,13 However, in heterosexual women or men, pharyngeal or rectal sampling is not based on official recommendations but rather on local practices, often on a case-by-case basis. The transmission of CT during oro-genital intercourse is well documented: from the female pharynx to the male urethra, 14,15 from the vagina to the male pharynx, and also through the proximity of the vagina to the anus in women. 15 –17
Many studies have sought to evaluate the relevance of screening for extra-genital CT infections in women over several decades, in different countries and among different, noncomparable populations. 17 –21 Only a few studies have focused more specifically on the impact of routine pharyngeal CT screening in women; a recent Dutch retrospective cohort study conducted in a population of asymptomatic women found a 2.4% carriage rate of pharyngeal CT and 0.5% with the pharynx as the only infected site, which did not allow the establishment of an optimal screening algorithm. 22 Most studies conclude that there is insufficient solid data or extrapolable results to justify the benefits of universal pharyngeal screening in women, either for individual or public health, and such screening is therefore not recommended. However, literature reviews published in 2016 and 2022 draw discordant conclusions regarding the value of pharyngeal screening in women. 10,12 In this context of incertitude and in the absence of evaluation of the benefit of such screening in France, we aimed to assess the relevance of a screening strategy combining pharyngeal and vaginal sampling in women consulting at the Montpellier University Hospital, including the city public STI clinic.
Patients and Methods
We conducted a monocentric, observational retrospective study at the University Hospital (CHU) of Montpellier, France, including the public STI clinic (CeGGID). All adult (≥18 years) cisgender women who provided at least one pharyngeal sample for C. trachomatis testing between May 1st, 2018, and June 30, 2023, and did not oppose the use of their data were included. Repeated sampling was allowed if samples were collected at least 6 weeks apart or if sexual risk-taking behavior was documented in between. As per French law on retrospective studies using anonymized data collected during routine care, no express written consent was required. All patients were informed through institutional communication materials and could refuse participation (opt-out process). Only data from patients who did not object were included. The study was approved by the Montpellier CHU Institutional Review Board (IRB-MTP_2023_05_202301418).
All specimens were tested by NAAT Aptima Combo 2 using the Panther Fusion® (Hologic, Inc.) instrument during the study period. Concomitant specimens of other sites (rectum, urine, or vaginal) were collected, as well as sociodemographic data (age, birth country), history of sexually transmitted infection (HIV, HBV, HCV, syphilis, CT), sexual behavior (sexual orientation, sexual practices, sex work, number of partners during the last 12 months), condom and contraceptive use, screening indication, and presence of symptoms. The primary judgment criterion was the rate of pharyngeal CT carriage. Secondary judgment criteria included the rate of pharyngeal-only CT carriage (i.e., if urine/vaginal and/or rectal specimens tested negative) and factors associated with pharyngeal CT carriage. Quantitative variables were described by their median and interquartile range (IQR) and compared using the Wilcoxon-Mann-Whitney test (normality assumption was not verified). Binary or qualitative variables were described by effectives and percentages and compared using χ2 or Fisher’s exact test when appropriate. Association of pharyngeal CT carriage with covariates was assessed using mixed logistic univariate and multivariate models to account for the panel data owing to the repeated and unbalanced testing in individuals and the possibility that the covariates varied in between visits. All tests were bilateral, and the alpha level was set at 0.05. Analyses were performed using Stata BE 18.0 (Stata Corp, TX, USA).
Results
A total of 765 samples met our inclusion criteria, including 552 from CeGIDD and 213 from other hospital departments. We excluded 71 samples from transgender individuals, 16 samples collected ≤6 weeks to a previously included sample without new risk exposure, and 12 samples from participants whose electronic medical records were unavailable.
Description of the study population (Table 1)
A total of 567 participants with a median age of 24 years (interquartile range [IQR]: 21–31) were included in the study. Most women had only one visit (n = 507, 89.4%), but 22 (3.9%) had ≥3 visits, contributing to a total of 666 samples. For participants who were born outside of France (n = 120, 21.2%), the sample was drawn <6 months after arrival in France for n = 16/92 (17.4%), between 6 and 12 months for n = 7/92 (7.6%), ≥12 months for n = 69 (75.0%), and the information was missing for n = 28.
Characteristic of Participants at First Testing
One participant reported no sexual partner in the last 12 months.
HIV, human immunodeficiency virus; HBV, hepatitis B virus; HCV, hepatitis C virus; PrEP, pre-exposure prophylaxis; BDSM, Bondage, Discipline, Domination, Submission, Sadism, Masochism; PEP, post-exposure prophylaxis.
Participants had a history of previous CT infection in 20.4% of cases (n = 85/416) (20.4%) with a vaginal carriage involved (n = 49/49, 36 missing), of syphilis for 0.9% (n = 5/559), of HIV infection for 2.2% (n = 12/559), of HBV for 2.2% (n = 12/559), and of HCV for 0.9% (n = 5/559). The median number of sexual partners over the past 12 months was available for n = 339/567 individuals and was 4 (IQR: 2–8, range: 0–100). Participants reported sexual intercourse with males (n = 323, 95.3%), females (n = 90, 26.5%), or transgender partners (n = 5, 1.5%). Systematic condom use with casual partners was reported by 44.0% of participants for vaginal intercourse, 36.8% for anal intercourse, and 3.6% for oral sex.
The use of psychoactive substances (alcohol, drugs) in a sexual context was reported by n = 12/320 participants (3.8%), and n = 44/426 had a history of sex work (10.3%). High-risk sexual behaviors (Bondage, Discipline, Domination, Submission, Sadism, Masochism [BDSM], and group sex) and a history of non-consensual sexual intercourse were poorly documented; nevertheless, they were reported by n = 27/148 (18.2%) and n = 88/158 cases (55.7%) of participants, respectively. Eight out of 559 (1.4%) participants were on or had been on HIV pre-exposure prophylaxis (PrEP). Contraception (either long- or short-acting) was used by 52.8% (235/445) of concerned participants.
Microbiological results
On first testing, 38 participants had CT carriage at least at one site, including n = 12/567 for the pharyngeal site (2.1%), n = 35/535 (6.5%) for the vaginal site, and n = 8/127 (6.3%) for the anal site. The pharynx was the only site involved for n = 5, the vagina for n = 22 participants, and the rectum for 1 participant (Fig. 1A).
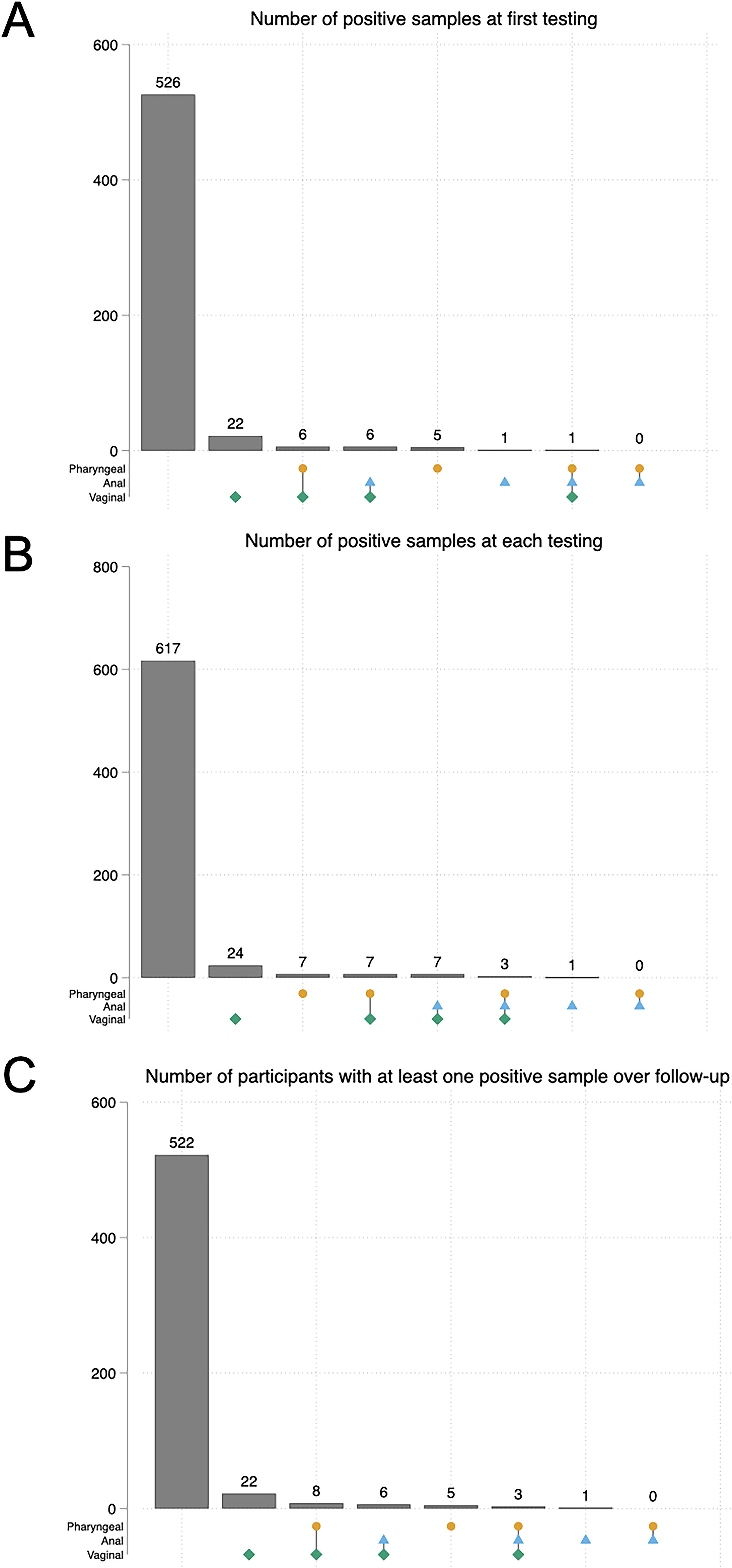
UpSet Plot showing the intersection of positive samples on the pharyngeal, anal, and vaginal sites
Including repeated pharyngeal samples led to 17/666 (2.6%) positive samples in 16 (2.8%) different participants (12 at first testing, 4 at second testing, and 1 at fifth testing). The participant with repeated positive samples was positive on her second and fifth testing. Similarly, 11/180 (6.1%) positive rectal samples were detected in 10 participants over a total of 135 participants who had at least one testing, and 41/630 (6.5%) positive vaginal samples (39/583 vaginal swabs, 3/63 urine samples, and 1/16 on both) were detected in 39 participants (2 women had 2 positive samples) over a total of 537 participants who had at least one testing.
All 17 positive pharyngeal samples were paired with vaginal swabs simultaneously, with 10/17 testing positive (59%). In seven cases (41%), anal samples were also collected, 3 (43%) of which were positive for CT. When considering all available testing, 45 women were found to carry CT at least one time. Among the latter, 5 (11.1% of all infections, 0.9% of the study population), 1, and 22 never had another site positive but the pharyngeal, anal, and vaginal sites, respectively; 8 (17.8%) had pharyngeal and vaginal, 6 (13.3%) had anal and vaginal, and 3 (6.7%) had pharyngeal, anal, and vaginal positive samples. All but 1 participant with positive anal CT carriage also had vaginal CT carriage (Fig. 1B and C).
Symptoms were present in 76 participants (76/655; 11.6%), including 17 (22.7%) with pharyngeal symptoms, 6 with both pharyngeal and vaginal symptoms (8.0%), 49 (65.3%) with vaginal symptoms, and 3 (4.0%) with anal symptoms. The most frequent symptoms were inflammation (29, 38.7%), unusual leucorrhea (16, 21.3%), dolor (7, 9.3%), burning sensations (6, 8.0%), metrorrhagia, unpleasant vaginal odor, pruritus (5 for each category, 6.7%), and discharge (2, 3.7%). Symptoms were present in 11.4% (n = 73/638) of episodes with negative pharyngeal testing and in 17.7% (n = 3/17) with positive pharyngeal samples. In the three latter women, symptoms were reported as vaginal, and only one participant tested positive at the vaginal site (she described metrorrhagia). All the participants reporting pharyngeal symptoms had negative pharyngeal testing.
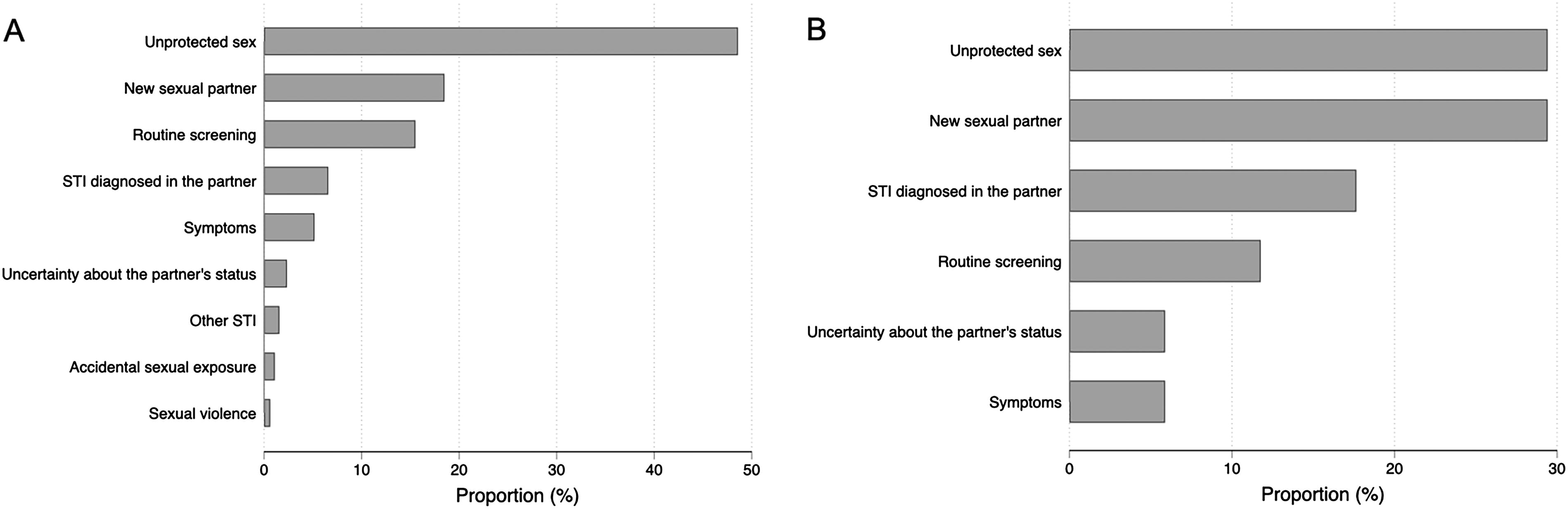
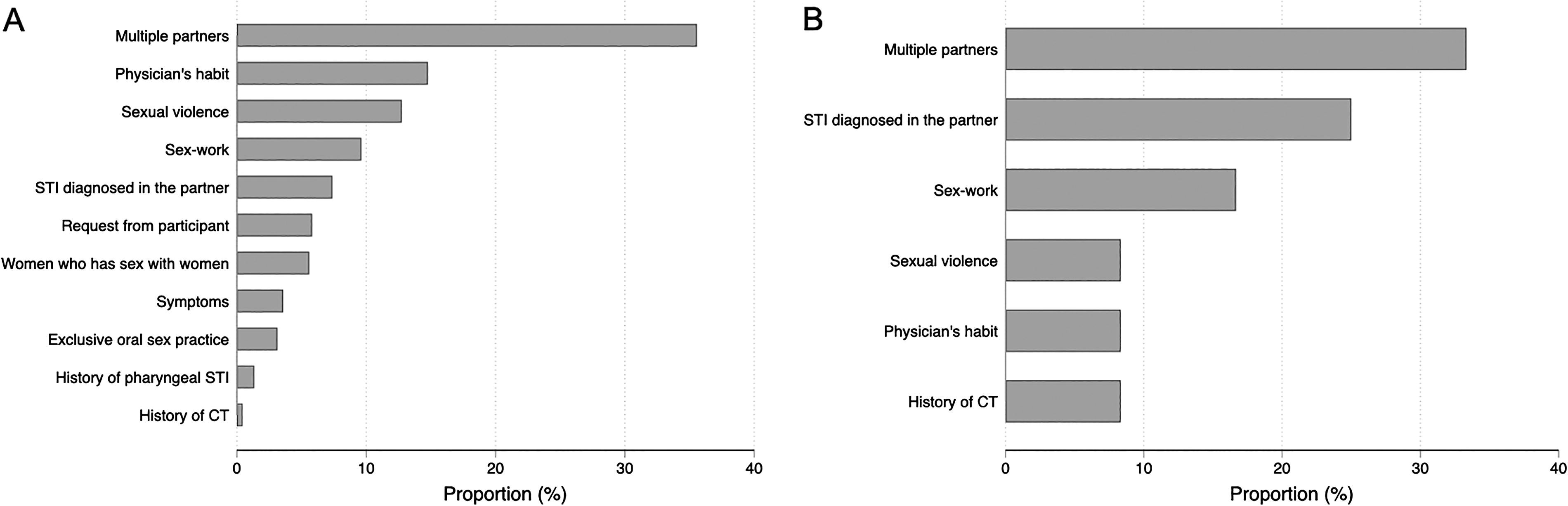
Screening context was identified in 655/666 samplings; it was mainly unprotected sexual intercourse (315/655; 48.1%), routine screening (101/655; 15.4%), and a new sexual partner (66/655; 10.1%) (Fig. 2). Overall, screening context did not differ significantly depending on pharyngeal testing status (χ2 test, p = 0.430). The reasons for pharyngeal sample collection were documented in 459 cases: primarily in participants with multiple partners (163/459; 35.5%), physician’s habit (67/459; 14.6%), or following sexual violence (58/458; 12.7%), sex work 45/459 (9.8%), or STI in sexual partner (36/459, 7.8%) (Fig. 3). Reasons were different depending on pharyngeal testing status (χ2 test, p = 0.038), and positive results were more likely seen in the presence of STI in the partner, sex work, previous CT. Specifically, among the 7 episodes of isolated pharyngeal CT carriage (considering repeated testing), 5 occurred in participants with potential indications for pharyngeal screening. Notably, 4 of them had a personal history of CT infection (n = 4): one also had a new sexual partner, one reported unprotected sex, one had a partner diagnosed with an STI, and one underwent routine screening. Another participant was tested in the context of sexual violence. The remaining two participants had no formal indication apart from physician habit; one reported unprotected sex, and the other presented with unspecified vaginal symptoms.
Motives of C. trachomatis screening for patients with
Motives of specific C. trachomatis pharyngeal testing with
Factors associated with pharyngeal positive CT testing
In univariate analysis (Table 2), the median age of participants with pharyngeal positive C. trachomatis testing was 21 years (IQR: 20–22.5), significantly lower than the population without pharyngeal CT carriage, whose median age was 24 years (IQR: 21–31, OR = 0.83, 95%CI: 0.71–0.96, p = 0.013). Four participants (25.0%) were born outside mainland France (3 in sub-Saharan Africa and 1 in Western Europe), which was not statistically different from the whole population. Among all cases, one reported a history of syphilis, and none reported HIV, hepatitis B, or hepatitis C infection. However, 5 (35.7%) of the participants reported a prior history of CT infection, a rate significantly higher than that of participants without pharyngeal CT carriage (19.7%, OR = 3.48, 95%CI: 1.25–9.64, p = 0.016). Condom use was reported by 1 out of 15 participants (6.7%), as opposed to 14/405 (3.5%) in participants without pharyngeal CT carriage, without statistical difference (p = 0.423). Three out of 15 cases (20.0%) reported engaging in sex work. Similarly to the findings from univariate analysis, in multivariable analysis only age and a history of CT infection were associated with pharyngeal CT carriage, with aOR = 0.81 (95%CI: 0.69–0.96, p = 0.012) and aOR = 4.04 (95%CI: 1.46–11.35, p = 0.007), respectively.
Univariate and Multivariate Analysis of Factors Associated with Pharyngeal C. trachomatis Carriage
CT, Chlamydia trachomatis; HIV, human immunodeficiency virus; HBV, hepatitis B virus; HCV, hepatitis C virus; PrEP, pre-exposure prophylaxis; BDSM, Bondage, Discipline, Domination, Submission, Sadism, Masochism; PEP, post-exposure prophylaxis.
Discussion
In our study, we aimed to retrospectively analyze the pharyngeal carriage of CT and the relevance of its screening in women. We found a pharyngeal carriage rate of CT of 2.8% over the whole follow-up, which is similar to what is reported in the literature. 20,22 –24 The pharynx as the only infected site was found in 0.9% of the studied population, accounting for 31% of the pharyngeal carriage cases, which is slightly higher than what was described by the Dutch team. 22 A significant amount (11.1%, 5/45) of CT infections in this population would not have been diagnosed if the pharyngeal sample had not been performed. When considering also rectal samples, this proportion increases to 16.3%. Pharyngeal carriage was always asymptomatic, as shown previously. 9,10,17,25 Of note, among the 7 episodes of isolated pharyngeal CT carriage, only 2 occurred in women without a documented specific indication for pharyngeal screening at the time of testing, highlighting the limited potential yield of universal screening in this population.
A younger age, concomitant infections, the number of sexual partners, and a history of exposure to an infected partner are the most frequently cited characteristics in the literature as being associated with extra-genital CT carriage in women. 15,22,23,26 A recent study found irregular condom use and HIV co-infection as risk factors, but considering both pharyngeal and rectal carriages. 11 We also found that a younger age (21 vs. 24 years as median age) seems to be a risk factor for pharyngeal CT carriage, although the clinical relevance of this difference is debatable. Furthermore, a history of CT infection appears to be significantly more common among cases with pharyngeal CT carriage (35.7% vs. 19.7%), which, to our knowledge, had not been described until now. This last finding could reflect a more active, varied sexual life, which would increase the risks of carriage. We might also hypothesize a poorer knowledge of prevention methods regarding STI recurrence or an inadequate eradication of the previous carriage.
Moreover, although the tested population is at higher risk for STIs, we observed that the profile of participants with CT pharyngeal carriage does not have any other specific characteristics regarding number of sexual partners, history of STIs, history of HIV, HBV, or HCV infection, syphilis, or PrEP use compared to those participants without pharyngeal CT carriage.
The population in our study consists of individuals consulting at a public STI clinic or at the University Hospital, which is the main hospital of the city, primarily in the infectious and tropical diseases department. We found a non-negligible number of participants with a history of STIs and nonconsensual sexual encounters and, to a lesser extent, those using PrEP or engaging in substance use in sexual contexts. Our study supports the finding that oro-genital intercourse is seldom protected by a condom. 8 We also observed CT carriage in individuals who reported using a condom systematically, whether for oral sex or for vaginal intercourse, highlighting the various routes of transmission. 16 It should be noted that CT transmission has not been documented through exclusively oral contacts, in contrast to Neisseria gonorrhoeae. 27,28
Based on all these data, it seems plausible that pharyngeal carriage plays a role in the transmission of CT. However, its pathogenicity and natural history are not fully elucidated. 29 Spontaneous clearance of CT at the pharyngeal level appears to exist, 23,30 primarily for exclusive pharyngeal carriage due to a lower bacterial load. Once again, the studies conducted have not established the relevance of pharyngeal screening in women.
Despite a substantial number of inclusions, our study has limitations, primarily related to the fact that it is a retrospective study subject to various biases. Patient declarations may also be erroneous. We also lacked information on recent or ongoing antibiotic therapy. For some criteria, missing data were also too numerous to allow for statistical significance, and the small number of cases likely resulted in insufficient power to identify certain associations, such as with the number of partners, despite a noticeable trend. Furthermore, our study is monocentric and concerns a population potentially at higher risk for STIs seeking care at a public STI clinic or in the infectious diseases department, which limits its external validity and extrapolation to the general population. Therefore, our pharyngeal CT carriage rate may have been overestimated compared to the general population but likely reflects the level of women consulting in those settings. Additionally, a substantial part of the study period coincided with the COVID-19 pandemic, during which access to STI screening was reduced due to national lockdowns and the reorganization of health care services. This was particularly evident in 2020, which included two lockdown periods. These disruptions likely limited the number of individuals tested and may have influenced both screening indications and case detection, potentially introducing a slight selection bias.
Given these findings, we believe that it is not relevant to screen women at the pharyngeal site based solely on risk factors such as a history of STIs or the number of sexual partners but rather based on the presence of a CT history, regardless of the affected site, and younger age. We assume that the burden associated with the potential complications of a CT infection will be carried mostly by women. We also observe that, given the evolution of sexual practices in young adults, oral intercourses seem to be frequent and is often unprotected. It thus appears necessary to consider this pharyngeal carriage, which could be a key element in broader sexual health prevention, particularly among young women. Despite a slight increase during the study period, pharyngeal screening for CT remained marginal. To establish its relevance, a prospective study with systematic pharyngeal sampling and standardized data collection is needed and should consider different settings to assess its relevance, such as the general population consulting general practitioners or individuals attending specialized STI clinics. Key objectives include identifying high-risk groups, evaluating spontaneous clearance, and assessing prior CT carriage or infection. A cost-effectiveness analysis would also be essential to determine the feasibility of large-scale implementation.
Footnotes
Acknowledgments
The authors thank the physicians involved in the follow-up of the patients in the study.
Data Availability
Authors’ Contributions
E.B. and C.P.: Conceptualization; C.B.: Methodology, software, validation, formal analysis, E.B.: Investigation, project administration; E.B. and C.B.: Visualization, supervision, writing—original draft preparation, data curation; All authors: writing—review and editing. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work did not receive specific funding. C.B. is the recipient of a grant from the Bettencourt-Schueller Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.