
Abstract
Abstract
Lumbocostovertebral syndrome is the association of a congenital lumbar hernia with rib and vertebral anomalies. We report the first case of a laparoscopic repair of a lumbar hernia in a child with lumbocostovertebral syndrome. Laparoscopic lumbar hernia repair appears to be safe and feasible in children.
Introduction
Case Report
A 6-week-old term female infant presented to the Pediatric Surgery department with a right-sided lumbar hernia. The antenatal course for both mother and fetus was normal. Clinically, the hernia defect was bounded by ileocostalis muscle posteriorly, the costal margin superiorly, extending almost to rectus abdominus anteriorly, and to just above the iliac crest inferiorly, and contained the liver and bowel. The hernia protruded with abdominal straining and reduced spontaneously. An accessory nipple 3 cm below the right nipple was noted.
Ultrasonography revealed a 4-cm lateral abdominal wall defect. Chest and spine radiography demonstrated abnormalities of the right fifth to ninth ribs, an absent right tenth rib, an abnormal ninth thoracic vertebra with a dextroconvex thorocolumbar scoliosis (Fig. 1). Magnetic resonance imaging revealed a tethered cord with the conus at L2. At age 24 months, the tethered cord was released because of progressive kyphoscoliosis.
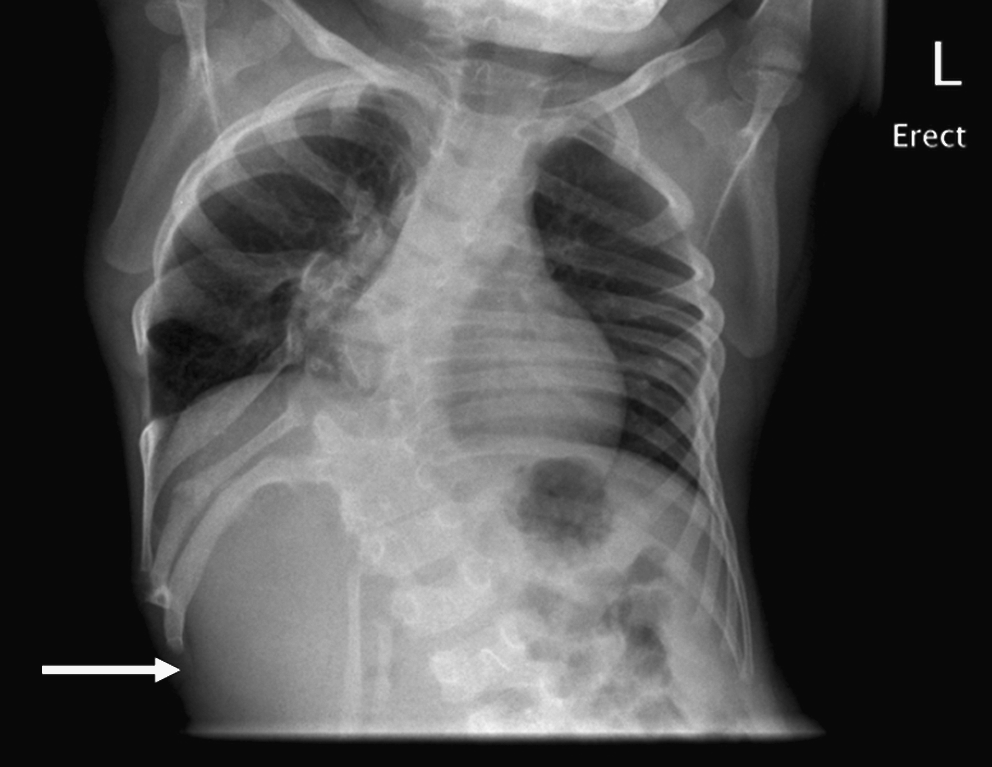
Chest radiograph demonstrating deformed ribs and scoliosis. The hernia protruded through the defect below the ninth rib (arrow), but was spontaneously reducing, so is not visible here.
At 31 months of age, the lumbar hernia was repaired laparoscopically via a 10-mm umbilical port and two 3-mm ports (both left sided along the midclavicular line, in the upper and lower quadrants). A peritoneal flap was raised, and a sheet of collagen biomatrix (Surgisis® Gold™; Cook Biotech Incorporated, West Lafeyette, IN) was secured to the edges of the defect with 4.0 braided polyester sutures. The hernia defect appeared to be bounded by the deformed ribs superiorly, the ribs and lumbar fascia posteriorly, and internal oblique muscle inferiorly. The peritoneal flap was replaced to leave the patch in a retroperitoneal plane and the peritoneum closed with 2.0 Ethibond sutures (Ethicon, Somerville, NJ) (Fig. 2). For cosmetic purposes, the accessory nipple was excised. Recovery was uncomplicated, and she was discharged on postoperative day 3. On follow-up at 12 months, there was no recurrence and a pleasing cosmetic result.

Laparoscopic view of repair after replacing a peritoneal flap. The liver is visible in the lower right corner of the image.
Discussion
The lumbar hernia was first described in an adult in 1731. 3 Petit described the inferior lumber triangle in 1733, 4 and Grynfelt described the superior lumbar triangle in 1866. 5 The inferior lumbar triangle of Petit is bounded by latissimus dorsi, external oblique, and the iliac crest. The superior lumbar triangle of Grynfelt is bounded by quadratus lumborum, internal oblique, and the twelfth rib. Touloukian, in 1972, described a female infant with bilateral lumbar hernias, hemivertebra at multiple spinal levels, thoracolumbar scoliosis, and deformed lower ribs, thus introducing the term lumbocostovertebral syndrome. 1 The defect in the present case was diffuse, but the boundaries conformed roughly to the superior lumbar triangle. The debate of open versus laparoscopic repair of lumbar hernias in adults is ongoing. A recent review suggests that for small or moderate defects, the laparoscopic approach seems best, while open surgery should be used for large defects and in cases where the laparoscopic approach has failed. 6
Conclusions
In conclusion, a lumbocostovertebral should be considered in infants presenting with a lumbar hernia and with chest and thoracolumbar spine radiographs performed. Children with lumbocostovertebral syndrome require multidisciplinary input from pediatric surgery, pediatric orthopedics, and neurosurgery. Laparoscopic lumbar hernia repair appears to be safe and feasible in children.
Footnotes
Disclosure Statement
No competing financial interests exist.